
Abstract
Chryseobacterium indologenes is a non-glucose fermenting Gram-negative bacteria widely distributed in nature. It has been found to cause a variety of infections like nosocomial pneumonia, bacteremia and wound infections usually in immunosuppressed patients and those with indwelling devices. The organism is resistant to a significant number of the commonly prescribed broad spectrum antibiotics. We report a rare case of meningitis due to C. indologenes in a patient diagnosed with medulloblastoma and hydrocephalus with an external ventricular drain in situ. The patient was successfully treated with trimethoprim/sulfamethoxazole combination and external ventricular drain replacement as shown by subsequent sterile cultures.
Introduction
Chryseobacterium indologenes, a non-motile Gram-negative bacteria, is widely distributed in nature and has been recovered from soil, plants, foodstuffs and water sources. In the hospitals, sink traps, feeding tubes and indwelling devices have been identified as reservoirs for Chryseobacterium spp. It is a non-glucose fermenting bacteria producing beta-hemolysis on sheep blood agar. It is oxidase and catalase positive, produces the pigment flexirubin and hydrolyses gelatin and esculin. 1 In 1993, Bonten et al. 2 first isolated a strain of C. indologenes from the tracheal aspirate of a patient with ventilator-associated pneumonia but the pathogenic role was unclear. Later its invasive nature in humans and significance as a true pathogen was identified in Taiwan. Since then, it has been found to cause a wide range of infections including nosocomial pneumonia, intraabdominal infection, wound infection, primary bacteremia, intravascular catheter–related bacteremia and cellulitis.3–5 Some of the major risk factors identified with infection are immunocompromised status, indwelling devices like tracheostomy tubes and patients with diabetes. 6 C. indologenes is intrinsically resistant to carbapenems and cephalosporins due to the production of molecular class A β-lactamase and class B carbapenem-hydrolyzing β-lactamase.7,8 Its presence in the inaminate objects in the hospital, ability to infect immunocompromised patients and intrinsic resistance to antibiotics could prove to be the decisive factor for the unfavourable outcomes in the hospitalized patients.
In this study, we report a rare case of meningitis caused by C. indologenes in an adult patient diagnosed with medulloblastoma who had an external ventricular drain (EVD) in situ. The patient was treated successfully and subsequent cerebrospinal fluid (CSF) cultures showed no growth.
Case report
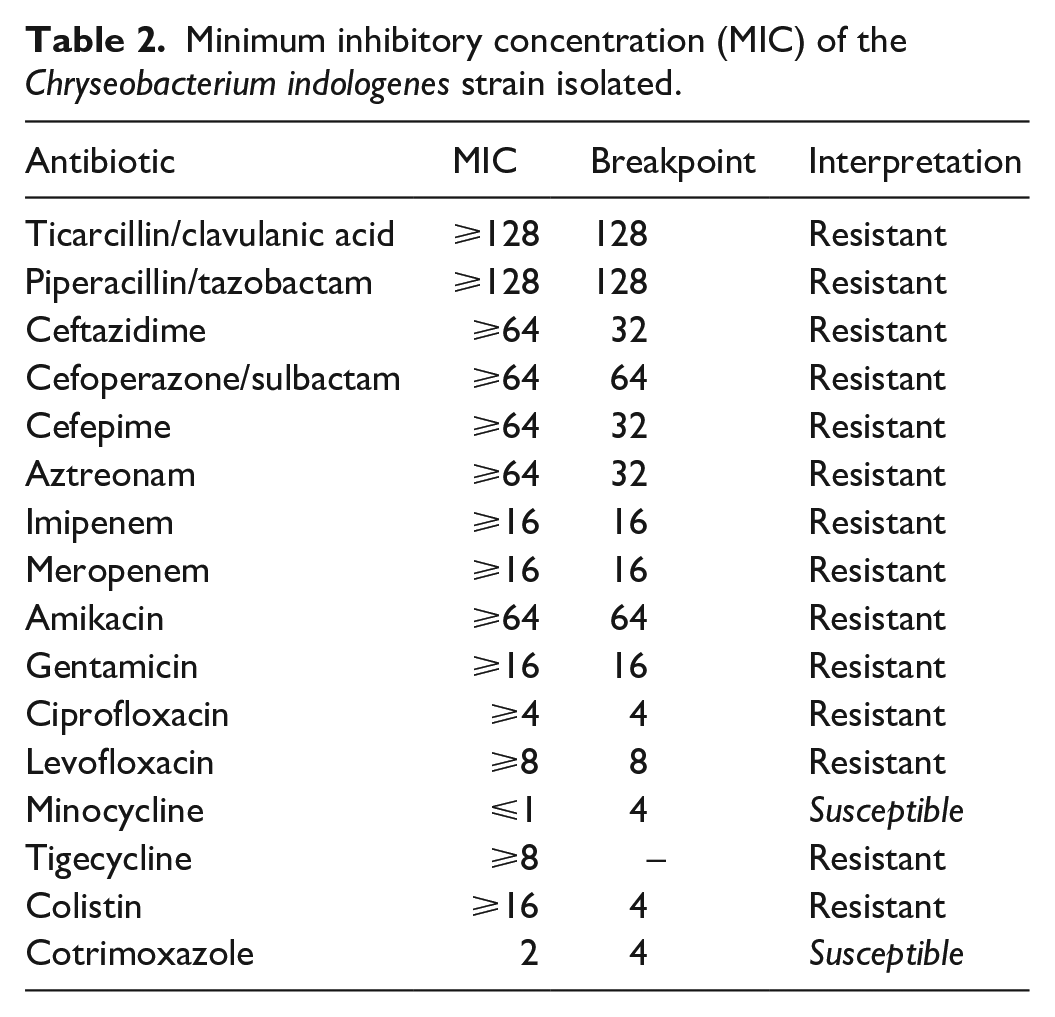
The patient is a 28-year-old female who was diagnosed with medulloblastoma when she was 8 years old. Corrective surgery for medulloblastoma was done in the year 1998 and a ventriculoperitoneal (VP) shunt was placed. On 9 September 2018, the patient did not get up in the morning and was found to be drowsy by the relatives. She was brought to the neurosurgery department where the VP shunt was found to be blocked. An EVD was placed following which clinical improvement was noted. However, shunt revision done on 21 October failed and EVD was again placed. For bacterial culture, CSF samples sent to the Microbiology