
Abstract
A 71-year-old woman with right chest and left lumbar pain was referred to our hospital. Computed tomography showed multiple recurrent tumors in the abdominal cavity and bilateral lungs. She had already received several chemotherapies for the recurrent tumor, and palliative care would be appropriate. However, she was seeking another anti-cancer therapy. Therefore, she was told about low-dose etoposide therapy and consented to its administration. Treatment was very effective; serum tumor marker levels decreased dramatically, the pain was controlled, and the recurrent masses were shrinking. However, her recurrent tumor had become refractory again in the 22nd month of treatment.
Introduction
Platinum, taxane, and doxorubicin are the first- or second-choice drugs for endometrial adenocarcinoma. However, we have few treatment choices for repeatedly recurrent refractory tumor, and its treatment remains a challenge. Etoposide is a DNA topoisomerase II inhibitor, to which ovarian cancer that is refractory to platinum or paclitaxel demonstrates good sensitivity. 1 In the 1990s, some reports were published from Japan in which oral etoposide treatment was tolerable and effective as treatment of recurrent endometrial adenocarcinoma.2,3 However, those were case reports with low evidence levels. Moreover, two phase II trials of oral etoposide therapy for recurrent endometrial adenocarcinoma showed no significant effect and a modest effect, respectively,4,5 and no large studies were then performed. In the present case, low-dose oral etoposide therapy was given to a patient with recurrent masses that were refractory to platinum and paclitaxel, and the treatment was extremely effective and tolerable, with mild side effects.
Case report
A 71-year-old woman with performance status 2 had right chest and left lumbar pain and was referred to our hospital for treatment. The computed tomography (CT) findings in the previous hospital showed some recurrent masses and metastatic tumors: 144 × 137 × 120 mm3 mass in the left abdomen to the pelvic cavity, a 50 × 43 mm2 mass on the right pelvic wall, a 52 × 47 mm2 mass on the ascending colon, and small metastatic masses on the diaphragm and bilateral lungs (Figure 1(a)). Serum carbohydrate antigen (CA)19-9 and CA125 levels were 3128 and 96.1 ng/mL, respectively. She had a previous history of 4 years’ treatment with paclitaxel and carboplatin, docetaxel and carboplatin, doxorubicin and cisplatin, medroxyprogesterone acetate, and paclitaxel-alone chemotherapies, as well as immunotherapy for the present recurrent tumors found 5 years after standard surgery for endometrioid adenocarcinoma G1 (Stage IB). Although she and her husband were informed by the former doctor and by us that palliative care would be appropriate, they desired another anti-cancer therapy. They were therefore told about daily oral administration of half-dose etoposide (25 mg/day) that had been reported in the 1990s in Japan. They provided written, informed consent to its administration, and the therapy was then started. Treatment for 4 months reduced serum tumor marker levels and relieved her pain; however, the therapy was discontinued at the end of the fourth month at her request because of mild to moderate stomachache, and serum tumor marker levels increased again. Therefore, the same treatment was quickly restarted. Serum CA19-9 and CA125 levels decreased dramatically to around 110 ng/mL and the normal range, respectively (Figure 2), and CT showed shrinkage of the recurrent tumors (Figure 1(b)). She became cheerful with a good appetite and bowel habit, with slight lumbar pain. However, the tumor marker levels gradually increased in the 22nd month of treatment, and she again complained of lumbar pain. The CT findings indicated tumor growth (Figure 1(c)). Her recurrent tumor had become refractory again. They asked for another chemotherapy regimen, and weekly paclitaxel and carboplatin chemotherapy was tried. However, it was ineffective. She developed genital bleeding, her serum tumor marker levels further increased, and she died suddenly from pulmonary embolism.
