
Abstract
In thyroid cancer patients with renal impairment or other complicating factors, it is important to maximize I-131 therapy efficacy while minimizing bone marrow and lung damage. We developed a web-based calculator based on a modified Benua and Leeper method to calculate the maximum I-131 dose to reduce the risk of these toxicities, based on the effective renal clearance of I-123 as measured from two whole-body I-123 scans, performed at 0 and 24 h post-administration.
Introduction
Radioiodine-131 (I-131) therapy is an established and validated treatment option in specific groups of patients with well-differentiated thyroid cancer. The administered activity (“dosage”) of I-131 is usually determined empirically, based on clinical and diagnostic imaging.1,2 However, patient-specific dose calculations can become critical in situations such as moderate to severe renal impairment, bone marrow pathology, poor pulmonary function, and extensive pulmonary metastatic disease, where the usual empiric doses could potentially result in serious toxicities in the bone marrow and lungs. Several dosimetric methods have been employed and described in the literature.3–5
In the Benua method, first described in 1962, an upper limit to the I-131 therapy dosage is set, such that the radiation absorbed dose to the patient’s blood (taken to reflect that to bone marrow) will not exceed 2 Gy. 6 In this method, blood and urine samples were obtained over regular intervals following administration of a diagnostic dosage of I-131 and analyzed for radioactivity content. The serial blood activity measurements were plotted versus time, and the area under the time-activity curve, along with patient weight, was used to calculate the maximum dosage to avoid bone marrow toxicity. It was subsequently determined that dosages for which the I-131 retention at 48 h was less than 4.44 GBq (120 mCi) were unlikely to result in serious hematological complications. 5 In addition, retention less than 3.0 GBq (80 mCi) was unlikely to result in pulmonary toxicity. Variations on this method based on simpler blood sampling protocols have been proposed. 7
Case discussion
To ensure that the total body retention of I-131 would not exceed the 48-h retention targets for marrow or lung toxicity in patients with impaired renal function, we developed a “modified Benua and Leeper” approach based on the retention of a diagnostic dose of iodine-123 (I-123) at 24 h following administration. Like the original Benua and Leeper method, our protocol is empirical in nature and compares an estimate of the total-body retained I-131 activity to the marrow and pulmonary tolerance activities (4.44 and 3.0 GBq, respectively). In our protocol, the patient first receives 74 MBq (2 mCi) I-123 sodium iodide by mouth. Anterior and posterior images of the whole body are obtained beginning 0.5–2 h following administration (“time zero”). The scans include an I-123 “standard” source in the field-of-view for purposes of correcting for scanner sensitivity variations between scans. It is crucial that these digitally acquired “time zero” images are taken before the patient has urinated—usually within 2 h after I-123 ingestion, so that the imaging data represent the initial total body radioiodine content.
Whole-body anterior and posterior images are then repeated at about 24 h “Day 1,” shortly after the patient has voided. Regions of interest (ROIs) in the images that include the whole body and the I-123 standard source are manually defined, and the geometric means of the anterior and posterior ROI counts are calculated for the “time zero” and “Day 1” images. The acquisition times and the geometric means for the whole-body and the I-123 standard source for both the “time zero” and “Day 1” images are entered into web-based analysis software. After correction for scanner sensitivity variation, the software extracts the whole-body biological clearance rate from the I-123 image data by correcting for the physical decay of I-123 (half-life 13.2 h). The software then calculates the projected whole-body activity of I-131 (half-life 8.02 days) at 48 h, based on the assumption that the biological clearance can be described by a single exponential function. This projected I-131 total body activity is then compared to the maximum I-131 dosage consistent with the 48-h retention targets for marrow or pulmonary toxicity (4.44 and 3.0 GBq, respectively).
This protocol was employed in a 48-year-old man with T4 N1 M1 papillary thyroid cancer and innumerable pulmonary metastases (see Figure 1). His primary tumor was 5 cm in size and exhibited vascular invasion and perithyroidal extension on histopathology. Our web-based software (see Figure 2) calculated his biological clearance half-life to be 18.8 h and I-131 clearance effective half-life to be 17.1 h (“Normal” Duke reference value is 18 h). This corresponded to a maximum administered activity of 30.9 GBq (836 mCi) and 20.6 GBq (557 mCi) to avoid severe marrow depression and severe pulmonary complications, respectively. These results confirmed that we would be able to treat the patient with our typical empiric single-treatment dosage of 7.4 GBq (200 mCi) for distant metastatic disease without concern for marrow or pulmonary complications.

Patient is a 48-year-old male with node-positive papillary thyroid carcinoma with adverse pathologic features and evidence for distant metastases s/p thyroidectomy. (a) Initial total body I-123 scan of the patient on “Day 1” obtained 1 h after I-123 but prior to voiding. A low-activity “standard” source (50–100 µCi) of I-123 is placed near the patient’s ankle to correct for changes in scanner speed and sensitivity between the two scans. Separate regions of interest (ROIs) are drawn around the whole body and “standard” on both anterior and posterior views (not shown). (b) Total body I-123 scan of patient on “Day 2” at 24 h. ROIs are drawn around the total body and “standard” (not shown) and integral ROI counts are used to compute total body burden and “standard” content. (c) CT shows innumerable pulmonary nodules. Although not radioiodine-avid, they were FDG-avid on positron emission tomography and wedge resection confirmed metastatic disease.
