
Abstract
We report a unique case of a patient presenting with histologically confirmed pseudoxanthoma elasticum–like phenotype and cutaneous polyarteritis nodosa. Cardiac, gastroenterological, and ophthalmologic evaluations were within normal limits. Genetic evaluation was pertinent for absent ABCC6, ENPP1, and GGCX mutations and a normal array comparative genomic hybridization. Extensive workup revealed skin-limited cutaneous polyarteritis nodosa, and further genetic testing for ADA2 deficiency was negative. The cutaneous polyarteritis nodosa lesions had an excellent response to hydroxychloroquine and methotrexate. Pseudoxanthoma elasticum and polyarteritis nodosa are relatively uncommon, and our patient is among the first reported cases presenting with both pseudoxanthoma elasticum–like and polyarteritis nodosa. Furthermore, this case emphasizes the importance of a thorough cutaneous exam, as the patient had the lesions consistent with pseudoxanthoma elasticum–like since childhood and had previously gone undiagnosed.
Keywords
Introduction
We report a unique case of a patient presenting with pseudoxanthoma elasticum (PXE)-like phenotype and cutaneous polyarteritis nodosa (PAN). Both PXE and PAN are relatively uncommon, and our patient is among the first reported cases presenting with both PXE-like and PAN. This case highlights a possible new association and further characterizes these rare entities. 1
