
Abstract
A 64-year-old female underwent a successful first percutaneous intervention using MISAGO stents for a de novo femoropopliteal lesion. Subsequently, three more effective procedures were done using balloon catheters for in-stent restenosis. In May 2016, a fourth procedure using Zilver PTX stent for in-stent restenosis was carried out. For this final procedure, we added direct oral anti-coagulant as she had additional problem of popliteal vein thrombosis and her femoropopliteal segment remained clear. A Zilver PTX stent, a drug-eluting stent for a peripheral artery, was expected to bring superior outcomes compared to conventional bare nitinol stents (i.e. MISAGO stent). But subsequent studies reported that Zilver PTX stent was not more effective than conventional bare nitinol stents. In our above mentioned case, her angioscopy findings suggest that her successful outcome appears to be related to the added direct oral anti-coagulant.
Keywords
Introduction
There is a continuing question about how best to treat recurrent in-stent restenosis (re-occlusion) in femoropopliteal segment. Tosaka et al. 1 reported that 1-year patency after balloon angioplasty for in-stent re-occlusion in femoropopliteal segment was quite low (22.7%). One-year efficacy of drug-eluting stent for this issue was reported; 2 however, its durability over several years was not certain. On the other hand, possible efficacy of direct oral anti-coagulant (DOAC) for patency after endovascular therapy in femoropopliteal segment was recently reported.3,4 The possibility of DOAC might offer effective post-procedure therapy and should be studied using case experiences. In our study, we report that where-patency was kept for 4 years after a drug-eluting stent was implanted into a recurrent in-stent restenosis with DOAC added on.
Case
In September 2014, a 64-year-old female was referred from vascular surgery for right leg recurrent intermittent claudication a few months after femoropopliteal bypass using polytetrafluoroethylene (PTFE) graft for atherosclerotic occlusion of superficial femoral artery (SFA). She had diabetes mellitus and hypertension, but neither smoking history nor renal insufficiency. Angiography revealed occlusion of femoropopliteal bypass graft (Figure 1(a)). We discussed about long-term patency of her native occluded SFA (TASC D) after endovascular therapy using bare nitinol self-expanding stents. After obtaining her informed consent, we undertook endovascular therapy which was initially successful. We deployed three MISAGO 6.0–100 mm stents (Terumo, Japan) and an optimal angiography was obtained (Figure 1(b)). Dual anti-platelet therapy by clopidogrel 75 mg and cilostazol 200 mg was continued and both blood pressure and HbA1c level were controlled fairly well. But repetitive balloon angioplasty for in-stent restenosis was necessary every 6 months after initial procedure.
