
Abstract
Instabilities of the craniocervical junction can be of rheumatic, traumatic, or congenital origin. The reported patient has a congenital malformation of the cervical spine, which is frequently observed in patients with Klippel–Feil syndrome. Her posterior arch of the atlas (C1) is hypoplastic and a chronic subluxation of the atlanto-axial joint would be possible. Although most common fusions in Klippel–Feil syndrome patients exist at C2/3, the majority of studies about Klippel–Feil syndrome deal with pediatric or adolescent individuals. Through extreme flexion of her neck, there was a compression of the spinal cord by the odontoid process. This led to a quadriplegia lasting about 10 min. Over the following weeks, all of her symptoms started to diminish. This situation turned out to be the third episode involving temporary neurological disorders in this 60-year-old female’s life.
Introduction
Craniocervical instability can result from rheumatic diseases, and either direct or indirect trauma to the cervical spine or head. 1 Moreover, they can be of congenital origin. The Klippel–Feil syndrome (KFS) is characterized by congenitally fused cervical vertebrae. Many patients do not have the complete triad of a short neck, a low posterior hairline, and a decreased range of motion in the neck. As a result of this, the clinical diagnosis is frequently disguised and hints at KFS are only given by radiological images. 2 Most fusions are between C2 and C3 in individuals with KFS. 3 If the craniocervical instability is a function of a congenital malformation, individuals either never become apparent of the neurological symptoms or were most likely aware of them early in their lives.4,5
We report on a 60-year-old female Caucasian patient, who was not aware of her malformation of the posterior arch of the atlas (C1), although there had been two other alarming events of neurological disorder in her lifetime. During Yoga practice, the patient suffered from a quadriplegia after a maximum flexion of her neck. Symptoms were already in regression when she came to our clinic. Nevertheless, she avoided any movement in her cervical spine for 4 days. Radiological imaging showed a hypoplastic atlas (C1) and a basilar invagination.
Taken together, the congenital variation led to the narrowing of the vertebral canal during vigorous flexion of the neck. To our knowledge, there has been no other case in the medical literature of someone with a congenital malformation, that is, of one occurring without obvious symptoms of disease, and of one provoking a quadriplegia by deliberate flexion of the neck. Also, it is not known to be a regular feature of KFS.
Description of the case
A 60-year-old female visited the emergency department (ED) of our hospital. She suffered from quadriplegia for 10 min after maximal flexion of her neck during Yoga practice. For 30 min, the patient was neither able to walk nor to stand. Thus, she was admitted to the hospital by first aid responders. In the ED, she still felt a tickling pain and numbness on the entire right side of her body. No motoric degradation was observed in the upper or lower limbs. Bowl and bladder function were found to be physiologically normal.
The patient reported to us that she had two similar events in the past—once at age of 21 years and another at age of 40 years. Back then, she had a paresthesia in certain body parts for 2–3 days, but never a motoric malfunction. It is obvious that she had not consulted a physician to date. These two events also occurred as a result of intense flexion in her neck. However, at that time, she did not connect the deliberate flexion movement with the subsequent numbness.
At the time of admission by ambulance, the patient could walk, stand, and showed no motoric malfunctions. All her vital signs were normal. Eye-catching was her head posture, though. She held her head straight and avoided any kind of movement in the upper cervical spine (active range of motion: extension/flexion 0-0-0°; rotation: 0-0-0°). When an object moved outside her visual range, she moved her whole body to locate it again. She still had the feeling that the whole right side of her body had less sensibility in it compared to the left. The patient sensed tickling paresthesia in her right hand, right lower leg, and right foot.
Immediately upon arrival at the ED, we conducted an angiographic computed tomography (CT) of the cerebrum and neck (Figure 1). To further investigate apoplexy diagnostics, she received a Doppler ultrasonography of the carotid arteries.

(a–c) Axial planes of the subluxated atlanto-axial joint with the malposition of the odontoid process in the native CT. (d) Angiographic CT of the head and neck. No hints of stenosis or dissection of the cerebrum-supplying arteries are observed here.
