
Abstract
Blastomycosis is a primary pulmonary mycosis of humans usually affecting patients geographically located near the Great Lakes, Lake-of-the-Woods and northern Ontario. We report a case of cutaneous blastomycosis in a patient with no environmental contact outside of Saskatchewan.
Introduction
Blastomycosis is a dimorphic fungus that grows as a nonpathogenic mold in the environment and converts to a pathogenic yeast after it infects the host. 1 The majority of cases of blastomycosis have been reported in North America, particularly the southeastern and south-central states bordering the Mississippi and Ohio River basins, and the states and provinces bordering the Great Lakes, the St. Lawrence and Nelson River.2,3 Most patients diagnosed with blastomycosis in Canada were from Ontario and Manitoba specifically northern Ontario, Rainy River, Thunder Bay and Kenora. 3 Hyperendemicity in the region surrounding Kenora, Ontario (near Lake-of-the-Woods) was estimated to have the highest annual incidence of blastomycosis anywhere in North America. 3 Previously thought to be a disease of North America, blastomycosis is now known to be endemic in many African countries and India. 3 A recent review of Regina Qu’Appelle Health Region data by Lohrenz, 4 reported 15 cases of blastomycosis in southern Saskatchewan between 2000 and 2015. Of the cases identified, eight had respiratory symptoms as their presenting complaint, four initially presented with cutaneous lesions, four with constitutional symptoms and one with chest pain after a fall. Of the four cases involving the skin, two of the cutaneous Blastomyces cases were isolated to the skin and the other two involved skin and other organ systems. Blastomycosis is one of the great mimickers in medicine and can be misdiagnosed as neoplasia, chronic pneumonia, immunologic skin disorders, tuberculosis, nocardia, pyoderma gangranosum 5 and other deep mycoses.6,7 Skin manifestations were diverse in the four cases and included a nonhealing ulceration of the ear, fluctuant subcutaneous nodules that broke and drained fluid to become nonhealing ulcerations, a necrotizing genital lesion and a hyperkeratotic cratered lesion resembling a keratoacanthoma. 4 Prior to this report, Saskatchewan blastomycosis data were gleaned from the Vallabh et al. cases presented in 1988. Three cases were presented, two were isolated to the lungs, the third case involved the lungs, kidney, liver, spleen, skin, left talus and subtalar joint. 8 Blastomycosis is a systemic infection primarily involving the lungs that occurs after inhalation of Blastomyces dermatidis. Hematological spread of the fungus can commonly cause disease impacting the bones, genitourinary systems and rarely the central nervous system (CNS). 7 The majority of cutaneous lesions are reported from hematogenous spread and not from direct inoculation. 1
Case report
We present a 51-year-old otherwise healthy female patient with isolated cutaneous blastomycosis with no evidence of pulmonary disease or hematological spread. At the time of referral, the patient had a 17 cm × 6.5 cm ulcerated verrucous plaque with foul smell and purulent discharge on her abdomen (Figure 1). The patient indicated the plaque had expanded over the time span of a year and had not responded to several courses of oral or intravenous antibiotic therapy. An incisional biopsy of the lesion displayed broad-based budding yeasts with doubly refractile cell walls consistent with B. dermatitis (Figures 2–4). The patient denied any travel outside of Saskatchewan and had no respiratory symptoms. The patient did recall going camping a week prior to first noticing a spot on her abdomen. While camping, the patient reported carrying firewood that would have rested on her abdomen in the area of her plaque but did not specifically recall a scratch or break in the skin. Chest X-ray and sputum cultures were negative. The patient was successfully treated with a 6-month course of oral itraconazole (Figures 5 and 6).