Case report
A 36-year-old woman presented with a 4-month history of progressive, ulcerating plaques on both legs. One month prior to the onset of her rash, she noted bilateral swelling and decreased range of motion of her hands and feet.
The physical examination confirmed these findings and also revealed bilateral pitting edema of lower limbs. Her cutaneous examination revealed multiple indurated plaques with central ulceration on both legs (Figure 1(a)). There was no palpable purpura nor livedo reticularis. Coincidentally, she was also noted to have multiple yellowish papules diffusely scattered on the posterior neck (Figure 2(a)). These lesions were present since childhood. Her family history was unremarkable, and she denied any cardiac or ophthalmologic symptoms.
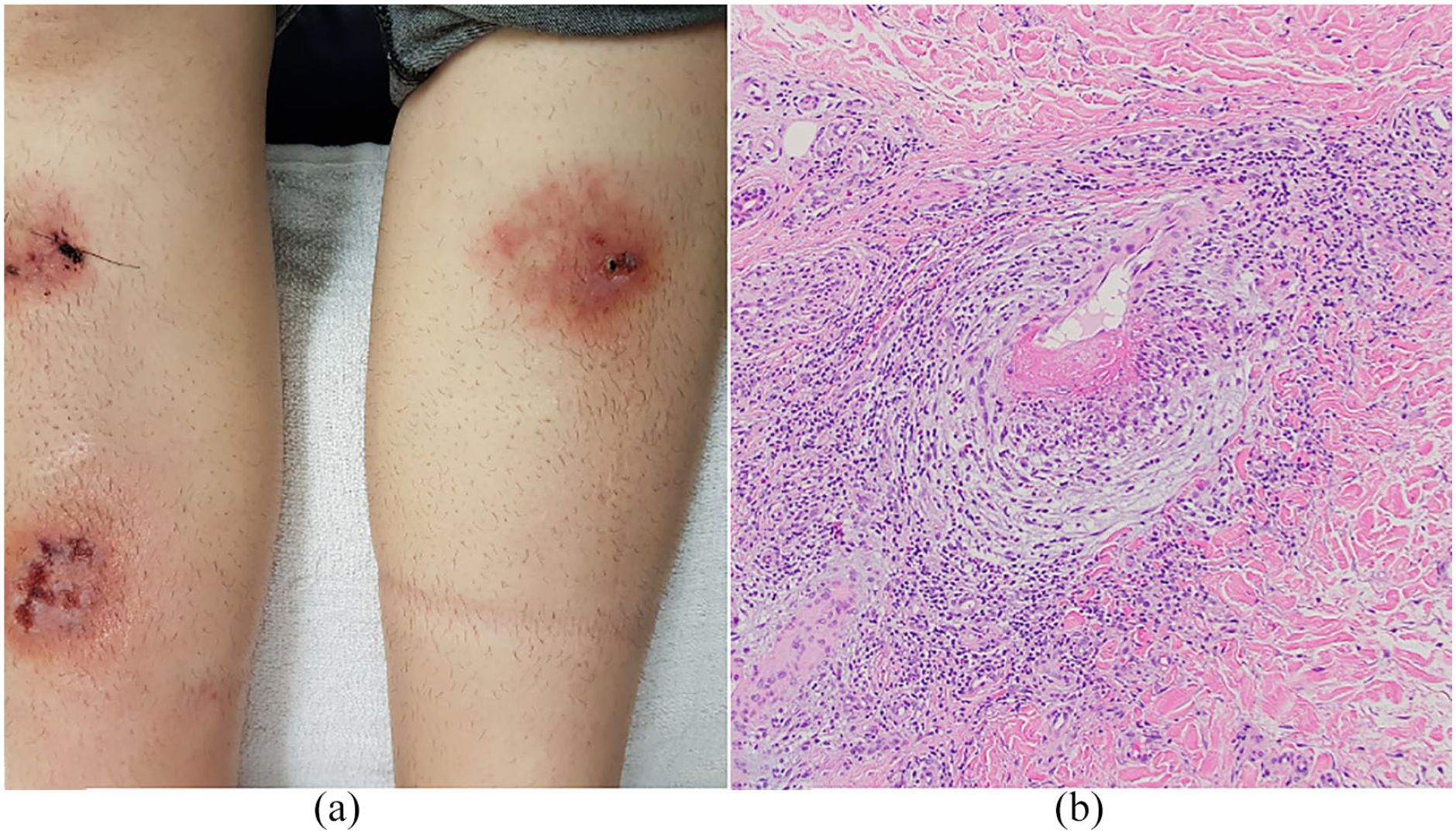
(a) Erythematous plaques with central ulceration on both legs. (b) Skin biopsy of the border of an ulcer. In the deep reticular dermis, there is a medium artery with prominent fibrinoid necrosis and inflammation, consistent with a necrotizing arteritis (hematoxylin–eosin stain; magnification ×100).
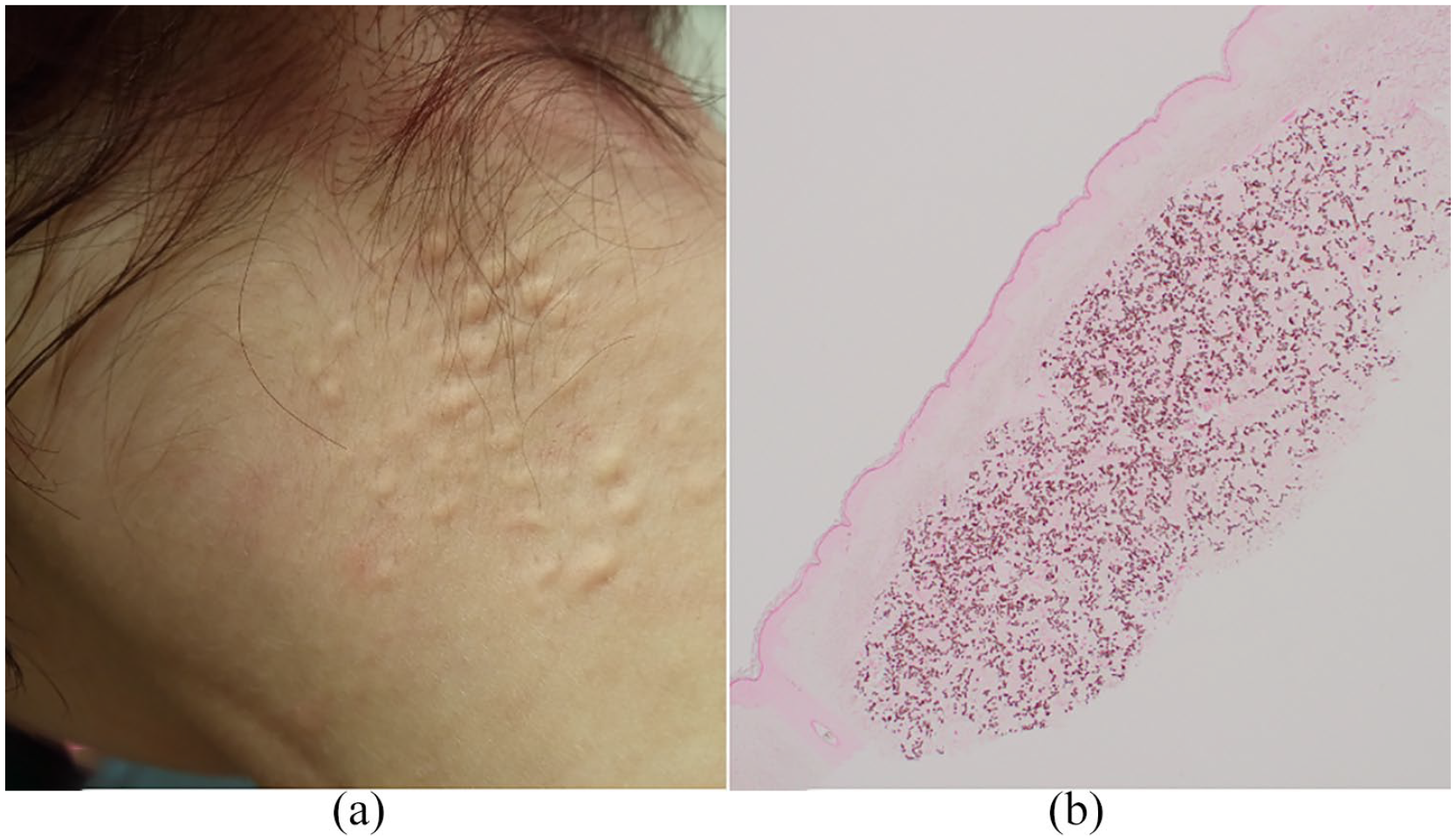
(a) Multiple yellowish papules on the posterior neck. (b) Skin biopsy of the yellowish papules on the posterior neck shows pseudoxanthoma elasticum–like calcification of the elastic fibers (Von Kossa stain; magnification ×40).
The patient did note polyarthralgia of her hands and ankles, and tenderness of the right Achilles tendon. She also noted paresthesia of her feet. A musculoskeletal (MSK) ultrasound of her hands, wrists, ankles, and feet showed no synovitis. X-ray imaging of the affected joints showed no erosions.
Her past medical history is significant for intellectual disability and a seizure disorder, both sequelae of an episode of meningitis as a child. Her medications at the time of presentation included levetiracetam, dilaudid, levonorgestrel-releasing intrauterine system, and acetaminophen. Her medications were long-standing, and there were no recent changes.
Her laboratory investigations included a normal complete blood count, normal mean corpuscular volume, normal renal function, normal liver profile, normal coagulation profile, and normal urine analysis. Her antinuclear antibodies, extractable nuclear antigen antibodies, lupus anticoagulant antibodies, and antineutrophil cytoplasmic antibodies (ANCA) serologies were negative. Hepatitis B, Hepatitis C, and HIV serologies were negative, and QuantiFERON-TB Gold was negative. Computerized tomography (CT) of the chest, and CT angiogram of the abdomen, and pelvis were unremarkable.