Laboratory were inoculated on a plate of 5% sheep blood agar, 5% heated blood agar and MacConkey’s agar and incubated at 37°C for 18–24 h. The CSF samples were also inoculated in brain heart infusion broth (BHI broth) and incubated for 48 h. During the first 2 months, three CSF samples were collected and they were sterile. However, bacterial growth was seen in the CSF samples collected later on and the bacteria was identified as Acinetobacter spp. which was susceptible to ciprofloxacin, trimethoprim/sulfamethoxazole and gentamicin (Table 1). The patient was treated with gentamicin (80 mg IV BD for 7 days) and no further cultures yielded growth of Acinetobacter spp. However, not much clinical improvement was observed in the patient and the fresh CSF sample was found to be turbid. The CSF sample was sent to Microbiology Laboratory and on gram stain, few pus cells were seen while no bacteria/fungal elements were present. The sample was cultured and large, yellow coloured, mucoid colonies were observed on 5% sheep blood agar and 5% heated blood agar. The colonies were beta-hemolytic. Small non-lactose fermenting colonies were seen on MacConkey’s agar. Gram stain of the colonies revealed Gram-negative cocci and the organism was found to be non-motile on hanging drop preparation. The isolate was found to be indole positive, catalase positive and oxidase positive. The identification and sensitivity testing was done using Vitek-2 Compact (Biomerieux®) and the organism was identified as C. indologenes which was resistant to ticarcillin/clavulanic acid, piperacillin/tazobactam, ceftazidime, cefoperazone/sulbactam, cefepime, aztreonam, imipenem, meropenem, amikacin, gentamicin, ciprofloxacin, levofloxacin, tigecycline and colistin. The only sensitive drugs were found to be minocycline and trimethoprim/sulfamethoxazole (Table 2). This organism was isolated in the first CSF sample which had growth of Acinetobacter spp. but since it was not recovered in subsequent samples, it was believed to be a contaminant. Further antibiotic susceptibility testing was carried out using Kirby Bauer disc diffusion method as per CLSI guidelines. 9 The organism was found to be susceptible to vancomycin, linezolid, nitrofurantoin and teicoplanin, while the drugs ceftriaxone, amoxycillin + clavulanic acid, cefotaxime, netilmicin and tobramycin were found to be ineffective. The organism was isolated from the patient’s CSF samples repeatedly. The blood samples were taken from the patient at various intervals and they were found to be sterile. The other laboratory results during this time were as follows: complete blood count showed haemoglobin was 10.7 g/dL, platelets were 455,000/µL, total leucocyte count was 11,900/µL, with the differential leucocyte count comprising neutrophils (68%), lymphocytes (26%), monocytes (4%) and eosinophils (2%) and the hematocrit was 30.4%. Cytology study of the CSF sample revealed cell count to be 45 cells/mm3 with polymorphs (22%) and lymphocytes (78%). The EVD of the patient was replaced and the patient was started on trimethoprim (80 mg)/sulfamethoxazole (400 mg) orally twice daily for 7 days. CSF samples collected after a week of starting therapy were found to be sterile.
Cerebrospinal fluid (CSF) sample culture results with the organisms and their susceptibility.