While taking a closer look at the CT scans, a series of congenital malformations were observed. The first cervical vertebra (C1) was hypoplastic and its posterior arch was completely missing. Thus, the occiput was closer to the posterior arch of C2 and the skull base was more steeply tilted to the rear. The atlanto-dental interval (ADI) was enlarged by 4.5 mm, which was an objective sign of atlanto-axial dislocation (AAD). Moreover, superior odontoid migration of 15 mm above the McGregor line was also detected. This pathological finding indicates a basilar invagination, such that these anatomical circumstances led to a narrowing of the foramen magnum and thus to craniocervical instability (Figure 2).
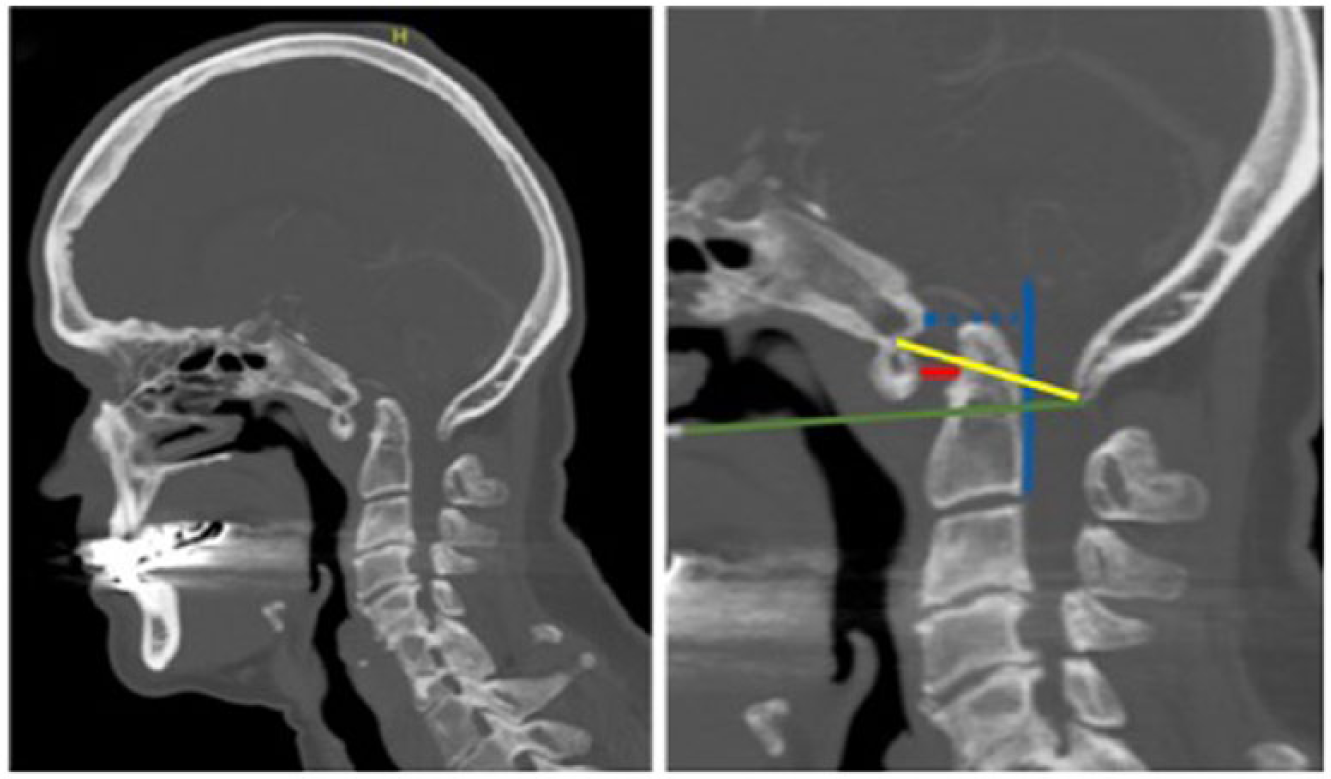
A CT scan of the odontoid process in the sagittal plane (left). Striking is the missing posterior arch of C1. One can assume a subluxated position in the atlanto-axial joint. The right image shows the AAD. The red line indicates an ADI of 4.5 mm (physiologically < 3 mm). 6 The dotted blue line depicts the basion-axial interval, which extends 15.5 mm (physiologically < 12 mm in females).7,8 The green line depicts the McGregor line. A superior odontoid migration of 15 mm can be seen, and as a result, the patient suffers from a basilar invagination. 9 The odontoid process migrated 8.8 mm above the McRae line (yellow).
