
Abstract
We herein describe a 38-year-old woman with Marfan syndrome and chronic type A aortic dissection. Computed tomography showed that the sinus of Valsalva and thoracoabdominal aorta had a diameter of 62 and 55 mm, respectively. After 7 months of a Bentall operation and total arch replacement with the elephant trunk technique, we performed thoracic endovascular aortic repair for an aneurysm of the descending aorta, but we preserved the retrograde flow into the false lumen because it supplied vessels perfusing the spinal cord. Computed tomography angiography 14 months after thoracic endovascular aortic repair showed that the thoracic aortic diameter had increased to 68 mm. We then performed partial (proximal only) coil embolization of the false lumen. After 6 months, the thoracic aortic diameter had decreased to 60 mm and the spinal cord remained perfused via the distal false lumen. Staged coil embolization after thoracic endovascular aortic repair for aneurysmal chronic type B aortic dissection is feasible and can be beneficial.
Keywords
Introduction
Patients with acute type B aortic dissections have recently been undergoing treatment with endovascular therapy. 1 However, endovascular therapy for a chronic type B aortic dissection with aneurysmal progression is controversial because the thrombogenic environment in the false lumen is incomplete due to retrograde flow through the residual re-entry tear.2,3
We herein present an endovascular approach using a combination of coil embolization with preservation of flow to major organs in a patient with a chronic type B aortic dissection and aneurysmal progression.
Case report
A 38-year-old woman with Marfan syndrome was referred to our hospital for treatment of a chronic type A aortic dissection. Computed tomography (CT) revealed that the diameter of the sinus of Valsalva and thoracoabdominal aorta was 62 and 55 mm, respectively (Figure 1(a)–(c)). We performed a Bentall operation and total aortic arch replacement with the elephant trunk technique. The elephant trunk was an 18 mm × 8 cm woven graft (Figure 1(d)). We subsequently planned thoracoabdominal aortic graft replacement. However, the patient refused to undergo this procedure because of the large operative wound and long hospitalization period. After 7 months of the first operation, we performed thoracic endovascular aortic repair (TEVAR) for the descending thoracic aortic aneurysm via right common femoral artery exposure. Two GORE TAG Thoracic Endoprostheses (28 mm × 15 cm and 34 mm × 20 cm; W.L. Gore & Associates, Inc., Flagstaff, AZ, USA) were placed 4 cm distal to the origin of the left subclavian artery to immediately proximal to the celiac artery. The false lumen supplied the vessels perfusing the spinal cord. Therefore, to prevent paraplegia, we preserved retrograde flow into the false lumen. Despite TEVAR, the diameter of the thoracic aorta was found to have increased to 68 mm by follow-up CT angiography 14 months after TEVAR. We decided to perform coil embolization for the false lumen. Coils were placed under local anesthesia through percutaneous femoral access. After obtaining femoral access, a 4-Fr multipurpose Berenstein catheter was advanced into the false lumen. After inserting two coils as anchors into the false lumen, eight more were inserted as embolic material (IDC, Interlock; Boston scientific, Marlborough, MA, USA; Tornade; Cook Medical, Bloomington, IN, USA) (Figure 2).