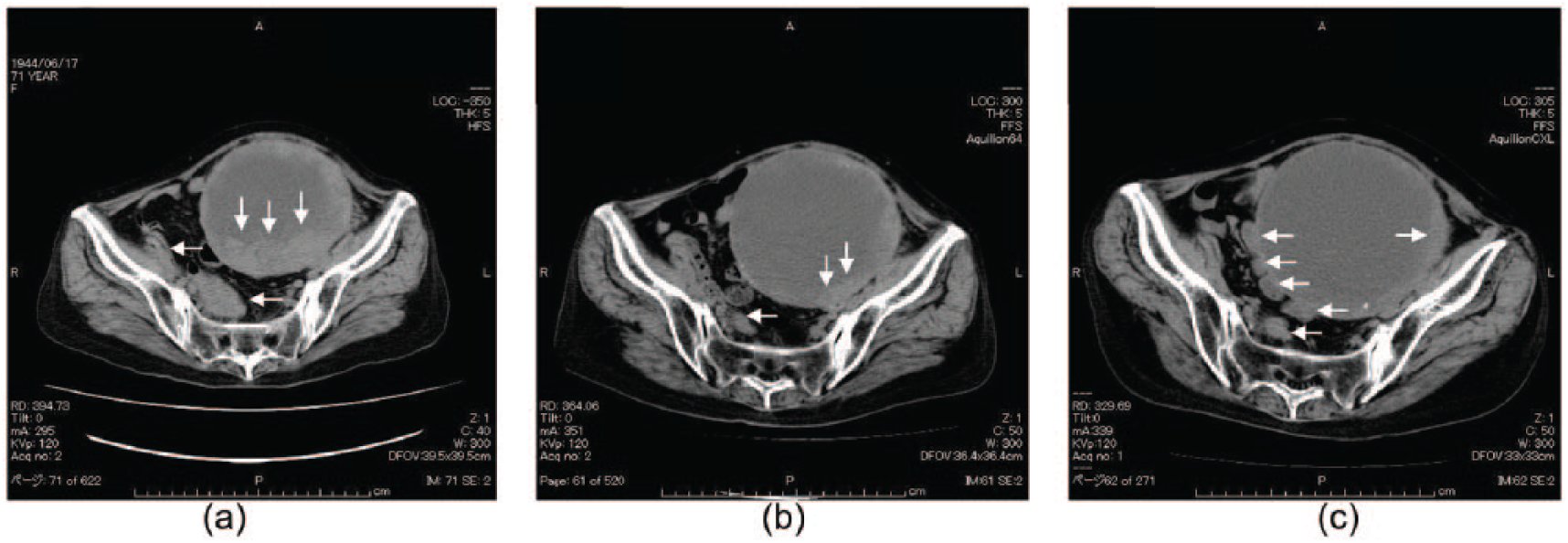
Computed tomography findings in the former hospital. Multiple recurrent metastatic tumors (white arrows) are detected (a). The recurrent metastatic tumors (white arrows) are shrinking at the 12th month (b) and growing again at the 23rd month (c) after the chemotherapy. They are the same horizontal levels.

Changes of serum tumor marker levels (CA125 and CA19-9) during therapy: (a) the days of discontinuation and (b) restart of the therapy.
Discussion
The present report provides us with an exceptionally informative case of response to daily oral administration of half-dose etoposide in a woman with refractory recurrent endometrial adenocarcinoma. This therapy has tolerable stomach effects without bone marrow suppression and is economical (US$7/25 mg capsule/day). She was able to spend wonderful days in her home and visited our outpatient hospital once a month. It is well known that combination chemotherapy with paclitaxel and carboplatin is the first-choice therapy with good clinical evidence for recurrent endometrial adenocarcinoma. When we have exhausted all known useful drugs for patients with tumor refractory to the above drugs, we attempt some daring methods or recommend palliative therapy. Etoposide is a DNA topoisomerase II inhibitor, and some positive outcomes have been described in reports of cases with refractory recurrent endometrial adenocarcinoma.1,2 Although the present patient was a rare case, the results of the previous phase II study were still considered debatable.4,5 Predictive biomarkers that are able to discriminate responders from non-responders to oral etoposide therapy are needed. It is well known that tumor cells are released from the recurrent sites into the blood stream; therefore, analysis of the circulating tumor cells may be a step toward personalized medicine. Moreover, the analysis of circulating cell-free tumor DNA can further complement data from tumor cell analysis.6,7 These recent studies highlight possible indications for patients that may respond to oral etoposide therapy for recurrent endometrial adenocarcinoma, as in the present case.
Conclusion
In conclusion, the treatment for repeatedly recurrent refractory tumor remains a challenge. Low-dose oral etoposide therapy can friendly improve the quality of life for some palliative patients with such an endometrial adenocarcinoma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.