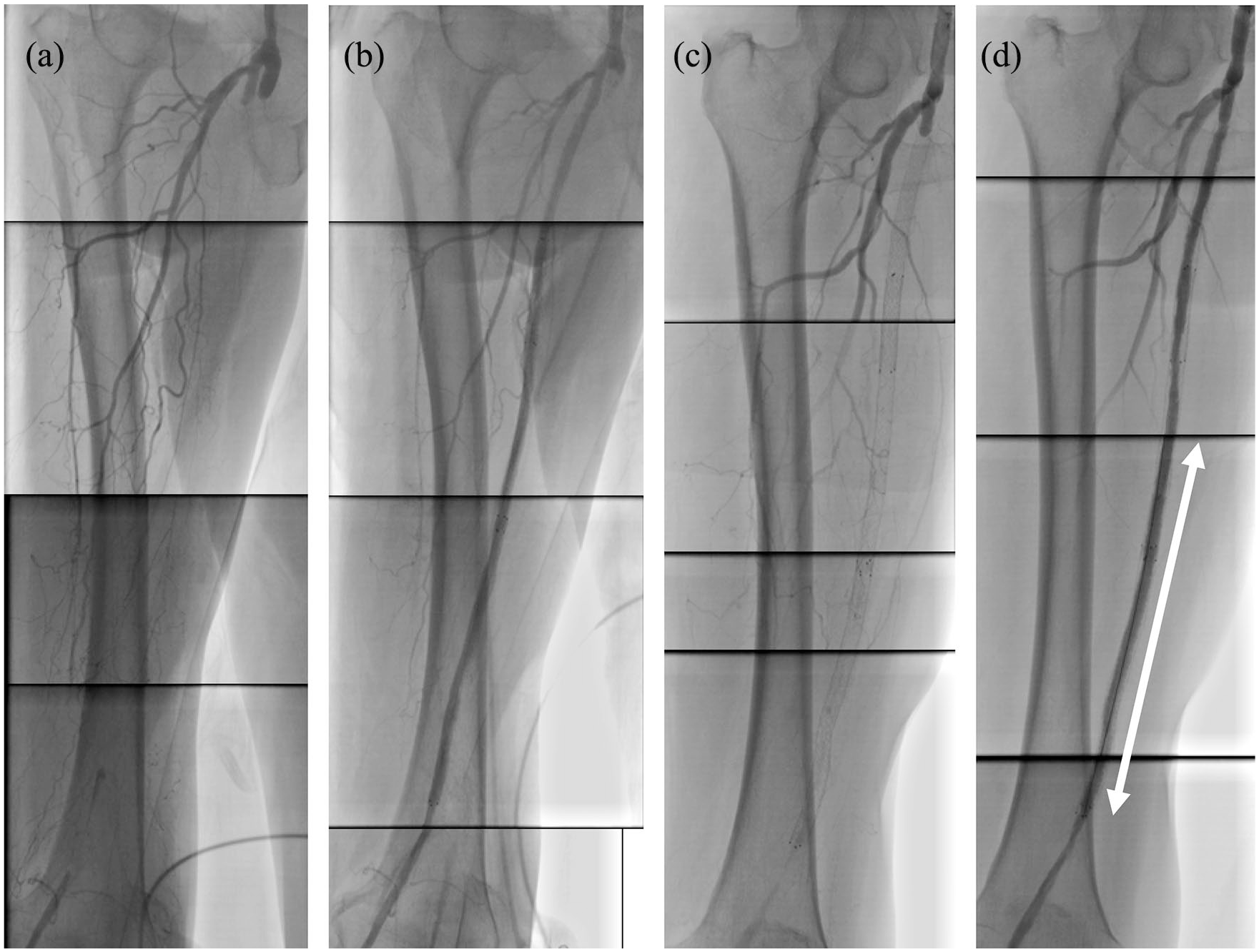
Panels (a) and (b) show baseline and final angiography at the index procedure in September 2014. Panels (c) and (d) show baseline and final angiography at the fourth procedure in May 2016. A white arrow indicates the segments where Zilver PTX 6.0–120 mm stent was deployed at this time.
The first time focal in-stent restenosis at middle SFA and diffuse in-stent restenosis at distal SFA occurred, non-slip element percutaneous transluminal angioplasty (NSE PTA) 5.0–40 mm balloon (NIPRO, Japan) and Senri 5.0–100 mm balloon (Terumo, Japan) were used for each lesion. The second time a diffuse in-stent restenosis at distal SFA recurred, NSE PTA 6.0–40 mm balloon (NIPRO, Japan) and Sterling OTW 5.0–100 mm balloon (Boston Scientific, United States) were used. At the end of each procedure, optimal angiographies were obtained. In May 2016, intermittent claudication recurred and duplex sonography unexpectedly revealed in-stent re-occlusion (TOSAKA class III) and thrombus at her popliteal vein. After discussion with her, we decided to do re-canalization using drug-eluting stent and add edoxaban 15 mg for prevention of deep vein thrombosis. Endovascular therapy was started by left femoral approach and baseline angiography showed total occlusion form proximal SFA to the middle of most distally implanted MISAGO stent (Figure 1(c)). On the fluoroscopy, MISAGO stents showed no stent fractures. Antegrade Treasure guide wire (ASAHI Intec, Japan) could easily pass, and balloon angioplasty using SABER 6.0–150 mm balloon (Cordis, United States) obtained good antegrade blood flow. On intra-vascular ultra-sonography (IVUS), MISAGO stents were well expanded, and neo-intimal hypertrophy were observed in the most distally MISAGO stent. The procedure ended with Zilver PTX 6.0–120 mm stent (Cook Medical, United States) deployment followed by post-ballooning (SABER 6.0–150 mm balloon (Cordis)) at distal lesion where recurrent in-stent restenosis occurred (Figure 1(d)). On final IVUS, implanted Zilver PTX stent was roundly well expanded, and minimum stent area (MSA) was estimated to be 15.5 mm2. After that procedure, medication of edoxaban 15 mg, clopidogrel 75 mg, and cilostazol 200 mg continued without any bleeding complications and angiography showed patent SFA in March 2020 (Figure 2(a)). In angioscopy findings in March 2020, MISAGO stent struts were invisible (Figure 2(b)); however, entire Zilver PTX stent struts were embedded in the neo-intima and still translucent (Figure 2(c)). A plaque underneath entire stent struts appeared white, and no thrombus was seen.

