
Abstract
Background:
Music has been found to improve sleep and reduce anxiety.
Purpose:
This article reports a 78-year-old Chinese female who had been diagnosed with early dementia underwent an 8-week music-with-movement intervention delivered by her husband at home after being trained in a day care center.
Methods:
Both the patient and the husband’s data were collected through repeated interviews and regular observations.
Conclusion:
The results indicated signs of improvement of the patient in terms of sleep quality and depressive symptoms.
Keywords
Introduction
People with early dementia (PWeD) can experience stress, anxiety, poor sleep quality, and poor quality of life.1,2 Music interventions have been found to be effective in improving sleep and reducing anxiety, facilitate non-verbal expression, and communication between the facilitator and PWeD.3,4 In addition, music intervention allows PWeDs to express themselves and create a sense of mental–physical relaxation through refocusing one’s attention on a more pleasant emotional state. 5 The music-with-movement (MWM) intervention is an intervention that is deemed particularly suitable for PWeD. 6 The content of the MWM protocol was written in Chinese and validated by experts from different health disciplines. 7 MWM is an active interventional approach which involves gross body muscle movement using participants’ preferred music, where verbal ability and fine muscle coordination are not required. It can cater to elderly people who dislike singing. It is suitable for PWeD, as their verbal skills decline in a relatively early stage, whereas their gross motor abilities are better preserved.8,9
Case study
This report describes the effects of MWM on a Chinese female with early dementia. She underwent an 8-week home-based program delivered by her husband. The aim of the intervention was to reduce anxiety and promote sleep.
The patient, aged 78 years, was born and educated in Hong Kong. After completing her university education, the mother of three became a teacher. She retired at the age of 60 years. Presently, she lives with her husband and a domestic helper. She had a stroke in 2011, resulting in left hemiparalysis. Later that year, she was diagnosed as suffering from early dementia. At the time of recruitment (September 2014), she has a score of 1 (mild dementia) with Clinical Dementia Rating scale. She suffers from memory loss and deteriorating verbal communication. Her functional performance improved somewhat after continuous physiotherapy but she still fully relies on her domestic helper for bathing and transferring. She also required some assistance in toileting and dressing, but was capable of feeding herself. Her Modified Barthel Index score when she joined our study was 35/100, suggesting that she was severely dependent on others for her activities of daily living.
Her mini-mental state examination (MMSE) score at baseline (12 November 2014) was 19/30 (the cut-off score for someone with her educational background is 25). Her Geriatric Depression Scale (GDS) score was 15/15 but with no suicidal ideation, and her Rating Anxiety in Dementia (RAID) score was 36/60 (a score higher than 11 indicates possible clinical anxiety). Her sleep quality was poor (Pittsburgh Sleep Quality Index (PSQI) = 18/25). The patient has regular appointments with a psychiatrist every 6 months for reported depression and anxiety 2 years ago. Due to her high GDS and RAID scores found during our study, she was referred to the social worker of her social center by the research team. As for her neuropsychiatric condition, she scored 8/36 in the Neuropsychiatric Inventory Questionnaire (NPI-Q), which was relatively low.
The patient’s music experience
The patient was recruited from a social center to join a randomized controlled trial on MWM intervention (ClinicalTrials.gov ID: NCT01976832). She was randomly assigned to the intervention group. According to her husband Mr L, neither the patient nor her family had much experience with music and was not interested in singing. However, the patient attends church every weekend, where hymns were played and sung. Furthermore, she told the research staff that she enjoys listening to Cantonese opera and music of her time.
The MWM intervention
The MWM protocol is an 8-week home-based intervention program, which was developed by a registered music therapist in Hong Kong to fit PWeD. The intervention protocol has been published, and it includes complex movements of motor imitation activities, playing with instruments, and exercising with music. 7 The intervention requires the primary caregiver to facilitate the delivery of a 30-min MWM at home for at least three times per week. Prior to the commencement of the intervention, the caregiver underwent a weekly 2-h training session for 5 weeks given by a registered music therapist and/or a trained research staff, about how basic music intervention techniques and how to deliver the intervention.
