
Abstract
Introduction and objectives:
The main objective of this article is to present and discuss a case of localized ulcerative nodular amyloidosis with deep involvement clinically manifesting as ulcerative panniculitis and discuss its impact on the choice of treatment.
Methods and results:
We present a 73-year-old woman with a history of painful ulcerated nodules on the inferior limbs. Microscopy confirmed amyloid deposits deep in the dermis and subcutaneous fat. No systemic involvement was found. Considering that skin-directed treatments often are not able to reach subcutaneous fat or were contraindicated because of the ulcers, she was successfully treated with cyclophosphamide and prednisone.
Conclusion:
Localized ulcerative nodular amyloidosis with deep involvement is a rare clinical presentation that can present as ulcerative panniculitis. Such a clinical manifestation might be misleading. Systemic treatment might be necessary to control symptoms when conventional skin-directed therapies are contraindicated.
Keywords
Introduction
Primary cutaneous nodular amyloidosis is a rare form of localized cutaneous amyloidosis presenting as waxy infiltrated plaques and nodules. 1 Its clinical appearance sometimes resembles that of systemic amyloidosis. 1 Secondary ulcers have rarely been described.
We aim to discuss a case of localized ulcerative nodular amyloidosis with extensive involvement of dermis and subcutaneous fat clinically manifesting as ulcerative panniculitis and discuss its impact on the choice of treatment.
Case report
A 73-year-old woman presented with a history of painful ulcerated nodules on lower limbs slowly progressing over a 7-month period (Figure 1). Vascular investigation was normal. She had been taking methotrexate for 2 years for a seronegative arthritis. She had had an aortic valve replacement the preceding year as well as a history of pulmonary embolism.

Painful ulcerated nodules on the inferior limbs slowly progressing over a 7-month period.
Skin biopsy of lesions revealed amyloid deposits deep in the dermis and subcutaneous fat (Figure 2) (Figure 3). Amyloid deposits were of the amyloid light-chain (AL). Monoclonal plasma cells were found around blood vessels, and monotypic kappa light-chain restriction was observed (Figure 4). Immunochemistry failed to reveal underlying cutaneous lymphoma. 2

Amyloid deposits deep in the dermis and subcutaneous fat on H&E.
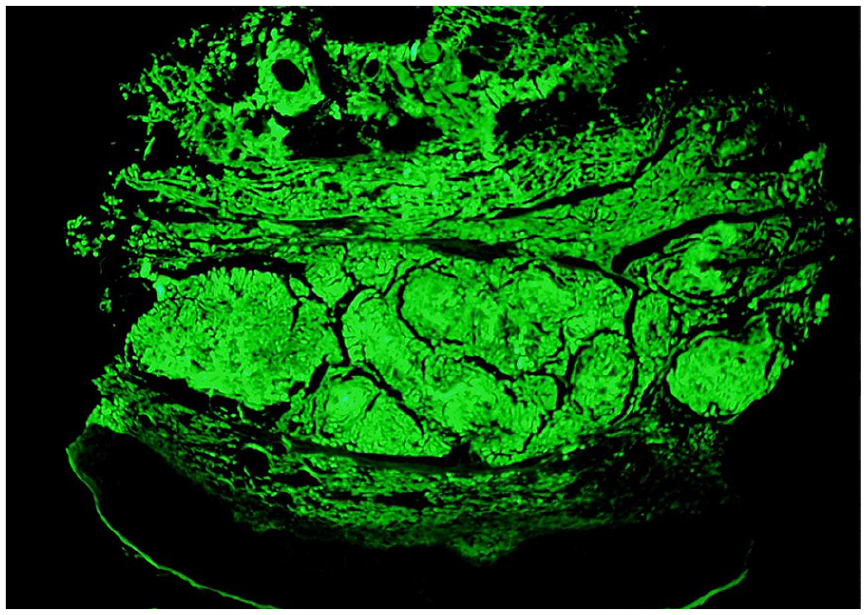
Amyloid deposit on thioflavine immunofluorescence.