On the second day of hospitalization, magnetic resonance imaging (MRI) of the cervical spine was conducted to obtain a direct view of the spinal cord. It showed a deformity of the medulla at the level of the dens axis (Figure 3). No edema was found, either in the dens axis bone or the ligaments surrounding it. No evidence of acute injury was seen on MRI either. Rather, we assumed a chronic subluxation of the odontoid process in the atlanto-axial joint. Given the missing posterior arch of C1, the spinal cord could dodge to the rear, as it had enough space in which to do that. Movements in the atlanto-occipital joint further minimized the leftover space and suggested an incarceration of non-bony structures, including the medulla (Figure 4).
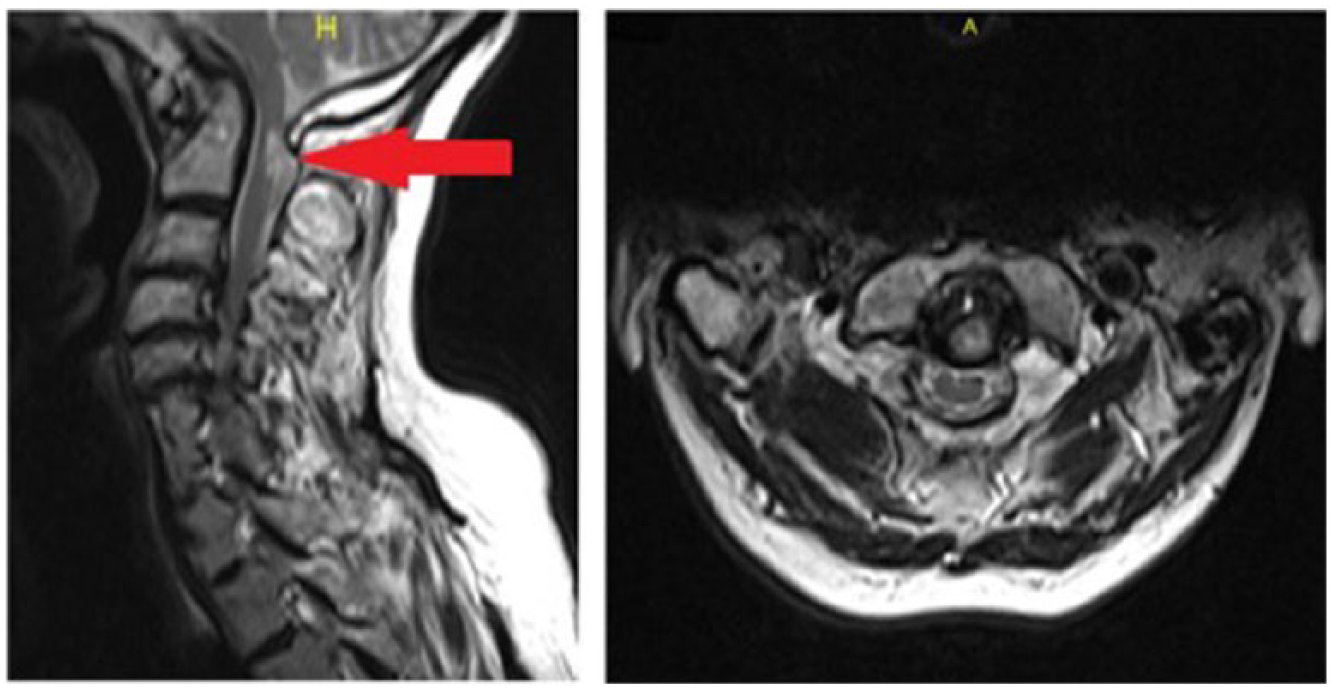
MRI of the cervical spinal column shows a chronic subluxation in the atlanto-axial joint with an impression and constriction of the foramen magnum. The arrow depicts an older deformity of the medulla. No perifocal edema is observed, which could result from a chronic compression. It is located dorsal of the odontoid process. No hints of a ligament injury can be seen, and in particular, the transverse ligament is also free of damage.

