
Abstract
Melanoma is an aggressive skin cancer form with a grave prognosis. Current results suggest that oncolytic virus treatment of melanoma has a high therapeutic potential. ECHO-7 (Rigvir) is the first oncolytic virus registered in Latvia. A female patient was diagnosed with stage IIIB melanoma in December 2012, over 9.4 years ago. After the first excision and re-excision, the patient had several recurrences and disease progressions. After the patient had received surgical treatment in 2014, ECHO-7 virus oncolytic virotherapy was started. Since then, the patient has experienced only one more disease progression episode in May 2015 and has been stable for over 60 months. The patient has not received any other treatment than surgery and oncolytic virotherapy. No severe adverse events have been reported during virotherapy. The present case suggests that ECHO-7 virotherapy is an effective treatment of skin melanoma.
Introduction
Research of cancer cell biology has shown that the changes that occur in the cancer cells make them more susceptible to viral infections. In order to avoid recognition by the immune system, several pathways are altered, for example, the interferon-mediated pathway. Both wild type and genetically engineered viruses have the ability to infect cancer cells while sparing the healthy cells of the organism. Currently, oncolytic viruses are tested for various indications, malignant melanoma being one of them. 1 Oncolytic viruses not only infect cancers cells and thus destroy them, but can also induce immune system reaction. When oncolytic viruses propagate and the cancer cell undergoes apoptosis, new viral particles, tumour associated antigens (TAA), damage associated molecular patterns (DAMP) and pathogen associated molecular patterns (PAMP) are released and induce an immune system response. Therefore, it has been suggested that oncolytic viruses not only directly kill cancer cells, but also expose them to the immune system. 2
ECHO-7 virus strain Rigvir is a positive sense single stranded RNA virus that has been selected and adapted for melanoma. It was registered in Latvia in 2004. A retrospective study has shown that stage IB–IIC melanoma patients benefit from ECHO-7 therapy after a surgery. In comparison to the control group, patients who received ECHO-7 virotherapy had 4.39- to 6.57-fold lower mortality. ECHO-7 was well tolerated and no severe adverse event was observed. 3
Talimogene laherparepvec is a herpes simplex type 1 virus that has been genetically modified to express human granulocyte–macrophage colony-stimulating factor (GM-CSF). Talimogene laherparepvec is approved for treatment of advanced melanoma in the United States and Europe since 2015. 4 Clinical trials involving unresected stage IIIB to IV melanoma patients showed increased durable response rate, objective response rate, and progression-free survival in the Talimogene laherparepvec study arm. 5
HF-10, Reovirus Serotype 3 - Dearing Strain, Vaccinia virus, Coxsackie virus A21 and adenovirus are also currently in clinical trials for melanoma treatment. Clinical studies involve not only monotherapy, but also combination therapy treatment. 6
Here we report a stage IIIB melanoma patient that has received oncolytic virotherapy with ECHO-7 virus after disease progression. The patient has been treated with ECHO-7 virus for over 70 months, experienced one more relapse in April 2015, but since then she has been stable for over 60 months. The patient has not received any other concomitant treatment post-surgery.
Results
A female patient at the age of 78 felt a small lesion in the bottom of the heel which then turned into ulcer. Surgical excision of the lesion was performed on 29 December 2010 with subsequent inguinal lymphadenectomy in February 2011.
The histopathological examination showed that the primary tumour was composed of spindle, epithelioid and nevoid cells, with large, round and elongated nuclei with prominent vesicular nuclei, large nucleoli, abundant eosinophilic cytoplasm with focal melanin pigment, focal necrosis, haemorrhage, epidermal ulceration, with moderate lymphocyte infiltration, invasion in sinus lymph vessels without vascular and perineural invasion. The tumour cells demonstrated marked nuclear pleomorphism with variation in cell size, shape and staining with increased number of mitosis up to 58/mm2 (Figure 1(a) and (b)). The tumour was Melan A immunopositive (Figure 1(c)).

Representative photomicrographs: (a) 29 December 2010. Nodular epithelioid, nevoid and spindle cell melanoma. The tumour cells demonstrated marked nuclear pleomorphism with variation in cell size, shape and staining. Scale bar is 20 µm; haematoxylin-eosin staining, (b) 29 December 2010. Nodular epithelioid, nevoid and spindle cell melanoma. The tumour cells demonstrated marked nuclear pleomorphism with variation in cell size, shape and staining. Scale bar is 10 µm; haematoxylin-eosin staining, (c) 29 December 2010. Melan A immunostaining. Scale bar 10 µm; haematoxylin-eosin staining, (d) 28 May 2013. Melanoma subcutaneous metastasis. Scale bar 20 µm; haematoxylin-eosin staining, (e) 28 May 2015. Melanoma lymph node metastasis. Scale bar 10 µm; haematoxylin-eosin staining, (f) 28 May 2015. Melanoma lymph node metastasis. Scale bar 5 µm; haematoxylin-eosin staining.
