
Abstract
It is a common medical practice to anticoagulate an asymptomatic left ventricular mural thrombus following an ST-elevation myocardial infarction using a vitamin K antagonist. Novel oral anticoagulants have not been studied extensively in this context, and therefore, no recommendations have been made for their use. A 67-year-old male physician with no significant medical history presented to the cardiology clinic complaining of shortness of breath that had been gradually worsening over a 2-week period and was found to have an anterior wall myocardial infarction with apical left ventricular thrombus that was treated with apixaban. We present a case of rapid resolution of left ventricular thrombus with the use of apixaban for anticoagulation. Although there are no guideline recommendations for this use, there have been case series and case reports that have shown safety and efficacy. Apixaban can be used for rapid resolution of left ventricular thrombus treatment.
It is a common medical practice to anticoagulate an asymptomatic left ventricular (LV) mural thrombus following an ST-elevation myocardial infarction (STEMI) using a vitamin K antagonist (VKA). 1 Novel oral anticoagulants (NOACs) have not been studied extensively in this context, and therefore, no recommendations have been made for their use. Unfortunately, there have been no large, randomized trials to support or guide the use of anticoagulation to prevent thromboembolic events in patients with LV thrombi, and the data for VKAs are based on observational studies only. NOACs are currently approved for venous thromboembolism (VTE), nonvalvular atrial fibrillation, and postoperative VTE prophylaxis. 2 There have been several case reports commenting on the resolution of an LV thrombus with the use of NOACs, but these are reported in patients with hypertrophic and tachycardia-induced cardiomyopathies or in the setting of failed anticoagulation due to bleeding with warfarin. We describe a case report of a patient with a STEMI and an asymptomatic LV thrombus that resolved with the use of apixaban.
Case report
A 67-year-old male physician with no significant medical history presented to the cardiology clinic complaining of shortness of breath that had been gradually worsening over a 2-week period. His electrocardiogram (ECG) revealed evidence of poor R wave progression in the anteroseptal leads. He underwent a transthoracic echocardiogram (TTE) and was found to have a reduced LV ejection fraction of 35%–40% with anteroseptal and apical wall akinesis. He became dyspneic and required intubation and mechanical ventilation. Coronary angiography revealed 99% proximal left anterior descending artery (LAD) and 80%–90% mid-LAD stenosis. He received two drug-eluting stents to the LAD. He also received an intra-aortic balloon pump for hemodynamic support.
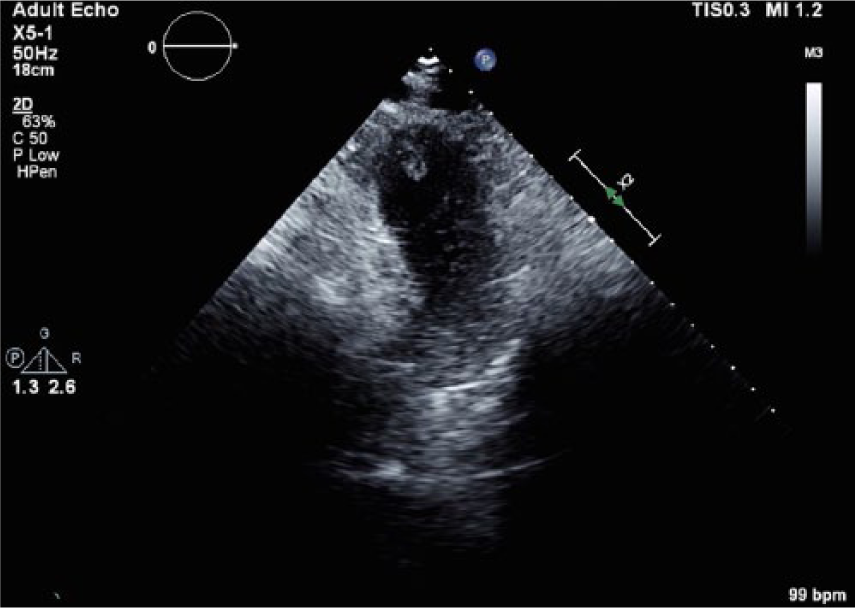
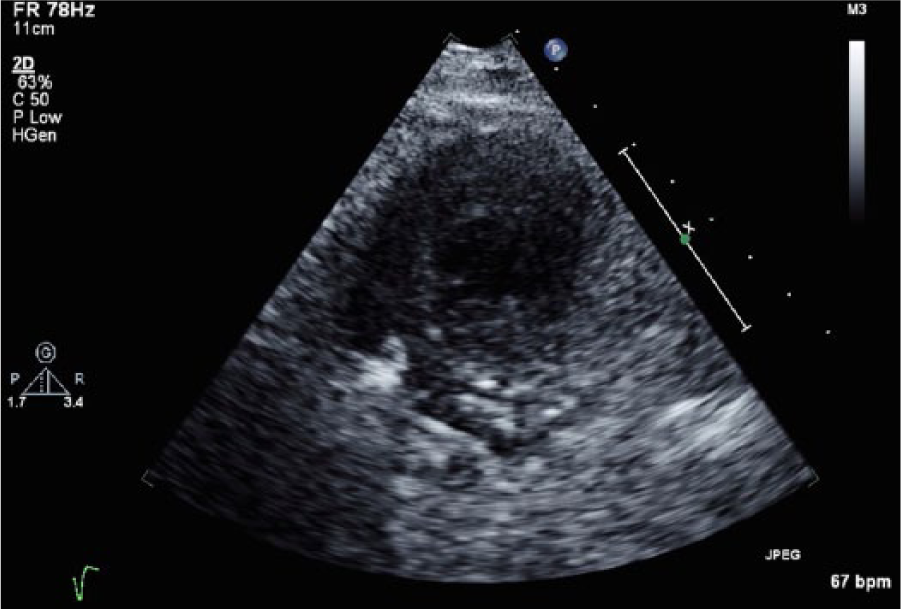
A follow-up TTE was ordered and revealed an LV thrombus (Figures 1 and 2). Initially, the patient was to begin warfarin for anticoagulation per STEMI anticoagulation guidelines. However, the patient preferred to attempt anticoagulation with an NOAC despite knowing the current guidelines, since he was a physician himself. Apixaban 5 mg twice daily was initiated with the intention to treat for 3 months. He was discharged home in stable condition.

B-mode short-axis view demonstrating left ventricular thrombus.
B-mode echocardiogram of left ventricular apex demonstrating left ventricular thrombus following anterior wall myocardial infarction.
