
Abstract
Muscle herniation in the upper extremity is a rare but recognized phenomenon with a paucity of reports in the current literature. In the majority of cases, the herniation is secondary to trauma, with some of the cases due to muscle hypertrophy and increased intra-compartmental pressure from the forced exertion. Treatment for this condition ranges from nonsurgical, repair, or reconstruction to fasciotomy of the flexor carpi ulnaris fascia. Here, we present a case of flexor carpi ulnaris herniation after an open in situ cubital tunnel release in a 57-year-old male 6 years after initial surgery. The patient’s symptoms did not improve with conservative management, and the patient subsequently underwent endoscopic fasciotomy with resolution of his symptoms and maintenance of his wrist and grip strength. The rationale for the treatment chosen is discussed.
Keywords
Introduction
Muscle herniation, also referred to as fascial herniation in some cases, was described initially by Dupuytren in the 1800s. 1 These herniations mainly occur in the leg, with the tibialis anterior being the most common muscle affected. Muscle herniation in the upper extremity is much rare, consisting of a very limited number of case reports in the English literature. 2 Furthermore, we could not find any reports of flexor carpi ulnaris (FCU) herniation following open cubital tunnel release (CuTR).
The treatment of muscle herniation has varied throughout history with many different methods being implemented successfully. These include fascia lata weave, 2 fascia lata inlay, 3 and fasciotomy. 4 The purpose of this case report is to illustrate that hand and wrist strength can be maintained with fasciotomy without reconstruction or repair of the investing fascia.
Case report
A 57-year-old male manual labourer presented with a complaint of a right forearm mass he noticed 3 years prior to presentation. The patient had a history of an open in situ CuTR 5 years previously. The patient reported that he did well in the initial post-op period, had good relief of his neurological symptoms, and was able to perform his daily activities. The mass, which was accentuated with wrist and finger flexion, was located on the ulnar side of his forearm deep to his prior CuTR scar. He also complained of discomfort when resting his forearm on a hard surface which started approximately 3 months prior to presentation with a maximum visual analogue scale (VAS) pain score of 5. He denied any trauma or inciting event. Clinical examination revealed a palpable mass over the ulnar aspect of his forearm deep to the surgical scar, with a tender area of fascia where the CuTR release had ended distally. He denied any exertional compartment syndrome–type symptoms.
The patient presented to us with a magnetic resonance imaging (MRI) ordered by his primary care physician, which was normal and did not reveal any masses. After discussing the diagnosis and treatment options, the patient wished to proceed with complete fasciotomy over the FCU.
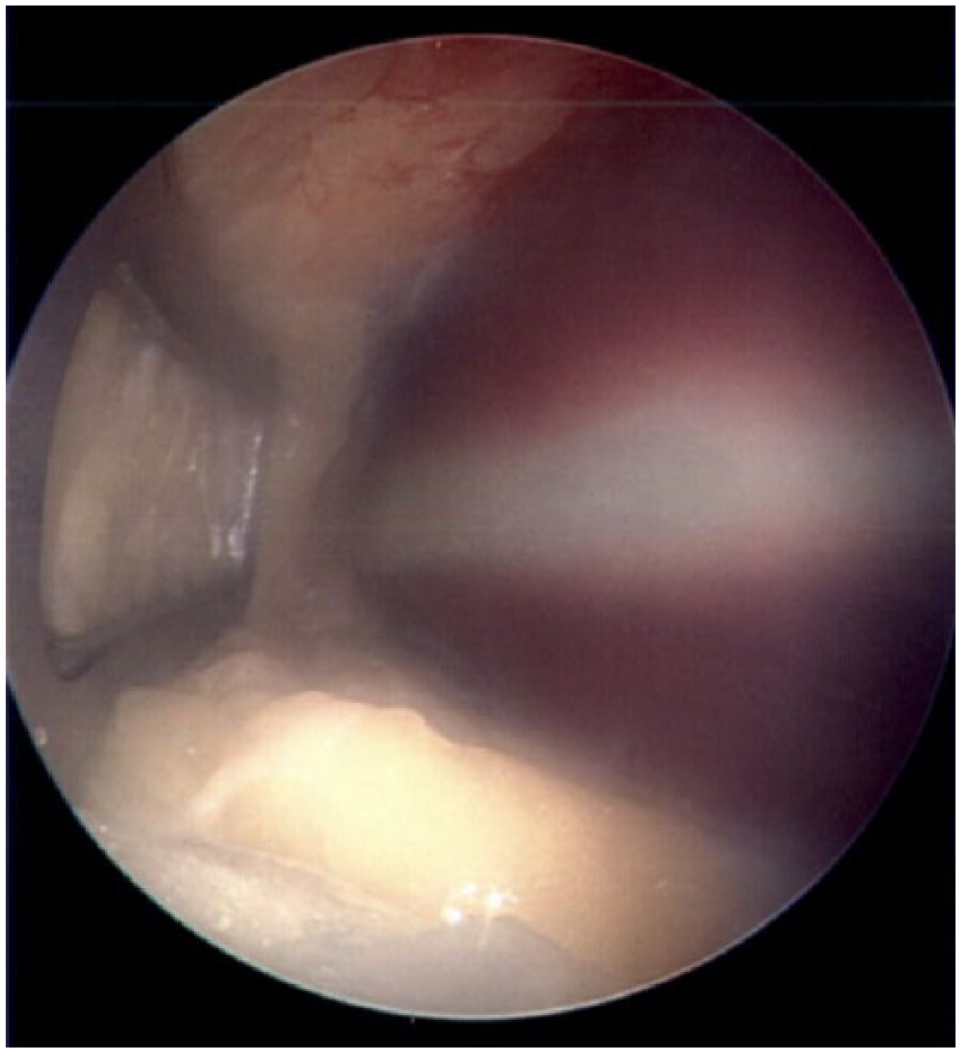