In addition, the melanoma metastasis to the right inguinal lymph node was observed. The TNM staging was T3bN1bM0. Clark level 4 and Breslow 3 mm. The metastatic lymph nodes were up to 4.0 cm.
A computed tomography (CT) scan in February 2012 did not show metastases in the lungs or in the retroperitoneal area (Figure 2(a) and (b)). Fibrous infiltration in the subcutaneous adipose tissue in the right inguinal area was observed in February 2012 (Figure 2(c)) and in May 2012 (Figure 2(d)).
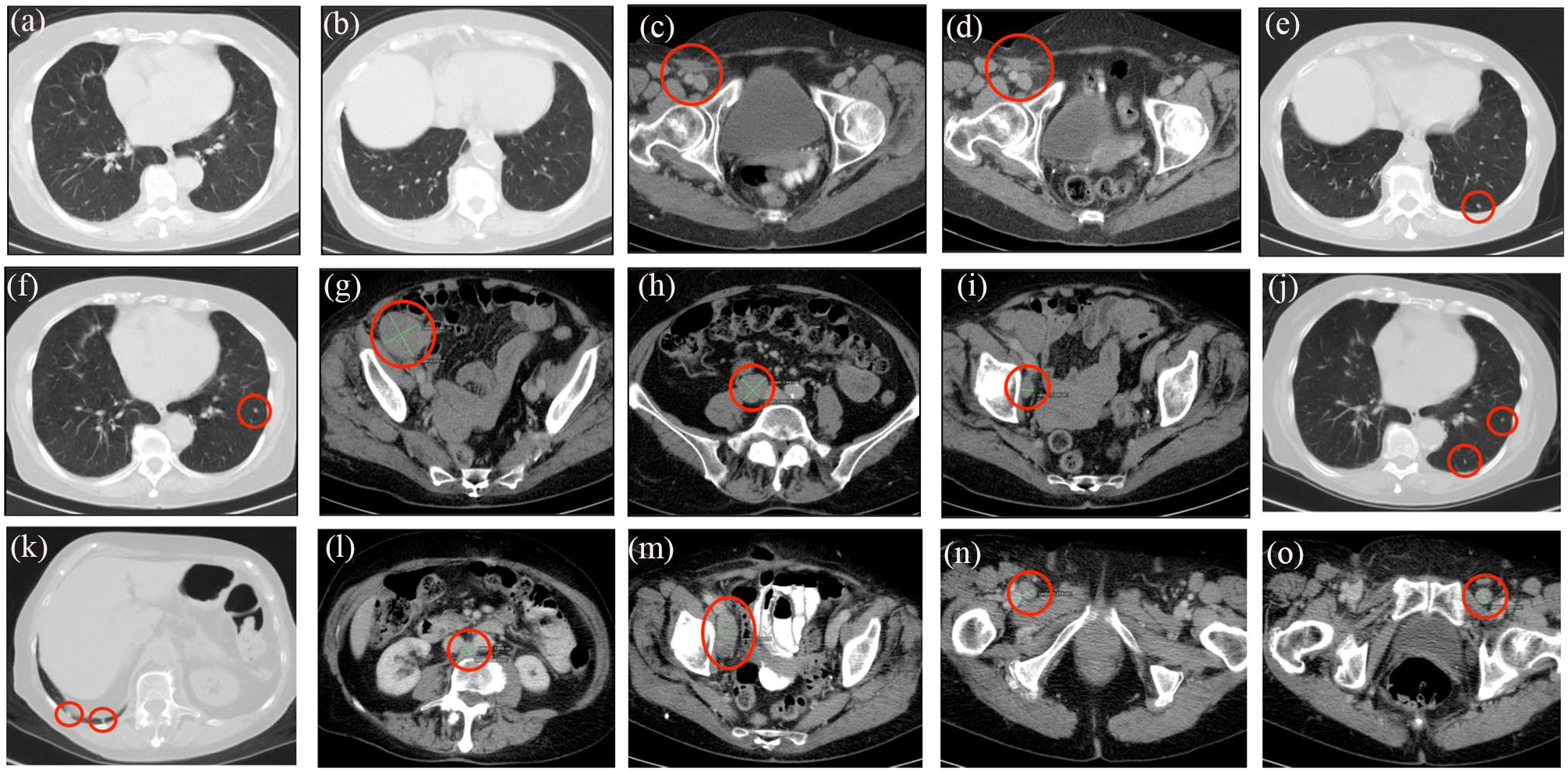
Contrast-enhanced computed tomography (CT). (a and b) 24 February 2012. No enlarged lymph nodes or lesions in lung basal part were observed, (c) 24 February 2012. Fibrous infiltration in the subcutaneous adipose tissue in the right inguinal area was observed, (d) 17 May 2012. Fibrous infiltration in the subcutaneous adipose tissue in the right inguinal area was observed, (e and f) 22 April 2015. Lesions in left lung basal part 0.4 cm in diameter were observed, (g–i) 22 April 2015. Enlarged lymph nodes retroperitoneal pericaval right area 3.0 cm x 2.5 cm and parailiacal right area 3.8 cm x 4.7 cm, (j and k) 19 February 2018. Lesions in basal part of both lungs 0.4–0.5 cm, (l–o) 19 February 2018. Enlarged lymph nodes in retroperitoneal interaortacaval area 1.4–1.8 cm, enlarged lymph node in right parailiacal side up to 2.1 cm x 4.6 cm, enlarged lymph nodes in inguinal area, in the right side up to 1.4 cm in diameter, and up to 1.3 cm in diameter in the left side were observed.