Data were collected before, immediately after, and 8 weeks after the intervention. During the intervention period, the center staffs and research assistant (RA) made either a weekly phone call or home visit to monitor and encourage the continual delivery of the intervention. At such times, the information about intervention intensity and frequency delivered by the family caregiver were also collected from the families, who were responsible for recording their intervention schedule. During the visits, the RA observed the manner in which the family delivered the intervention and offered remedial instructions and/or further training if needed. The caregiver was interviewed by the RA using a semi-structured questionnaire upon the completion of the intervention.
Treatment processes
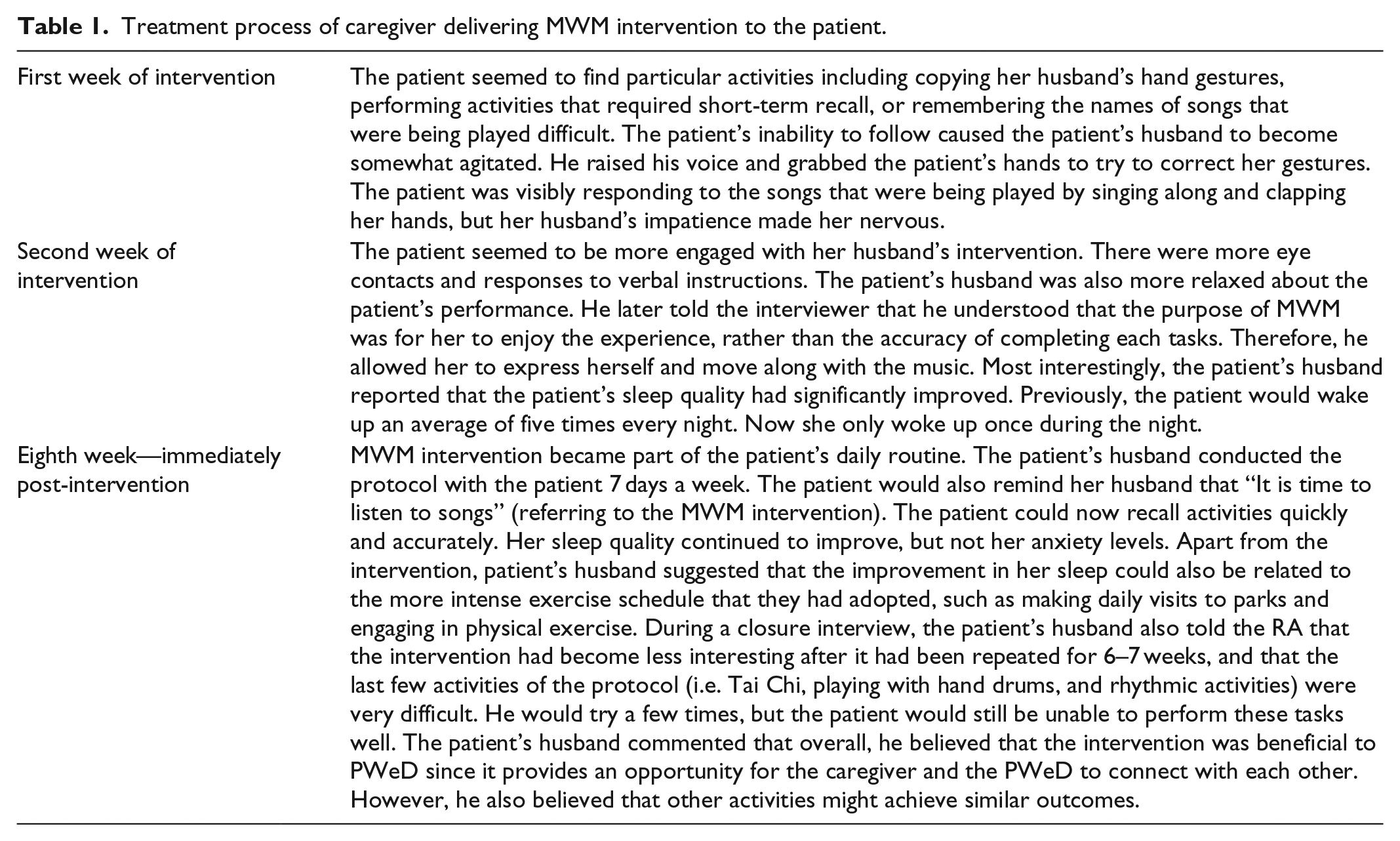
Through observation and interviews conducted by the RA during home visits, how the MWM intervention was delivered at home was recorded (Table 1).
