
Abstract
Splanchnic pseudoaneurysms are rare causes of hemobilia. Specifically, hepatic artery pseudoaneurysms from infectious or inflammatory etiology are even more rare. In this article, we describe our encounter with a 72-year-old female presenting with obstructive jaundice and acute blood loss anemia. Upper endoscopy indicated hemobilia and endoscopic retrograde cholangiopancreatography was completed with stent in place. Post endoscopic retrograde cholangiopancreatography, computed tomography angiogram indicated a right hepatic artery pseudoaneurysm which was the cause of her hemobilia. The patient was ultimately treated with selective coil embolization and interval cholecystectomy.
Introduction
Splanchnic artery pseudoaneurysms are rare but important vascular malformations, which may present with massive upper gastrointestinal (GI) bleeding due to hemobilia. The hepatic artery and its branches are the second most common site of splanchnic artery aneurysms, with pseudoaneurysms accounting for over 50% of cases in the reported literature.1,2 These are most often due to iatrogenic or traumatic causes but may also develop as a sequela of periarterial inflammation, such as cholecystitis.2–5
Case presentation
A 72-year-old woman presented with severe acute epigastric pain associated with nausea and vomiting. Her medical history was significant for an aortic valve replacement with a biologic valve and MAZE procedure for treatment of atrial fibrillation 6 months ago, on chronic anticoagulation with warfarin. She had no prior abdominal surgeries. She was afebrile with vital signs within normal limits. Initial exam was notable for mild epigastric pain on palpation and a negative McBurney’s sign. Her liver function testing was pertinent for transaminitis—aspartate transaminase (AST) 122 U/L, alanine transaminase (ALT) 80 U/L, alkaline phosphatase 295 U/L, total bilirubin 2.9 mg/dL, and lipase 240 U/L. Hemoglobin was noted to be 10.9 g/dL, white blood cell count (WBC) was 9300/mcL, and international normalized ratio (INR) was 3.6. An abdominal ultrasound was obtained as the initial imaging study due to the patient’s acute on chronic renal failure (glomerular filtration rate (GFR) 48 mL/min). The ultrasound noted cholelithiasis which was described as echogenic material. There was no gallbladder wall thickening or ductal dilation noted.