The decision was made to complete the fasciotomy distally to the FCU tendon level in order to remove the painful stimulus as well as the discrete area muscle bulge noted over the ulnar forearm. This was performed open with an endoscopic assist method. A longitudinal incision was made in the skin approximately 2 cm long, 5 cm proximal to this fascial band. The soft tissue spreaders were then placed over the forearm fascia distally to create a working space for the endoscope. The nasal speculum was then inserted into the wound under the skin and the endoscopic camera was inserted. This revealed the leading edge of the fascial herniation (Figure 1). Using long Mayo scissors, the forearm fascia over the FCU was released from a proximal to distal direction under direct visualization, taking care to preserve cutaneous nerves and veins encountered. The fascia was released distal to the forearm, near the level of the wrist when the FCU tendon was encountered (Figure 2). The endoscope was then removed from the wound along with the instruments. Palpation of the forearm revealed no fascial band leading to muscle herniation present. The patient tolerated the procedure well.

FCU herniation in the location of the prior in situ CuTR.
Complete fasciotomy performed with resolution of FCU herniation.
At the 4-month post-op visit, the patient had equal grip and wrist flexion strength, and the pain over the fascial edge had subsided. No discrete mass was evident and the patient was satisfied with the aesthetic appearance. He was able to perform his activities of daily living and occupation without issues or restrictions and his post-op VAS pain score was 0.
Discussion
Cubital tunnel syndrome is the second most common nerve compression in the upper extremity, affecting 20.9 of 100,000 people. 5 The complication rate of in situ CuTR is 3.6%, with the most common complications being instability (1.3%), recurrent cubital tunnel syndrome (0.9%), and infection (0.9%). 6 The revision rate for in situ CuTR is approximately 1.8%. 6
Controversy exists regarding the extent of release required in order to accomplish an adequate decompression of the ulnar nerve in the cubital tunnel. The current literature describes decompression of the ulnar nerve until the two FCU heads are seen as much as 4–15 cm distally to the retrocondylar groove.7 –10 The outcomes of varying degrees of release have not been described. The lack of reports in the literature leads us to believe that the degree of release may not predispose patients to FCU herniation; however, this has not been studied. Based on this case, we encourage surgeons to perform an adequate release of all constricting bands of the ulnar nerve, as we believe an associated FCU herniation to be a rare event. Lacking a history of trauma, we feel this herniation may be secondary to muscle hypertrophy which propagated the initial surgical fascial release.
We chose endoscopic release in order to minimize soft tissue disruption and to aid the preservation of the antebrachial nerves and perforating vessels of the forearm. Endoscopic fasciotomy is well described in the literature for chronic exertional compartment syndrome,11,12 but we have been unable to find any reports in the literature of this technique being used to treat muscle herniation in the extremities.
In addition, we did not detect a loss of strength in the affected upper extremity in comparison with the contralateral limb (65 lbs on the left and 70 lbs on the right with a Jamar dynamometer (Jamar II; Jamar, Bolingbrook, IL)). While reports exist of fascial reconstruction and repair, 2 fascial release may have similar clinical outcomes with lower cost and possibly lower risk of recurrent cubital tunnel syndrome.
Conclusion
Upper extremity muscle herniations are rare events, and FCU herniation after CuTR has not been reported in the literature. Surgical options include repair, reconstruction, or completion of the fasciotomy. In our case, we successfully performed an endoscopic-assisted fasciotomy with good results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.