
Abstract
A 76-year-old Caucasian woman presented with a 3-year history of a recurrent pruritic eruption on the hips, thighs, and under the breasts associated with intermittent lesions resembling vesicles and bullae that failed to respond to topical corticosteroids. She had a history of severe lichen sclerosis et atrophicus, leading to invasive squamous cell carcinoma of the vulva for which she underwent radical vulvectomy and bilateral inguino-femoral lymph node dissection. On physical examination, involving the inframammary breasts, abdomen, hips, and proximal thighs there were multiple erosions with hemorrhagic crust and multiple clustered translucent papules. 4+ pitting and nonpitting edema were present on both legs. Biopsies were consistent with acquired lymphangiectasia. Acquired lymphangiectasia can be difficult to identify clinically. In our case, the unusually widespread distribution was morphologically reminiscent of immunobullous disease. The extensive surgical disruption to the patient’s lymphatic system was likely responsible for this unique presentation.
Introduction
Acquired lymphangiectasia (AL), also known as acquired lymphangioma circumscriptum, is a rare condition caused by lymphatic destruction resulting in superficial lymphatic dilatations. Reported causes include surgery, chronic infection, malignancy, and radiotherapy. Lymphedema is also a common association. Presentation of AL is dependent on the anatomical site and degree of lymphatic disruption.1,2 We report a case of AL after radical vulvectomy and inguinal lymphadenectomy with an abnormally widespread distribution and clinical features of immunobullous disease.
Case report
A 76-year-old Caucasian woman presented with a 3-year history of a recurrent pruritic eruption on the hips, thighs, and under the breasts associated with intermittent lesions resembling vesicles and bullae. Previous topical and intralesional corticosteroid therapy provided her with minimal relief. The patient was also experiencing swelling of the lower extremities. She had a history of long standing severe lichen sclerosis et atrophicus. Several months prior to the onset of the eruption, she was diagnosed with stage 2/grade 2 invasive squamous cell carcinoma of the vulva for which she underwent radical vulvectomy and bilateral inguino-femoral lymph node dissection.
On physical examination, involving the inframammary breasts, abdomen, hips, and proximal thighs, there were multiple erosions with hemorrhagic crust and multiple clustered translucent papules morphologically reminiscent of vesicles (Figures 1 and 2). 4+ pitting and nonpitting edema and scattered small vesicular lesions were present on both legs. Biopsies from representative lesions showed superficial dermal thin-walled dilated vascular channels surrounded by hyalinized collagen and scant perivascular lymphohistiocytic inflammation (Figures 3 and 4). The ectatic vessels showed endothelial cell staining with D2-40. Direct immunofluorescence of perilesional skin was negative. Given her clinical findings and surgical history, the diagnosis of AL was made.

Abdomen: multiple clustered translucent and hemorrhagic papules morphologically reminiscent of vesicles.

Thigh: multiple erosions with hemorrhagic crust and multiple clustered translucent papules.

4×. Superficial dermal thin-walled dilated vascular channels surrounded by hyalinized collagen.
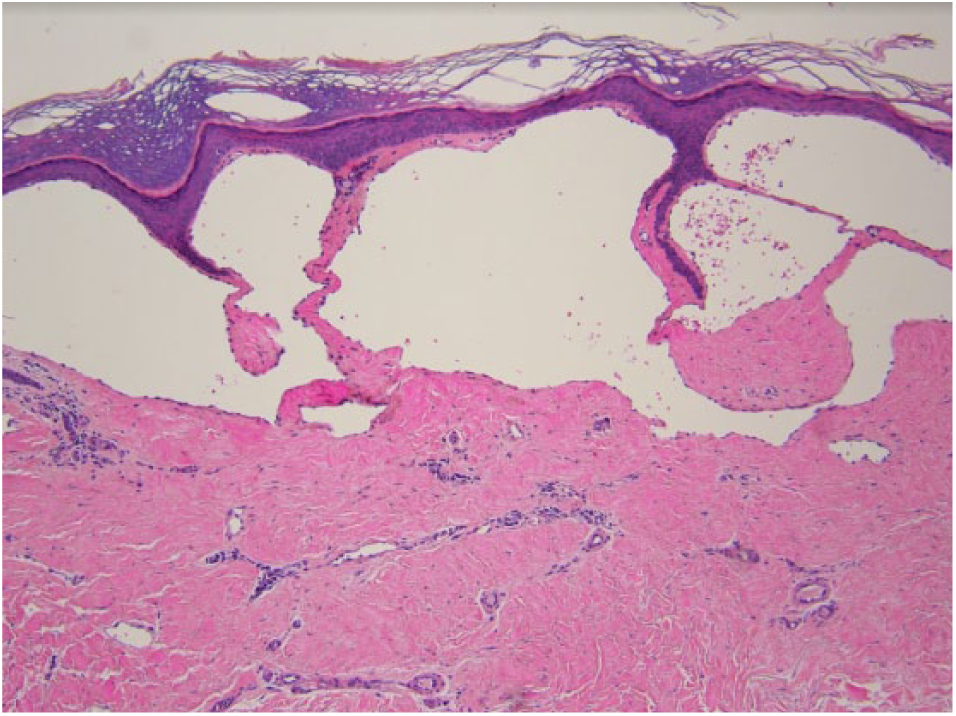
10×. Thin-walled, dilated vascular channels surrounded by hyalinized collagen and scant perivascular lymphohistiocytic inflammation.
Discussion
Typically, AL presents as clusters of small translucent papules (which represent superficial dermal location), containing fluid which ranges in color from clear to red, with a clustered appearance resembling the redundant bundles of eggs produced by some amphibians (“frog spawn”).1,2 Histopathologic findings show papillary to superficial reticular dermal ectatic and saccular vessels, sometimes containing pauci-cellular lymphatic material. Podoplanin (D2-40) is a frequently used immunohistochemistry stain specific for an O-linked sialoglycoprotein found on lymphatic endothelium (as in our patient). 1
Our case is noteworthy due to the unique distribution and symptomatology mimicking immune bullous disease, particularly the vesicular variant of bullous pemphigoid. This rare variant presents with multiple small tense vesicles with a symmetric distribution and typically affects patients in this age group. 3 The adjacent grouping of “vesicles” without confluence into bullae and hemorrhage within vesicles should allow the observant clinician to consider AL. Other reported clinical mimics of vulvar AL include bullous lichen sclerosis et atrophicus and infection with herpes simplex virus. 2
Vulvar carcinoma has an increasing risk of spread to regional lymph nodes with depth of invasion. There is a 26%–34% chance of spread to regional lymph nodes in tumors greater than 3 mm in depth (our patient had a depth of 6.2 mm). 4 Given the depth of invasion and its proximity to midline (less than 2 cm), radical vulvectomy with bilateral inguino-femoral lymphadenectomy was indicated. 4 The inguinal lymph nodes are responsible for the abdomen’s lymphatic drainage, from approximately the level of the umbilicus, extending inferiorly to the lower limbs. 1 Given the extensive surgical disruption of this drainage pathway, this is likely the reason for the widespread distribution, including portions of our patient’s trunk. Depending on the patient’s anatomy, this could include inframammary skin.
Treatment of AL is difficult and lesions often recur. Treatment for our patient has included use of electronic lymphedema pumps to the lower extremities for 1 hour twice daily. This has resulted in marked reduction of edema, skin erosions, and size/fragility of lymphangiectatic clusters. Her mobility and quality of life have substantially improved.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained for use of de-identified data and photos for publication.