
Abstract
Condyloma acuminata, also known as anogenital warts, represent a cutaneous infection caused by sexual transmission of the human papilloma virus. We present a case of overwhelming condyloma acuminata that was treated successfully without surgery using only topical imiquimod 3.75% cream. The patient, a 66-year-old female, was referred to Dermatology for large protruding verrucous plaques that covered the entire surface of her external vulva, perineum and perianal area. These lesions developed after being treated for genital warts with cantharidin. Four other cases treated with imiquimod were identified in the literature but either required surgery, higher doses or longer duration of treatment or involved pediatric populations. In patients who are not amenable to surgery, topical imiquimod may be a novel standalone or an adjunctive therapy for giant condyloma acuminata.
Keywords
Introduction
Condyloma acuminata, also known as anogenital warts, represent a cutaneous infection caused by sexual transmission of the human papilloma virus (HPV). 1 In 2008, 39.9 million women in the United States were infected with HPV.2,3 Certain subtypes, such as 6 and 11, are associated with warts, while other subtypes like 16 or 18 are prone to malignant transformation.4–6 Genital warts can eventually resolve without treatment in an immunocompetent host. 4 However, with persistent and recurrent infection, surgical procedures are often required.4,7,8 We present a case of overwhelming condyloma acuminata that was treated successfully using only topical imiquimod.
Case report
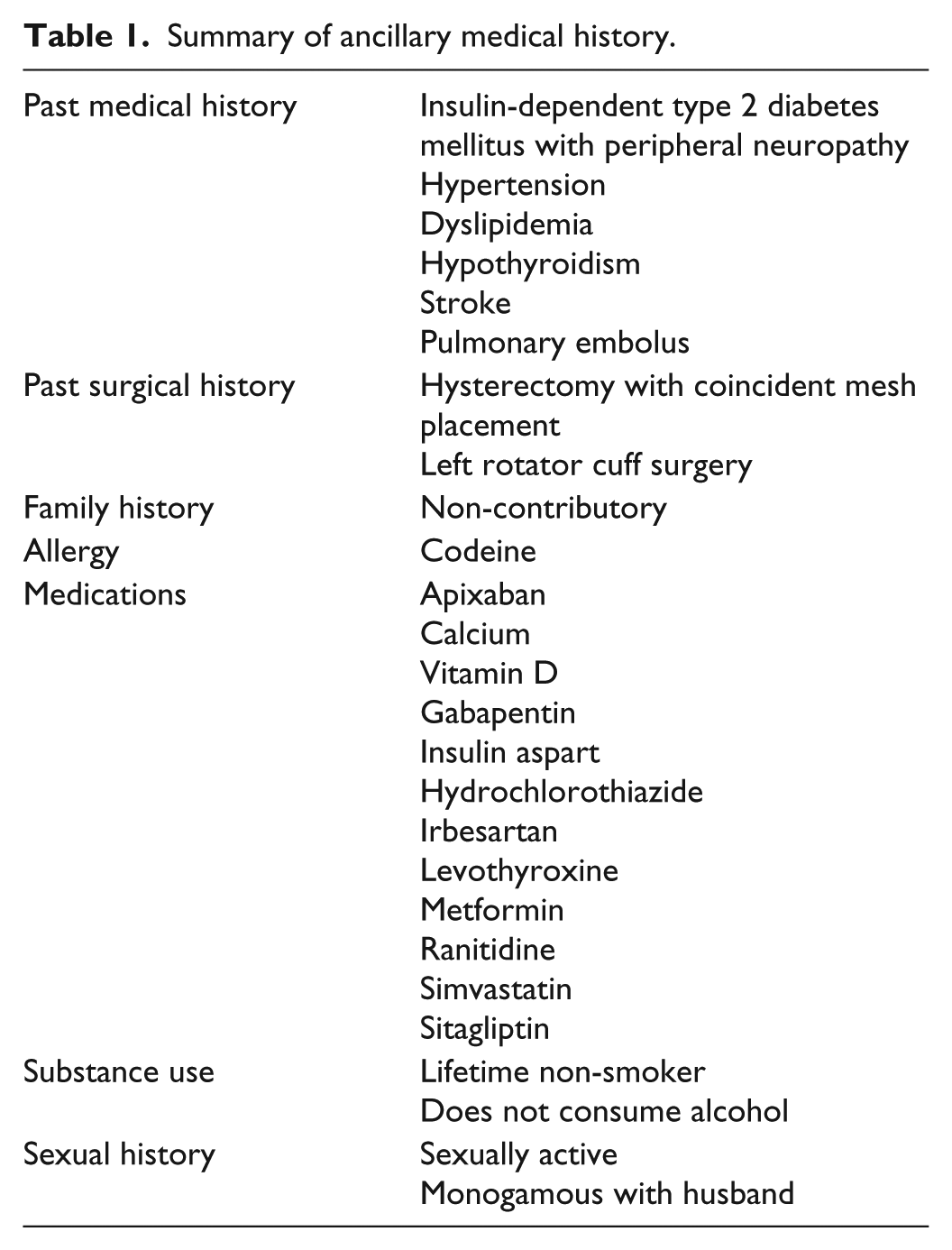
The patient, a 66-year-old female from El Salvador, was referred to Dermatology in December 2016 for large protruding verrucous plaques that covered the entire surface of her external vulva, perineum and perianal area. She also reported severe pain localized to the lesions which was refractory to both topical lidocaine and oxycodone. Relevant medical history is described in Table 1.