Plasma cell perivascular infiltrate on H&E. Monotypic kappa light-chain restriction was observed on immunohistochemistry.
Patient presented with elevated serum light chains kappa and elevated troponins. However, cardiac magnetic resonance imaging was normal as well as microscopic re-evaluation of aortic valve for amyloid deposits. Biopsy of abdominal fat, renal function, bone marrow biopsy and positron emission tomography scan were unremarkable. Ultimately, investigation did not show evidence of systemic amyloidosis or multiple myeloma, and patient was found to have an ulcerated form of primary cutaneous nodular amyloidosis.
Lesions were too deep to consider conventional skin-directed treatments such as cryotherapy, electrodesiccation or CO2 laser. The wide extent of lesions contraindicated surgical excision. Steroid injections and radiotherapy were avoided because of infection risk related to the ulcers. Methotrexate was stopped, but lesions kept nonetheless progressing. The patient was then treated with cyclophosphamide and prednisone. Ulcers slowly healed after a 12-month period. The patient remained free of disease after 1 year of follow-up.
Discussion
Primary cutaneous nodular amyloidosis is a rare form of localized cutaneous amyloidosis. 1 It usually presents as waxy infiltrated plaques and nodules, most commonly on the trunk or extremities. 1 Secondary ulceration has rarely been described. 1
It is a disease that occurs predominantly in women, with a mean age at diagnosis of 60 years. 3 It has sometimes been described in association with systemic diseases such as Sjögren syndrome, 4 diabetes mellitus and CREST syndrome. 5 Two cases of concomitant paraproteinemia have also been reported.1,3–6
Histopathologic analysis classically shows amyloid deposits diffusely infiltrating dermis, subcutis and blood vessel walls. 7 In nodular amyloidosis, a monoclonal population of plasma cells produces the amyloid protein, 6 the latter being of the light-chain (AL) type (λ, κ or both). 7 Gene rearrangement studies confirm clonality of the amyloid-producing plasma cells in the skin but not in the bone marrow. 7
In our case, clinical presentation was misleading. Lesions presented as deep painful nodules instead of asymptomatic waxy plaques and were secondarily ulcerated, which is an unusual presentation for cutaneous nodular amyloidosis. Methotrexate might have been involved to some extent in the ulceration process. However, lesions did not heal when the medication was stopped and histopathologic findings did point towards classic presentation of methotrexate-induced ulcers.
In the absence of an underlying treatable cause, the management of localized cutaneous nodular amyloidosis is difficult, as there is no consistently effective treatment. Various modes of treatment have been reported for improving the appearance of lesions, such as surgical excision, cryotherapy, electrodesiccation and curettage, intralesional steroid injection and, more recently, treatment with the CO2 laser. 7 Radiotherapy has also been reported with mitigated results. 8 Unfortunately, the rate of local recurrence in this type of amyloid is high. 7
In our case, lesions were too deep to consider skin-directed treatments. The wide extent of lesions contraindicated surgical excision. Steroid injections and radiotherapy were avoided because of infection risk related to the ulcers.
Patient had a paraproteinemia as well as elevated troponins but did not have enough criteria for a diagnosis of myeloma or systemic amyloidosis. However, normalization of those biological parameters with systemic therapy might indicate subclinical systemic disease.
In patients with localized cutaneous nodular amyloidosis, reported progression rate to systemic disease is 50%. 1 However, more recent case studies seem to indicate that it is more around 6%.5–6 Patients presenting concomitant paraproteinaemia at the time of diagnosis seem to be more at risk. 6 It is not known whether the presence of ulceration alters the risk of progression to systemic disease. In our case, no cutaneous recurrence and no systemic progression was observed 1 year after clinical remission. Localized ulcerative nodular amyloidosis with deep extensive involvement is a rare clinical presentation that can present as an ulcerative panniculitis. Its clinical manifestation might be misleading and clinicians should be alert of its existence. In this case, methotrexate might have also been involved in the ulceration process. Deep involvement of amyloid deposits along with the ulceration process may contraindicate conventional treatments. Systemic treatment might be necessary to control symptoms. Long-term follow-up is necessary, since the risk of systemic development of this deep ulcerated form is unknown.
Footnotes
Authors’ Note
Poster presented at the World Congress of Dermatology (June 2019) and at the Canadian Dermatology Association Conference (June 2019).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed patient’s consent has been obtained for publication of the images and case report information.