In 2013, cutaneous metastases in the sole of the foot, right leg medial, lateral and posterior surface, as well as at the right inguinal part were observed. During the surgery on 28 May 2013, 9 subcutaneous and dermal lesions with diameter of 0.3–1.0 cm were excised. The tumour did not exhibit any degree of regression (Figure 1(d)).
On 7 August 2014, ECHO-7 virotherapy was started (2 ml intramuscular injections, 106 TCID50/ml alternately in left and right gluteus and deltoid muscles); the first 4 months ECHO-7 virus administration was every 3 weeks. Subsequent administrations have so far been with an average interval of 30.8 days. The patient has received a total of 62 administrations by 12 September 2019 and ECHO-7 virotherapy is ongoing.
In April 2015 a CT scan showed metastases in 5 right parailiacal and 6 paraaortal lymph nodes with capsular invasion. The CT also showed lesions 0.4 cm in diameter in the basal part of the left lung (Figure 2(e)and (f)), enlarged lymph nodes in the right retroperitoneal pericaval area (3.0 cm x 2.5 cm) and in the right parailiacal area (3.8 cm x 4.7 cm) (Figure 2(g)–(i)). Surgery was performed on 28 May 2015. Two lesions 10 x 9 x 4 and 7 x 5 x 3 cm in size were excised and histologically examined; metastatic melanoma lesions in lymph nodes were observed in both samples with regression of melanoma manifested with cells ballooning and necrosis compared to previous histopathological findings (Figure 1(e) and (f)).
Lesions in the basal part of both lungs (0.4–0.5 cm) were observed on CT in February 2018 (Figure 2(j) and (k)). Enlarged lymph nodes in the retroperitoneal interaortacaval area (1.4–1.8 cm), an enlarged lymph node on the right parailiacal side (2.1 cm x 4.6 cm), enlarged lymph nodes in the right (up to 1.4 cm in diameter) and left (up to 1.3 cm in diameter) of the inguinal area were observed in February 2018 (Figure 2(l)–(o)). In comparison to May 2015, the radiological examination showed that the largest lymph nodes had decreased in size, while new, smaller lymph nodes had appeared.
The patient has not received any other treatment besides surgery and ECHO-7 virotherapy. No adverse events have been observed during the therapy with ECHO-7 virus strain.
Discussion
The foot is considered a problematic spot for melanoma. The disease may be confusing, leading to misdiagnosis of the lesion.7,8 As with any type of malignant melanoma, the most important survival indicators are tumour thickness, ulceration and lymph node metastases. Because of infrequent checks of the acral skin, the lesion is often diagnosed quite late with big tumour thickness. Furthermore, there is increased risk for thick melanomas to reappear on the acral skin of the upper part of the leg. 7
Oncolytic virotherapy for melanoma is increasingly emerging as a novel treatment that can both have a direct effect on the tumour and also induce a systemic immune response. 9 Studies of oncolytic viruses for various cancers are ongoing; both as combination treatments and monotherapies. 10 The first oncolytic virus registered by the FDA and EMA is talimogene laherparepvec, which is used in advanced melanoma and has shown efficacy on overall survival for patients with cutaneous metastases. 11 Available data show that the expected survival for stage IIIB melanoma patients treated according to standard treatments in the United States 9.4 years after diagnosis is approximately 45%. 12
Conclusion
The present patient was diagnosed over 9.4 years ago. After several recurrences and progression episodes, stabilization of the disease has been observed since June 2015, for over 70 months during virotherapy treatment. The present case suggests that ECHO-7 virotherapy is an effective treatment for cutaneous melanoma.
Footnotes
Authorship
All authors attest that they meet the current ICMJE criteria for Authorship.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.T., A.R., and P.A. are employees of the Rigvir group. V.S., E.O., and S.I. state no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.