He returned to the emergency department 1 week later for recurrent dyspnea. His workup revealed no acute findings. Repeat echocardiogram revealed resolution of the LV thrombus (Figures 3 and 4) and there were no clinical signs to indicate embolus. The decision was made to continue anticoagulation with apixaban for a total of 3 months as originally prescribed. The patient continued to do well, and at most recent follow-up, more than 12 months following the described clinical event, the patient is without embolic sequelae.
B-mode echocardiogram of left ventricular apex demonstrating resolution of left ventricular thrombus.

Color-flow Doppler of left ventricular apex demonstrating resolution of left ventricular thrombus.
Discussion
We present a case of rapid resolution of LV thrombus with the use of apixaban for anticoagulation. There are no randomized trials that evaluate the efficacy of oral anticoagulation to prevent LV thrombus embolization following a STEMI, and the current data available have been obtained from observational studies. 1 A recent retrospective study showed that the incidence of LV thrombus during STEMI involving approximately 2000 patients was noted to be 1.5%. 3 This low prevalence of disease makes the possibility of randomized controlled trials to evaluate treatments unlikely because of the low enrollment numbers that would be expected. A meta-analysis of seven observational studies included patients with STEMI and LV thrombus who either did or did not receive anticoagulation, supported the hypotheses that the risk of embolization of mural thrombus after a myocardial infarction is reduced by systemic anticoagulation and anticoagulation can prevent mural thrombus formation. 1 These studies were completed prior to the era of NOACs. There is currently no data on the use of non-vitamin K oral anticoagulants for prevention of LV thrombus embolization. For this reason, they are not currently recommended for this indication.
There are several limitations to using VKA including the need for close monitoring to maintain a narrow therapeutic range, dietary restrictions, and multiple drug-to-drug interactions. These concerns are mitigated when an NOAC is substituted for a VKA. There are now several case reports that demonstrate similar findings to our case report with resolution of LV thrombus following an acute coronary syndrome with apixaban, rivaroxaban, and even dabigatran.4–6 There has also been case reports of LV thrombus secondary to tachycardia-induced and hypertrophic cardiomyopathies that have been successfully treated with NOACs.7,8 Our case report demonstrates rapid resolution of LV thrombus in less than 3 months, and this was also observed in several other cases.4,5,7,8 Moreover, only one other case revealed LV thrombus resolution in 1 week. 8 This implies that LV thrombus treatment with NOACs maybe of shorter duration than with VKAs if future data demonstrate consistency of these findings and NOACs are approved for this indication.
Conclusion
Recent studies have shown that NOACs are at least noninferior to warfarin for the prevention of embolization in nonvalvular atrial fibrillation and treatment of VTE.9,10 This case study exemplifies that apixaban and other NOACs maybe efficacious for the treatment of LV thrombus, and do so expeditiously, but further studies are necessary to help guide their use for this indication.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.