Summary of ancillary medical history.
She initially presented to primary care in November 2016 with small hard bumps on the vulva. Cryotherapy was applied initially and then cantharidin 0.7% solution at a subsequent office visit which the patient did not wash off. Afterwards, she presented to the emergency department with a severe bullous reaction and was advised to use topical polymyxin B/bacitracin. In the following weeks, while her skin was re-epithelizing, she developed large verrucous plaques and was referred to a Dermatologist.
On pelvic examination, there were large verrucous plaques involving bilateral labia majora and vulvae (Figure 1). The lesions were tender to palpation and covered the entire anterior apex and clitoris, extending 15 cm down each labium to the perineum and approaching the anal verge. The labia majora and minora were completely covered in warty tissue. The urethra and distal vagina did not have any involvement. Abdominal exam was benign and inguinal lymph nodes were not palpable.

Large verrucous plaques encompassing vulva, bilateral labia, and perineum.
A skin biopsy was done by the Dermatologist in January 2017 which showed benign wart tissue. She was then referred to the Vulvar Dermatology Clinic who instructed her to apply imiquimod 3.75% cream three times weekly and to hold if irritated. The patient, however, applied the cream daily for 1.5 months despite experiencing redness and skin breakdown, requiring topical lidocaine and oxycodone for pain relief.
She was also referred to Urology for urgent debulking; however, Urology felt that the patient was not appropriate for surgical excision as the warts were too overwhelming and would require skin grafting and support from plastic surgery. She was referred to Gynecology by the Urologist for a possible vulvectomy. For a summary timeline events, please see Figure 2.
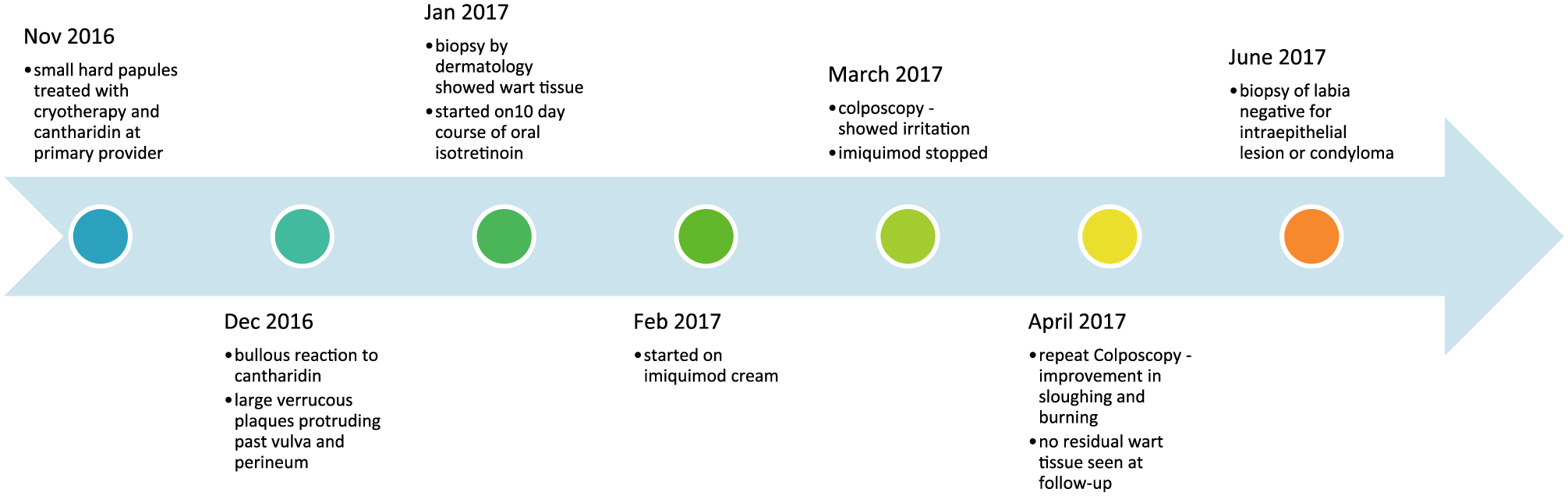
Timeline of events from first presentation of genital warts to full resolution.