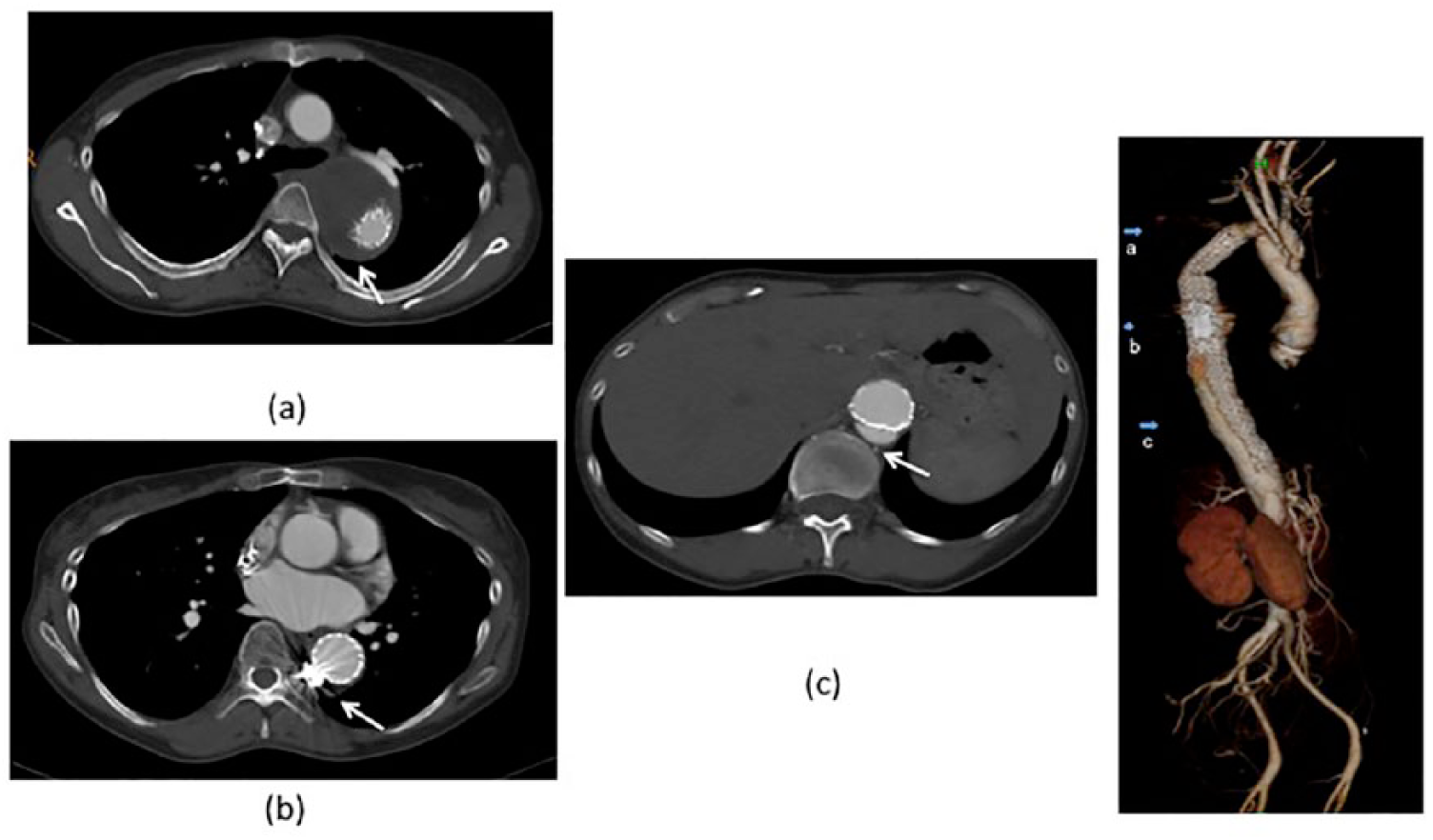
(a)–(c) Preoperative computed tomography images of the aorta of a woman with Marfan syndrome. The diameter of the sinus of Valsalva was 62 mm (panel b) and that of the thoracoabdominal aorta was 55 mm (panel c). (d) Postoperative computed tomography shows the results of the Bentall operation and total aortic arch replacement with the elephant trunk technique (elephant trunk: 18 mm × 8 cm woven graft).