Overnight, she became hypotensive and developed an acute leukocytosis, with her WBC increasing to 22,000/mcL. Gastroenterology was consulted and planned for endoscopic retrograde cholangiopancreatography (ERCP) the following day after reversal of her INR. She was given 2 units of fresh frozen plasma and 10 mg of intravenous (IV) vitamin K. She was placed on continuous IV fluids for resuscitation and broad-spectrum antibiotics. The following morning, her hemoglobin had acutely decreased to 4.9 g/dL. Clinically, there was no evidence of overt show of blood. As she was already scheduled for ERCP, she was transfused 2 units of packed red blood cells, and scheduled for diagnostic esophagogastroduodenoscopy (EGD) prior to ERCP.
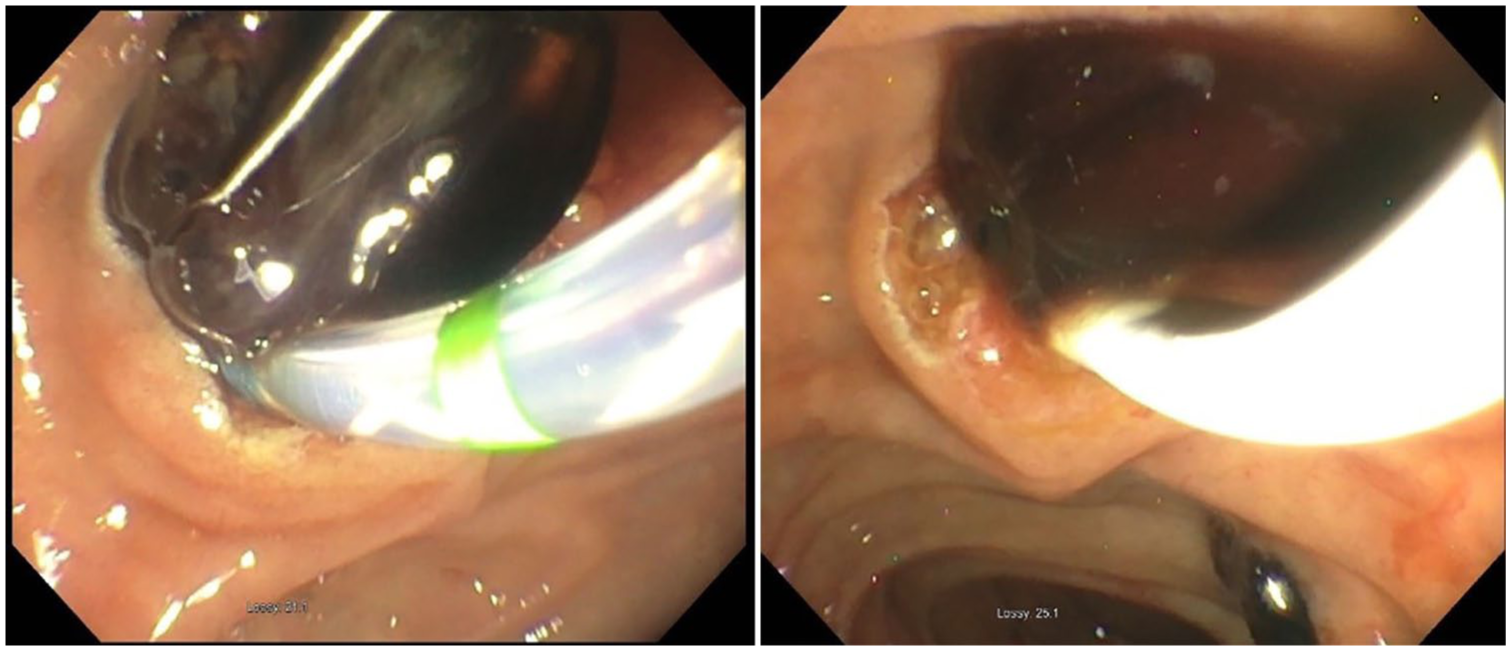
EGD noted a 1.5-cm duodenal ulcer in the bulb. The ulcer was not bleeding but was prophylactically treated with epinephrine around the ulcer and an endoclip deployed on the ulcer (Figure 1). Once ERCP was started prior to making a sphincterotomy, there was evidence of heme material being expelled from the ampulla of Vater along with stones (Figure 2). After sphincterotomy and balloon sweeps of the common bile duct (CBD) were performed, a large amount of blood and clots were removed (Figure 3). A 10 × 80 mm covered metal stent was then placed in the CBD (Figure 4). A stat computed tomography (CT) scan with contrast was then obtained to evaluate for the source of bleeding, revealing a pseudoaneurysm adjacent to the gallbladder with a pericystic hematoma (Figure 5). Overnight, the patient’s hemoglobin remained stable, and there was no evidence of ongoing bleeding. Based on the CT scan results, the patient underwent an emergent celiac angiogram by the Interventional Radiology team, and no active extravasation noted. The pseudoaneurysm was found to originate just distal to the sixth and seventh branches of the right hepatic artery. Superselective catheterization was performed, with coil embolization of the pseudoaneurysm (Figure 6). Distal perfusion was demonstrated on completion imaging via collateral flow. The patient’s condition stabilized with no additional episodes of GI bleeding. She subsequently underwent partial cholecystectomy which had to be converted from laparoscopic to open surgical repair due to severe inflammation. The patient continued to do well postoperatively and was discharged in stable condition post surgery.