After seeing Gynecology in March 2017, she was advised to discontinue imiquimod. A colposcopy at the time revealed only vulvar irritation. When seen in follow-up in early April 2017, the patient reported significant improvement in the size of lesions. The patient’s ongoing pain also decreased, requiring only acetaminophen for analgesia. On examination, there was no evidence of residual wart tissue with only post-inflammatory hyperpigmentation around the vulva and perineum (Figure 3). A repeat colposcopy in April 2017 showed no recurrent lesions with resolution of sloughing and burning.

Follow-up after 6 weeks of imiquimod treatment - no remaining lesions with intact genitalia.
Repeat biopsies were done by Gynecology in May 2017 to rule out vulvar intraepithelial neoplasia (VIN). The right labium and a new small erythematous nodule near the urethra were excised, both of which were found to be negative for intraepithelial lesion.
Discussion
Cantharidin, a vesicant produced by the blister beetle, is often used to treat warts.9,10 It is however reported as contraindicated in genital regions.10,11 This contraindication may be related to the propensity for increased blistering in mucosal surfaces. 12 In our case, the adverse reaction to cantharidin was so severe that narcotics were needed. Because of the potential for severe reactions, cantharidin requires significant caution when being administered. Physicians using cantharidin should ensure that patients have a clear understanding to remove cantharidin within 2–6 h or immediately if any adverse reactions occur. 11 In this case, a language barrier may have prevented proper understanding of post-treatment instructions.
Condyloma acuminata may progress to a form called giant condyloma acuminata, also known as a Buschke–Lowenstein tumor. Clinically, this variant is a slow-growing cauliflower-like growth that is locally invasive. 13 Although it is usually benign, up to one-third of the cases progress to malignancy.13,14 Because of the risk of malignancy, surgery is the first-line treatment for giant condyloma acuminate.13–15 On the other hand, topical agents such as imiquimod are highly effective in treating typical genital warts. A recent meta-analysis of studies comparing complete clearance of genital warts by imiquimod 3.75% cream to placebo (N = 601) found that there was a relative risk ratio of 2.88 favoring imiquimod 3.75%. 3 However, there is little information on whether imiquimod is effective against giant condyloma acuminata. We looked for other cases of giant condyloma acuminata that were treated with imiquimod. A search of PubMed in December 2017 turned up seven articles in which three cases were treated with a combination of imiquimod and surgical excision and one case was treated solely with imiquimod (Table 2).16–19
Cases of giant condyloma acuminata treated with topical imiquimod.

IFN: interferon.
In comparison to the other four cases, our case achieved clearance using lower potency and shorter treatment duration (Table 2). For Suarez-Ibarrola et al., imiquimod failed as an initial monotherapy. In the other two cases, imiquimod was used as an adjunct after surgery to treat the remaining warts. Finally, although Dinleyici et al. achieved complete clearance using only imiquimod, their patient was pediatric. Thus, our case has different implications, in that imiquimod has the potential to be used for monotherapy in adult patients. The benefit of using imiquimod over surgery alone is that imiquimod may help spare genital tissue by avoiding extensive surgery such as vulvectomy or reducing the amount of tissue that is needed to be excised.
A potential limitation to our case is that the giant condyloma acuminata progressed rapidly over weeks, while the other cases developed over years. We are unsure whether giant condyloma acuminata that arise in such a manner may be more responsive to immunomodulating therapies like imiquimod. Another limitation of this report is the lack of long-term follow-up. As giant condyloma acuminata are slow growing and recurrent, despite treatment with imiquimod, there may be subclinical remnants that recur. Finally, although imiquimod’s safety in treating genital warts is well established, these data may not be applicable to giant condyloma acuminate. 3 While our case demonstrates promising results, surgical excision remains the mainstay of treatment for giant condyloma acuminata until the safety and efficacy profile of imiquimod 3.75% cream can be verified for this off-label indication.
Footnotes
Declaration of conflicting interests
M.D. and E.C. have received honoraria for being a speaker and an advisor for Valeant. M.H. and S.N. have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Signed, written informed consent for patient information and images to be published was provided by the patient.