Minimum inhibitory concentration (MIC) of the Chryseobacterium indologenes strain isolated.
Discussion
The genus Chryseobacterium, first defined in 1994 and earlier named flavobacterium, has six species commonly isolated from clinical specimens: C. meningosepticum, C. odoratum, C. multivorum, C. breve, C. indologenes and C. gleum. 6 C. indologenes is a non-motile, catalase-positive, indole-positive, oxidase-positive, non-glucose fermenting Gram-negative bacteria widely distributed in nature and is responsible for nosocomial infections. Although not a normal component of human microbiota, its presence in the hospital environment (wet surfaces and water sources) poses a significant risk. The predisposing factors for infection include immunocompromised status, malignancy, neutropenia, diabetes, organ transplant, steroid use, malnutrition and indwelling devices like respirators, endotracheal tracheostomy tubes, mist tents humidifiers and so on. 10
The organism’s ability to produce protease and biofilms on indwelling devices play an important role in invasive infections.11,12 Most cases with C. indologenes infections are catheter-related bacteremia and nosocomial pneumonia, with very few studies reporting it to be the causative agent for meningitis.13–16
Resistance to aminoglycosides, tetracyclines, chloramphenicol, erythromycin, clindamycin and teicoplanin makes the infections caused by Chryseobacterium spp. difficult to treat.1,4,5 The SENTRY Antimicrobial Surveillance Programme showed that the most active antimicrobial were the quinolones, especially the newer agents (levofloxacin, garenoxacin and gatifloxacin). 17 The isolate in our study was found to be resistant to levofloxacin with minimum inhibitory concentration ⩾8. However, it was found to be susceptible to trimethoprim/sulfamethoxazole and minocycline similar to what was seen by Chou et al. 18
Initially, in our case the organism was thought to be an environmental contaminant as subsequent cultures did not yield this organism but instead growth of Acinetobacter spp. was seen in repeated CSF samples. When Chryseobacterium spp. was isolated from the patient in subsequent cultures, it was believed to be the pathogen responsible for causing meningitis in this patient. This is important because if treatment was directed against C. indologenes from the beginning, then the patient could have improved faster reducing the days of hospitalization. Trimethoprim/sulfamethoxazole combination was started and the EVD was replaced. There is no clear rule that indwelling catheters should be removed or not with studies citing it to be a necessity while others proving that all catheters need not be removed.4,5,19 The CSF samples collected from the patient later did not yield any bacterial growth and the patient was successfully treated.
Conclusion
C. indologenes meningitis can occur in patients having indwelling devices and prolonged hospitalization but it can be successfully treated by giving appropriate antibiotics based on the antibiotic susceptibility pattern.
Footnotes
Authors’ contribution
All the authors were actively involved in the conceptualization, methodology, investigation and writing of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.