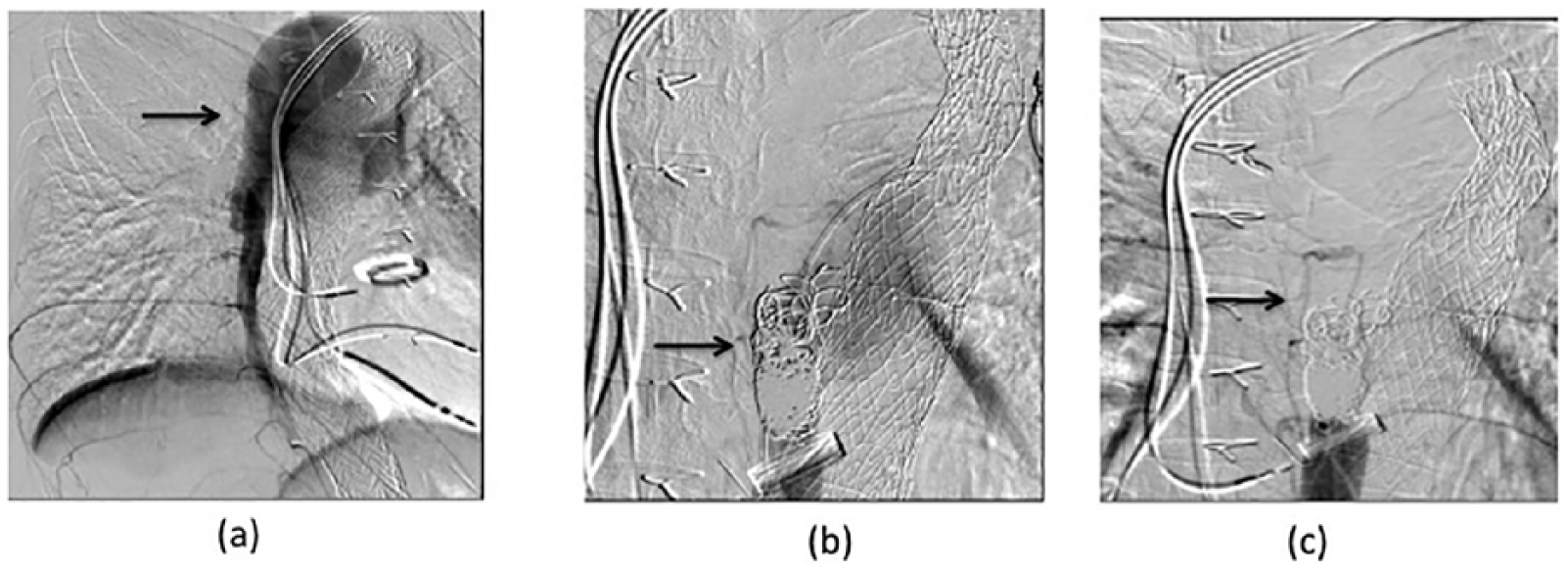
(a) Angiography shows enhancement of the false lumen. (b) Coils were placed into the aorta through percutaneous femoral access and under local anesthesia. After placing two coils as anchors, the false lumen was filled with eight more coils as embolic material. (c) The proximal false lumen was not completely enhanced, but the vessels perfusing the spinal cord (arrow) were enhanced.
After 6 months of coil embolization, CT angiography showed reduction in the thoracic aortic diameter to 60 mm and absence of enhancement of the proximal false lumen. The spinal cord still continued to be perfused from the false lumen (Figure 3).
(a, b) After 6 months of coil embolization, computed tomography angiography showed a reduction in the thoracic aortic diameter to 60 mm and absence of enhancement of the proximal false lumen. (c) The spinal cord was perfused from the false lumen (arrow).
Discussion
Endovascular treatment for acute type B aortic dissection has become common. Furthermore, endovascular treatment for prevention of antegrade flow into the false lumen in patients with acute type B aortic dissection has been performed with good results for complete exclusion of the false lumen with re-entry coverage. 1 However, endovascular therapy for chronic type B aortic dissection is not established. 4 A patent false lumen is a risk factor that affects the long-term treatment outcome in patients with chronic type B aortic dissection. In previous studies, closing only the entry tear of the false lumen with stent grafting for chronic type B aortic dissection led to an increase in the size of the false lumen.2,3 Coil embolization for a persistent false lumen after stent graft repair of type B aortic dissection has also been reported. 5 San Norberto et al. 5 found that endovascular coiling of the patent false lumen after endovascular stent graft treatment for type B aortic dissection avoided the risk of rupture or death due to secondary aneurysm formation.
In the present case, the false lumen was gradually increasing in size; however, because it was providing blood flow to major organs, we could not thrombose the entire false lumen. Therefore, our technique of staged coil embolization could be a viable treatment option for patients in whom false lumen thrombosis is not immediately possible. In our case, however, it is also critical that we continue to monitor the perfusion of the spinal cord and the aneurysm progression. Overall, staged coil embolization after TEVAR for aneurysmal chronic type B aortic dissection appears to be feasible and beneficial while also having the advantage of being less invasive.
Conclusion
The strategy of combining coil embolization and stent graft implantation may prove useful for treatment of endovascular false lumen occlusion while ensuring blood flow to major organs in patients with chronic dissection and aneurysmal progression.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.