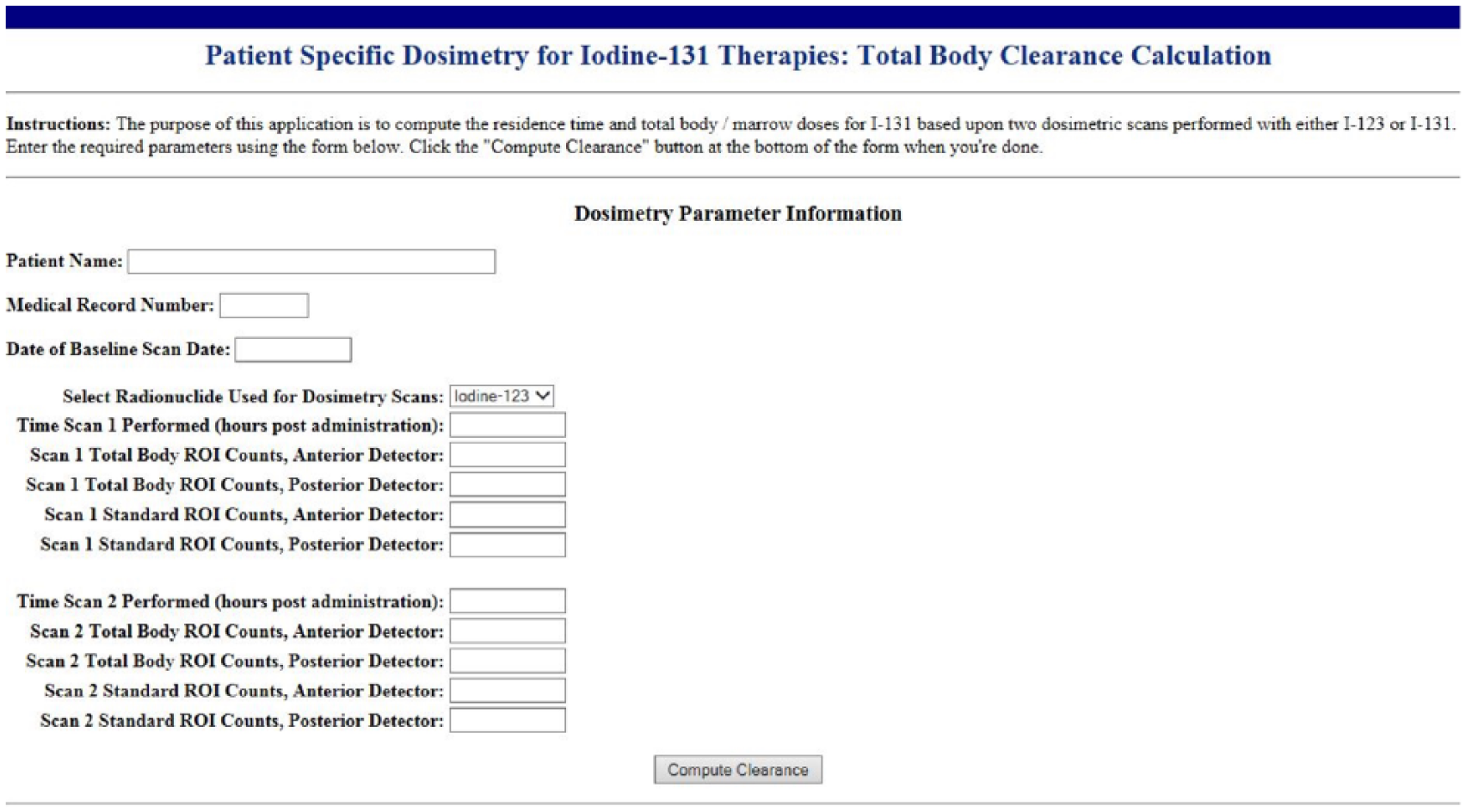
Data entry form of the web-based calculator that computes the effective clearance half-time for I-131 using data from two total body iodine scans. Provision is made using a standard source to correct for variations in scanner sensitivity. The I-131 effective clearance half-time is used to estimate the maximum administered activities to avoid marrow and pulmonary toxicity.
We also employed this protocol in a 39-year-old woman with Stage IV chronic kidney disease on the renal transplant list with serum creatinine of 5.7 mg/dL, a pT1b N1a MX papillary thyroid cancer with a 1.3 cm primary tumor, micrometastasis in a perithyroidal lymph node, and no clinical evidence of distant metastasis. An estimate of radioiodine clearance was requested due to the increased risk of toxicity in the setting of chronic renal failure. Using our approach, 1.85 GBq (50 mCi) of I-131 was determined to be the maximal safe dosage for this patient.
Conclusion
In summary, we have developed a web-based calculator based on a “modified Benua and Leeper” methodology, which enabled us to treat two patients with an appropriate activity of I-131 while ensuring that bone marrow and pulmonary toxicities would be avoided. This method requires estimation of the effective renal clearance of I-123 as measured from two whole-body I-123 scans, performed at 2 and 24 h post-administration, and uses that information to calculate the projected I-131 retention at 48 h for comparison to marrow and pulmonary toxicity targets.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institutional review board does not require ethical approval for reporting individual cases or case series of three or fewer patients.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent (as per Committee on Publication Ethics guidelines) was obtained from the first of two of the patients in this manuscript for their anonymized information to be published in this article. Written informed consent was also obtained from the legally authorized representative of the second of the two patients reported in this manuscript, who is deceased.