The left sketch depicts the physiological anatomy of the craniocervical junction in the sagittal plane. In the right sketch, the congenital malformation is shown with its AAD. The occipital bone slips closer to the odontoid process due to the hypogenetic posterior arch of the atlas. Furthermore, the odontoid process appears more cranial, indicating the basilar invagination. In conjunction with this scenario, the vertebral canal is narrower in its diameter than is physiologically normal, and becomes even narrower when the neck is flexed.
Dynamic X-ray images were taken in flexion and extension (Figure 5). A dislocation of the odontoid process of 4 mm was observed. This was graded as a sign of a mobile AAD. Moreover, she had a fusion of C6/7. Congenital fusions in the cervical spine are part of KFS. 10 Due to her typical phenotype and anatomical abnormalities in the cervical spine, we strongly assumed it was KFS. Specific genetic testing was indicated, but had not been carried out due to missed events in the therapeutic procedures (and was of no relevance to the patient as well). The patient had no anamnesis of polyarthritis. There was no rheumatism seen in blood testing. Sensible evoked potentials of the nervus medianus showed a normal result on both sides. In contrast, the nervus tibialis showed a prolonged stimulus conduction on both sides, with a stronger occurrence on the left side, without exact localization of the damage.
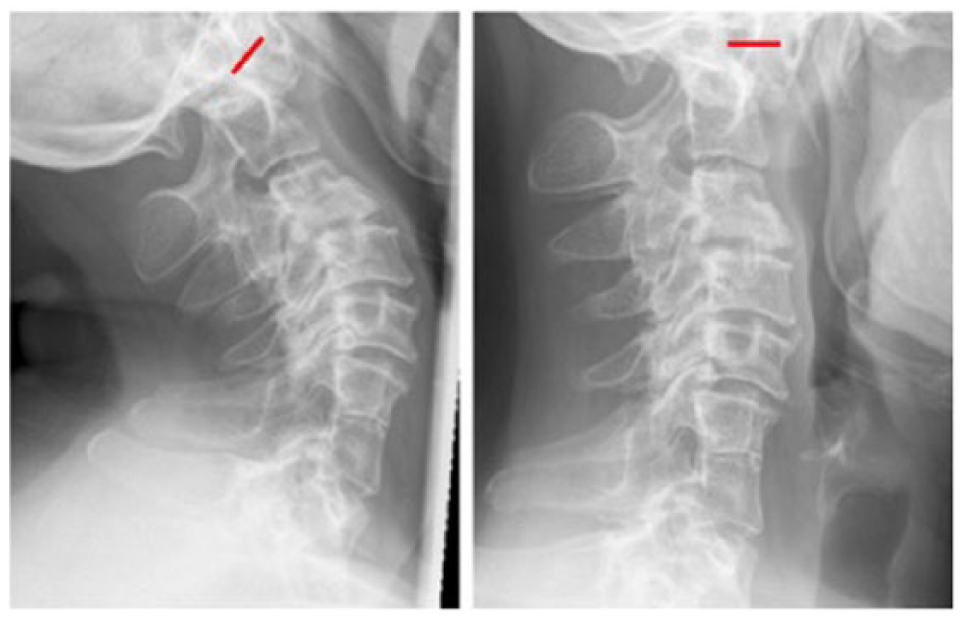
Dynamic X-rays images showing the cervical spine in active extension (left) and in active flexion (right), which is as far as possible for this patient. One can observe a congenital fusion of C6 and C7 and the missing posterior arch of C1. The ADI is indicated by the red line. A mobility of 4 mm in the ADI was observed, which indicates an AAD.