Left: duodenal ulcer with adherent clot. Right: endoclip deployment with hemostasis.

Hemobilia noted from papilla prior to sphincterotomy.
Blood clots and stones noted after balloon sweeps.

Post-CBD stenting without further evidence of hemobilia.

CT angiogram showing the right hepatic pseudoaneurysm and biliary stent with no evidence of active extravasation.

Left: selective hepatic artery angiogram showing the right hepatic artery pseudoaneurysm. Right: no filling of the pseudoaneurysm after transarterial coil embolization with distal branch filling via collateral flow.
Discussion
Splanchnic artery aneurysms comprise 1% of all cases of arterial aneurysms, with hepatic artery aneurysms comprising 20% of these cases. Hepatic artery aneurysms can present as abdominal pain (55%), GI bleeding (46%), jaundice (9%), palpable mass (6%), or hemodynamic shock (7%), or be asymptomatic (2%). 2 Pseudoaneurysms comprise over 50% hepatic artery aneurysms, which are distinct from true aneurysms as they do not involve the entire arterial wall but rather a focal defect in the artery surrounded by fibrotic material, thus forming a false layer. 3 Arterial trauma or iatrogenic injury is the most common etiology in most reported cases of hepatic artery pseudoaneurysms.6–9
Hepatic artery pseudoaneurysms from iatrogenic causes are often associated with percutaneous biliary procedures or surgeries.1,2,4,6,8–11 There have been reports with both plastic and bare metal biliary stents causing injury.12–14 Pseudoaneurysms due to infectious or inflammatory conditions are much less common.2,4,7,11,15 The first case of a right hepatic artery pseudoaneurysm associated with cholecystitis leading to hemobilia was reported by Akatsu et al. 4 in 2004. Severe inflammation causing adjacent arterial wall degeneration is proposed as the mechanism resulting in pseudoaneurysm formation. Previous reports have described a similar etiology and presentation for cystic artery pseudoaneurysms.16–18
Hemobilia can be asymptomatic, as is often the case with melena, or could present as a massive GI bleed with hematemesis. The term “hemobilia” was first reported in 1948 by Sandblom representing a blood vessel communicating with the biliary tree usually due to trauma leading to hemorrhage and blood flowing along with the bile into the duodenum. Due to advancement in endoscopic procedures, it is frequently diagnosed usually reported as a triad of abdominal pain, jaundice, and upper GI hemorrhage, all three reported in 22%–80% of patients.11,17,19 Once blood enters the biliary tree, its presentation depends on the rate of bleeding. If the bleeding is brisk, it could present as hematemesis or melena and even manifest as a lower GI bleed. When it is slower, it could lead to clot formation and obstruction in the common biliary tree presenting as jaundice. 11
More than 90% of upper GI bleeding is due to alimentary canal related etiologies. Upper endoscopy remains an important and commonly performed initial diagnostic test to rule out common causes such as gastric ulcers and variceal bleeding. Moreover, drainage of blood from the papilla is also confirmatory of hemobilia, but it does not locate the exact site of bleeding. 20 Color Doppler ultrasound of the right upper quadrant can be useful as an initial diagnostic test as it is fast, affordable and can evaluate the gallbladder and any associated masses which could raise concern for an aneurysm. 17 CT imaging, while useful in imaging wall thickening of the gallbladder, is not very useful in demonstrating aneurysms or bleed without the use of iodinated contrast. CT with contrast enhancement can be more helpful to evaluate for active bleeding and aneurysmal degeneration but could miss aneurysms <1 cm in diameter.19,20 Hepatic angiography remains the gold standard for diagnosis. The role of angiography in GI bleeding has been well known since 1960 when angiography was first used to demonstrate GI bleeding. It is reported to identify vascular abnormalities in more than 90% of cases of hemobilia. 11 There have been no reported cases of biliary stenting as potential treatment or tamponade for acute hemobilia due to cystic or hepatic artery pseudoaneurysms. In one previously reported hepatic artery pseudoaneurysm caused by chronic cholecystitis, the patient was taken for emergent angiography with transcatheter arterial embolization (TAE). 4
Due to the rarity of the condition, there are no treatment guidelines available. Initial management should be directed at stabilization of the patient as in any case of bleeding and interventions to control bleeding. In review of the available literature of right hepatic artery pseudoaneurysms and similar cases, TAE has been an effective and safe treatment, including in cases involving rupture of the pseudoaneurysm.4,6–8,10–12,19 The success of TAE is reported to be 80%–100%. Alternatively, in patients who are good surgical candidates or have evidence of cholecystitis, cholecystectomy with aneurysmal repair or arterial ligation is the procedure of choice. 11 Due to advancement of interventional endoscopic procedures, the possibility of biliary stenting for tamponade effect could also be a potential management option in the future.
Conclusion
Pseudoaneurysm of the right hepatic artery is a rare diagnosis, often related to prior surgery or trauma and less commonly due to chronic infection or inflammation. Patients presenting with new onset upper GI bleeding and evidence of obstructive jaundice should raise the concern for possible hemobilia. Appropriate workup should include abdominal imaging, as well as endoscopy to evaluate for GI bleeding and possible ERCP. If hemobilia is confirmed on endoscopy, then consideration should be given to bile duct stenting as a temporizing measure. Resuscitation and timely control of bleeding is of utmost importance in such patients. Ultimately, as in our case, TAE has been shown to be an effective and safe treatment for ruptured splanchnic pseudoaneurysms.
Footnotes
Acknowledgements
This study was carried out in accordance with the Declaration of Helsinki.
Author contributions
M.D. and S.W. wrote the manuscript and reviewed the literature. F.-H.V. and R.N. reviewed the literature and made critical revisions to the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
M.D. is the guarantor of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.