Panel (a) shows angiography in March 2020. Panels (b) and (c) show angioscopic findings at MISAGO stent (a black arrow) that was deployed 6 years before and Zilver PTX stent (a white arrow) that was deployed 4 years before.
Discussion
We see a remaining problem about refractoriness of re-canalization of in-stent restenosis in femoropopliteal segment and break-through strategy that has not yet been overcome. Tosaka et al. 1 reported the limitation of balloon angioplasty, especially for in-stent re-occlusion. We chose Zilver PTX stent (Cook Medical) owing to its superior performance as the first generation drug-eluting stent in peripheral segments compared to conventional bare nitinol stents; however, Zilver PTX stent (Cook Medical) unfortunately failed to show durability superiority in subsequent reports.5,6 Zeller et al. 2 reported a 1-year clinical efficacy of Zilver PTX stent (Cook Medical) in use for in-stent restenosis; however, its efficacy over several years was uncertain. According to the reports, we speculated that it would be difficult to believe that Zilver PTX stent was a main factor for our case to keep patency over several years.
In use of Zilver PTX stent (Cook Medical), long lesion (≥16 cm), small vessel (the external elastic membrane area ≤27 mm2), and under-expansion of a stent (minimal stent area ≤12 mm2) were reported as predictors for in-stent restenosis in 2015. 7 On this point, our procedure in 2016 might be optimal to bring out its beneficial performance because spotty stenting only for distal in-stent occlusion site could be performed (i.e. stent lesion length was not longer than 16 cm) and enough stent expansion could also be obtained (i.e. minimal stent area was larger than 12 mm2).
Recently, possible efficacy of DOAC in peripheral artery disease has been reported.3,4 Moll et al. 3 reported potential efficacy of edoxaban (60 mg/day) in conjunction with aspirin compared with clopidogrel and aspirin for preventing restenosis/re-occlusion following endovascular therapy in their randomized prospected study. In VOYAGER PAD trial, revascularization rate of rivaroxaban group (rivaroxaban 5 mg plus aspirin 100 mg/day) for 3 years was 20% and the rate of major bleeding defined according to the thrombolysis in myocardial infarction classification in rivaroxaban group for 3 years was 2.65%. 4 In this case, edoxaban 15 mg plus clopidogrel 75 mg and cilostazol 200 mg maintained vascular patency without any minor bleeding for 4 years.
The most notable point in this case might be her angioscopy findings. To the best of our knowledge, angioscopy findings several years after drug-eluting stent implantation have not been reported with the exception of this case. Tsukiyama et al. 8 reported that over 80% of Zilver PTX stents (Cook Medical) were completely covered and their struts were invisible at 1 year. In contrast, her angioscopy findings showed that stent struts remained translucent 4 years after original stent implantation. These findings suggest possible benefits of DOAC modification. Further investigation into efficacy of DOAC in peripheral intervention, its mechanism, class-effects, and appropriate dosage would be useful.
Conclusion
Although single case experience, addition of a DOAC to recurrent in-stent restenosis in a peripheral vascular disease patient might help in preserving patency over several years.
Footnotes
Acknowledgements
The authors thank Steve Burke for medical writing assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.