
Abstract
Although basal cell carcinoma is the most common malignancy in humans, intravascular basal cell carcinoma is rarely reported in the literature. A 78-year-old male presented for Mohs Micrographic surgery of a 1.5 by 1.5 cm2 nodular and focally infiltrative basal cell carcinoma on the left parietal scalp. In the fifth stage, intravascular tumor cells were noted, and the patient was still positive in five out of six specimens with a defect measuring 6.5 × 7.0 cm2. Mohs surgery was stopped due to concern of widespread disease. A positron emission tomography/computed tomography scan was ordered that demonstrated diffuse prominent activity in the cervical level IIa nodes, right sacrum, right scapula, and the third left rib, concerning for metastatic disease. This case emphasizes the importance of vigilance to examine high-risk basal cell carcinoma pathology for intravascular invasion in addition to perineural invasion, especially in the setting of high risk factors for metastatic basal cell carcinoma.
Keywords
Introduction
Although basal cell carcinoma (BCC) is the most common malignancy in humans, intravascular BCC is rarely reported in the literature. Due to its rarity, there are no guidelines on the management of this entity. We report a case of BCC on the scalp treated with Mohs micrographic surgery with histologic evidence of local intravascular invasion and distant metastases.
Case report
A 78-year-old immunocompetent Caucasian male with past medical history of numerous BCCs and malignant melanoma of the right posterior shoulder (0.26 mm Breslow depth treated with wide local excision in 2010) presented with an asymptomatic, crusted, pink plaque of unknown duration on the left parietal scalp measuring 1.5 × 1.5 cm2. Shave biopsy revealed a nodular and focally infiltrative BCC. He was referred to the Mohs Surgery clinic for treatment.
The patient had a past medical history of multiple aggressive scalp BCCs. Five years prior he underwent Mohs surgery for two BCCs on the left and right parietal scalp. The left parietal scalp BCC recurred 18 months later and he was treated at an outside plastic surgery clinic with a wide local excision. He developed a BCC on the vertex scalp 9 months after that which was treated with Mohs surgery. Due to extension to bone, the patient also underwent adjuvant radiation therapy.
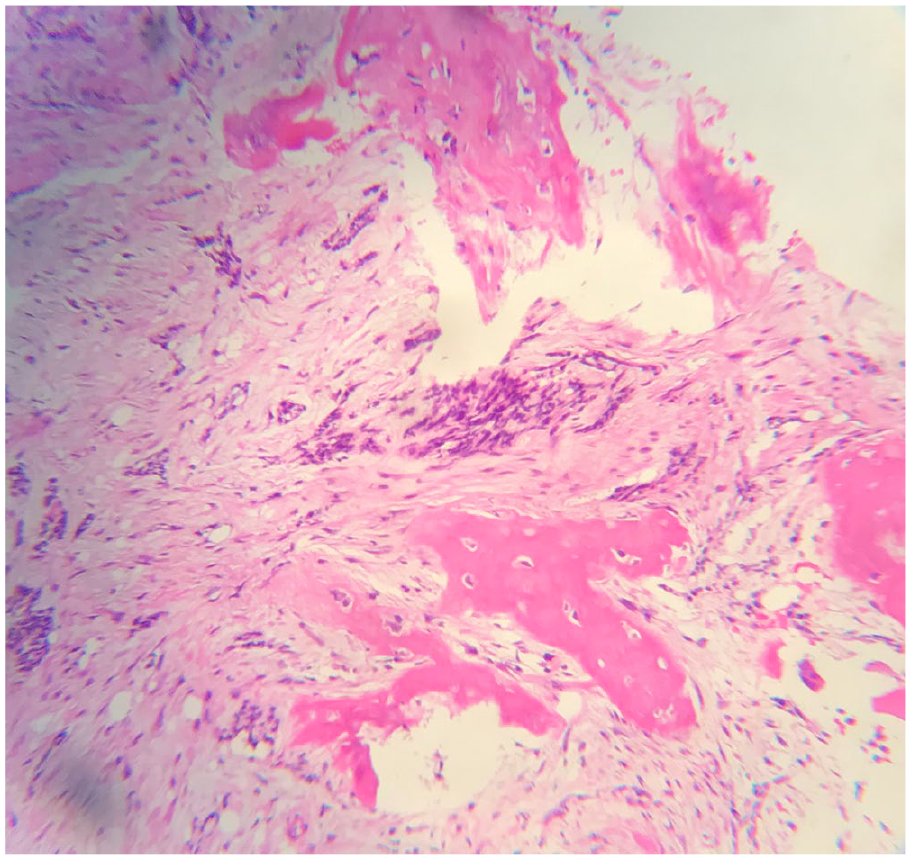
Mohs surgery was initiated for the most recent recurrent BCC on the vertex of the scalp (Figure 1). Frozen section analysis revealed diffuse infiltrative BCC in the dermis and subcutaneous fat. In the fifth stage, intravascular tumor cells were noted (Figure 2), and the patient was still positive in five out of six specimens with a defect measuring 6.5 × 7.0 cm2 (Figure 3). Intravascular invasion, with CD31(+) and CD34(+) vascular channels, was confirmed with permanent sections by a board-certified dermatopathologist. No evidence of perineural involvement was seen in the sections examined.