A biopsy at the border of the ulcer revealed a necrotizing medium vessel arteritis present in the dermis most suspicious of PAN (Figure 1(b)). Furthermore, she was seen by rheumatology who found she had no signs of systemic vasculitis particularly given the normal CT angiogram and MSK ultrasound showing no synovitis. Her presentation was consistent with limited or cutaneous PAN, and thus she was started on oral prednisone with the addition of celecoxib. She initially responded well to prednisone with almost complete resolution of her pretibial lesions. However, upon tapering the prednisone, her lesions recurred and she has since been maintained on hydroxychloroquine and methotrexate with excellent control.
In addition, her neck lesions were suspicious PXE, and thus one of the papules was biopsied. The biopsy showed clumped elastic fibers in the mid and deep reticular dermis suggestive of PXE. Von Kossa stain highlighted the clumped elastic fibers (Figure 2(b)).
Given the suspicion of PXE, she underwent cardiac, gastroenterological, and ophthalmologic evaluations which were within normal limit. Genetic testing for mutations associated with PXE was normal including an absence of ABCC6, ENPP1, and GGCX mutations. Furthermore, genetic testing for CECR1 mutations, which has been reported with PAN, was also normal. 2 The patient also has a normal array comparative genomic hybridization (CGH). Thus, the cutaneous findings were most in keeping with PXE-like phenotype.
Discussion
PAN is a vasculitis characterized by the involvement of medium-sized arteries. In a large retrospective study, 50% of patients diagnosed with PAN had cutaneous involvement, which included palpable purpura, livedo reticularis, inflammatory retiform purpura, and punched-out ulcers. 3 However, only about 10% of patients with PAN have limited, meaning limited to the skin, PAN. 3 Cutaneous PAN can also have extra-cutaneous manifestations including the symptoms often found in classic PAN such as constitutional symptoms, myalgia, arthralgia, and neuropathy. 4 Despite the systemic symptoms in cutaneous PAN, these patients do not have any evidence of organ involvement other than the skin. For cutaneous PAN, the course of the disease is chronic and relapsing. Furthermore, in a study of 21 patients with cutaneous PAN, with a follow up of 17 years, only 2 patients ultimately progressed from cutaneous-limited disease to systemic disease. 5 Homozygous or compound heterozygous pathogenic variants of the ADA2 gene (also called CECR1) result in a deficiency of adenosine deaminase 2 has been associated with early onset of PAN. 2 Genetic testing in our patient did not reveal a pathogenic mutation of ADA2. Our patient has not shown clinical signs of systemic PAN disease but has required long-term treatment with hydroxychloroquine and methotrexate to control the leg ulcers.
PXE is an autosomal recessive disorder resulting in clumped, distorted, and calcified elastic fibers. Most patients have a loss-of-function mutation in both copies of ABCC6 which is found in hepatocytes.
6
Other mutations identified in PXE are ENPP1, and GGCX.7,8 PXE, like PAN, primarily affects mid-sized arteries. However, in PXE, the progressive calcification of the elastic media and intima results in atheromatous plaques which can result in intermittent claudication, hypertension, myocardial infarction, angina pectoris, and stroke.
9
Our patient did not have any of the previously described mutations and no evidence of systemic involvement in keeping with PXE-like phenotype. PXE-like has been described in patients with β-thalassemia, ingestion of penicillamine, multiple coagulation factor deficiency, contact with saltpeter, ingestion of
Our patient has two rare entities, cutaneous PAN and PXE-like phenotype. We speculate that the occurrence of the two conditions in our patient is coincidental and brings to light the importance of performing a complete cutaneous exam.
Footnotes
Acknowledgements
The authors thank the patient for granting permission to publish this information. The authors also thank Dr May Chergui for providing the histopathological images and expertise.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Denis Sasseville receives royalties from UpToDate (Wolters Kluwer Health). The other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The patient signed informed consent for the collection and publishing of the non-identifiable images. Upon request, the informed consent form can be provided.