The patient received comprehensive diagnostics and conservative treatment in the inpatient clinic for 5 days. This regimen incorporated analgesia (Metamizole 500 mg) up to eight times a day. Her tingling paresthesia on the right side of her body was diminished at her release. Three months after hospitalization, she visited our outpatient clinic for a follow-up examination. The patient had no relapse of sensomotoric malfunctions and also felt no tickling paresthesia.
We informed the patient about the risk of a permanent quadriplegia and recommended a surgical stabilization. She refused any surgical therapy and preferred our alternative recommendation, that is, not to force her neck into any extreme positions.
Discussion
The congenital malformations of the reported patient are in line with KFS. In 1912, the syndrome was described as a triad of a short neck, low posterior hairline, and a limited range of motion in the cervical spine. However, the complete triad is seen in less than 50% of all cases. 6 The short neck and limited range of motion, due to fusion of the cervical vertebrae, result from a failure of segmentation of the cervical somites during gestation. 11 Moreover, the observed malformations of our patient fit type II, according to the updated classification by Samartzis et al. 7 A basilar invagination is commonly observed in patients with KFS. Only about one-third of examined patients display any neurological symptoms. 8
Very few cases of chronic subluxations of the atlanto-axial joint have been described, which do not originate from rheumatoid arthritis or direct trauma. A series of 19 patients with AAD without fracture has been reported by Hu et al. 9 The examined patients showed mild or transient neurologic deficits. The author claims that physiological functions of the nervous system will be restored without residual assistance. In this series of patients, Hu presumed that an operative intervention might be useful if the transverse ligament showed signs of instability. In our reported case, the transverse ligament appeared radiologically stable, without any discontinuity in the MRI—although the ADI was enlarged to 4.5 mm (physiologically < 3 mm). 12 Moreover, flexion/extension X-ray images showed a mobility in the ADI of 4 mm.
The patient suffered from a severe stenosis of the vertebral canal. Even if the quadriplegia lasted only for a short period, there always exists a risk of recurrence. The rare phenomenon in our patient was the missing posterior arch of C1, although it might be hypoplastic because of fusion with C2. Most common fusions in KFS patients are C2/3, but the majority of studies of KFS patients deal with pediatric or adolescent individuals. The presented patient reached age of 60 years, despite the congenital instability in her craniocervical junction.
We also assume there was a stronger ligamentotaxis when she was younger, preventing her from more severe subluxations. Chronic craniocervical instability cannot be compared to acute instability from trauma—whereas in younger patients, ligaments are more stable than in older ones, which might be why she had so few neurologic symptoms throughout her lifetime. In advanced maturity, ligaments become stiffer and less compensatory in handling the bony malformations. The enlarged ADI signals a horizontal instability. The basilar invagination is a sign of vertical instability. Furthermore, compression of the spinal cord has an influence on blood flow and perfusion capacity. A long-term reduction in perfusion might also be one cause of medulla deformation. 13 However, the patient had no coronary heart disease or peripheral arterial disease. Nevertheless, a compromise of either the anterior spinal artery or posterior spinal circulation could necessitate further diagnostics. In terms of a “systems analysis,” the craniocervical junction is severely unstable. As such, we recommend a surgical intervention with reduction, decompression, and stabilization.
Conclusion
In the ED, rapid exclusion of the frequent causes of paralysis is vital, as well as sufficient treatment for acute spinal injury. Ultimately, the patient’s abnormal anatomy, in combination with a deliberate maximal flexion of the neck, led to a quadriplegia. We found this case unique as a rare variant of KFS. In view of a possible recurrence, and because of the already existing damage to the myelon, we continued to recommend surgical stabilization. Permanent treatment with a collar would be inadequate and would not be tolerated by the patient.
Footnotes
Acknowledgements
The authors thank Carol Seitzer-Zurcher from American Manuscript Editors for editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institutions do not require ethical approval for reporting individual cases or a case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.