Preoperative clinical photograph.

Intravascular invasion on frozen section (hematoxylin and eosin, 40× magnification).

Clinical photograph of Mohs defect after fifth stage of resection.
Mohs surgery was stopped given the concern for widespread disease of the scalp and inability to attain a clear margin. A positron emission tomography/computed tomography (PET/CT) scan was ordered to evaluate for metastatic disease. The PET/CT scan demonstrated diffuse heterogeneous moderate tracer distribution in the left scalp wound favoring malignant involvement with an overlap of activity into the left parietal bone with erosion of the cortex, favoring osseous involvement. Prominent activity was last noted in the left cervical level IIa nodes, right sacrum, right scapula, and the third left rib, concerning for metastatic disease. A right sacral ala biopsy showed infiltrating nests of basaloid tumor cells in a sclerotic stroma, consistent with metastatic BCC (Figure 4). After discussion at a multidisciplinary tumor board involving head and neck surgery, radiation oncology, and medical oncology, he started vismodegib 150 mg daily. Repeat PET/CT scan 6 months later showed decrease in the activity of right sacrum metastatic lesions, consistent with response to treatment, and stable cervical IIa nodes. However, there was an interval new subcutaneous focus over the right cheek suggestive of new BCC development, which is being managed with vismodegib at this time.
Sacral ala core biopsy demonstrating nests of basaloid tumor cells (hematoxylin and eosin, 40× magnification).
Discussion
Despite the high incidence of BCC in the general population, metastatic BCC is rarely encountered with an estimated incidence of less than 0.1% and 300 cases reported in the literature. 1 The most frequent locations of metastasis are lungs and then bone; thereafter, the incidence decreases substantially to skin, liver, kidney, and spleen. 2
Of reported cases of metastatic BCC, there is an approximate 50:50 distribution in reported hematogenous versus lymphatic routes of metastases. 2 Despite this rate, histologic intravascular invasion of BCC is rarely reported. While four relatively recent case reports describe intravascular invasion BCC in the setting of non-metastatic disease,3,4 a case series published in 1984 noted intravascular invasion in three of the five patients with metastatic BCC. 2 Risk factors for metastatic spread of BCC include male sex, location on the head and neck and in particular the scalp, larger size, and recurrence of tumor after excision.1,2 Metastatic BCC has an average age of onset from 45 to 59 years, median time of onset of 9 months after diagnosis of primary tumor, and median survival of 10–14 months. 1 The 5-year survival is estimated to be 10%. 3
There are no specific guidelines for the management of intravascular or metastatic BCC. Because of the unusual pattern and rarity of metastasis and intravascular invasion in BCC, it is unclear whether intravascular invasion poses a risk for metastasis or recurrence. In contrast to intravascular invasion, perineural invasion (PNI) is well documented and is listed as a high-risk feature in the American Joint Committee on Cancer (AJCC) TNM staging of BCCs. While National Comprehensive Cancer Guidelines (NCCN) guidelines recommend adjuvant radiation therapy and imaging for high-risk BCC with negative margins but with extensive perineural involvement, no guidelines currently exist for adjuvant treatment or diagnostic measures in a patient with lymphatic or intravascular invasion. In cases of BCC with lymphatic or intravascular invasion, the use of sentinel lymph node biopsy could be considered. 2 Given the rarity of this condition, however, the benefit has not been evaluated. In addition, while the utility of PET imaging for BCCs is questioned in some studies, 5 in our patient, there was a clear benefit as it detected metastatic disease. For patients with the unique finding of intravascular BCC, PET imaging may be useful for detecting metastatic disease and monitoring disease progression.
Optimally, these cases can be presented at a tumor board with multidisciplinary input from head and neck surgery, radiation oncology, and medical oncology. There may be a role for smoothened inhibitors for metastatic BCC, although the data are minimal.
This case emphasizes the importance of vigilance to examine high-risk BCC pathology for intravascular invasion in addition to PNI, especially in the setting of high risk factors for metastatic BCC such as male sex, location on scalp, recurrent tumor, and/or large size.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for patient information and images to be published were provided by the patient.