Ulcerated verrucous plaque on the abdomen.
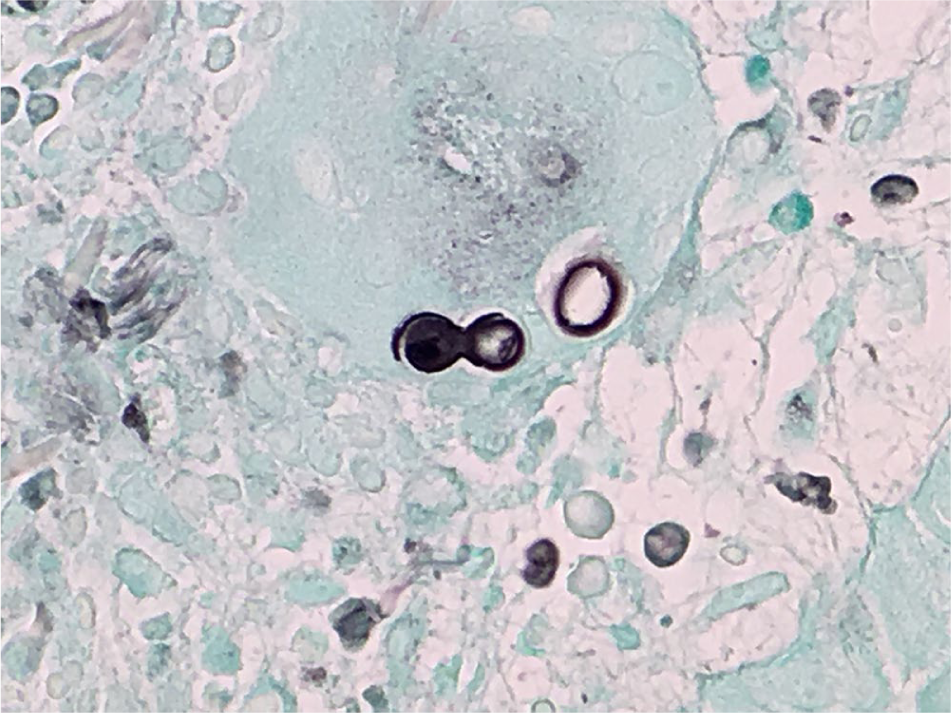
Specimen stained by the Gomori methenamine silver stain method.

High-power magnification of the skin biopsy specimen reveals a broad-based budding yeast cell.

Low-power examination of a hematoxylin-and-eosin stained skin biopsy specimen.

After 8 weeks of itraconazole treatment.

Healed after itraconazole 200 mg p.o. TID for 3 days then 200 mg p.o. BID for 6 months.
Discussion
Blastomycosis is an uncommon fungal infection that is infrequently reported in the province of Saskatchewan. This case report demonstrates a non-healing abdominal lesion infected with blastomycosis in a patient with no environmental contact outside of Saskatchewan. Case reports have shown that the incubation period for cutaneous inoculation of blastomycosis is considerably shorter (14 days) versus the incubation period for blastomycosis caused by pulmonary exposure (30–40 days). 9 In this case, the timing of the initial lesion presentation combined with the lack of systemic symptoms and negative chest X-ray suggests that this patient could have been inoculated while carrying firewood. Damp soil and decaying wood are known to be favorable hosts to blastomycosis. 3 However, there are cases of secondary cutaneous blastomycosis having no associated pulmonary findings on chest radiography. 10 It is difficult to distinguish cutaneous inoculation blastomycosis from secondary cutaneous blastomycosis with a subclinical pulmonary focus. 10 It is not possible to determine whether this case report is primary or secondary blastomycosis. To prevent dissemination of blastomycosis antifungal therapy is necessary for all infected patients. 3 The majority of patients with blastomycosis can be treated with oral itraconazole for a duration of 6–12 months depending on clinical and radiographic improvements. In cases of life threatening disseminated blastomycosis or CNS infections, more aggressive treatment with intravenous amphotericin is required initially followed by a 6–12-month course of oral itraconazole. 6
This case report highlights the importance of considering blastomycosis as a potential pathogen for patients in Saskatchewan especially those not responding to treatment with antibiotics.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Patient consent was obtained.