Treatment process of caregiver delivering MWM intervention to the patient.
Results
The patient had an average of four sessions of intervention per week, each session lasted an average of 60.5 min. Table 2 shows no clear changes in the patient’s MMSE score; however, there was a decrease in her GDS and PSQI scores. Interestingly, patient’s RAID score increased during the intervention period. At the post-intervention follow-up assessment in the eighth week, the patient’s husband indicated that they had decreased their MWM intervention to just once a week for 15 min. The PSQI score increased again.
Participant’s performance at baseline, immediately post-intervention, and 8 weeks post-intervention.

MMSE: mini-mental state examination; GDS: Geriatric Depression Scale; RAID: Rating Anxiety in Dementia; PSQI: Pittsburgh Sleep Quality Index; NPI-Q: Neuropsychiatric Inventory Questionnaire.
Discussion
The results in this case are different from those of previous reports on music intervention, which often indicated a reduction in anxiety. 10 One possible explanation for this is the interventionist effect, which therapist himself or herself could be a factor affecting the outcome of the intervention. 11 One of the aims of MWM was to foster a sense of success and competency in PWeD. 12 Mr L, however, focused on the patient’s ability to accurately follow the activity protocol, which was not the spirit of the intervention. Eventually, he came to understand the purpose of the intervention and the process became more enjoyable. Consequently, the patient willingly accepted the MWM protocol as part of their daily activities. However, the patient’s husband still followed the steps of the protocol closely and lacked the flexibility to adapt the intervention to the needs of the patient. In the future, more intense training will be needed if a caregiver-delivered intervention is to be successful.
RA’s observations during site visits showed that the patient’s short-term (free and cued recall) and long-term memory had improved. She was able to recognize songs and the names of the singers. She was also capable of carrying out some of the routines of the MWM activities (without being prompted). However, her MMSE score did not reflect such improvements. Because MMSE assesses a person’s global cognitive status, improvements in a specific cognitive domain may not be clearly captured. Although the patient’s GDS score had slightly improved, she was still within the score range of possible depression. In terms of sleep quality, the patient showed clear improvement. In the follow-up assessment in the eighth week, however, the data indicated that the effect was not sustained.
One other confounder that could have affected the outcomes was the patient’s stepped-up physical activity program. Other investigations will be needed to identify whether the MWM or other intervening variables led to sleep improvement. With regard to the benefits of MWM, an obvious change was seen after the intervention. The patient changed from being uninterested in singing to exhibiting clear enjoyment of the MWM activity and making MWM her daily routine.
Conclusion
The results showed that the MWM intervention might improve sleep quality. Unlike individualized music therapy, MWM does not require a music therapist, although the interventionist must be well trained. The MWM intervention is therefore more cost-effective and easily accessible. With a home-based intervention, PWeD can enjoy music activities delivered by trained family members. An individualized protocol can also be designed to fit particular PWeD. However, in order for PWeD to benefit from MWM, more vigorous training is needed for caregivers to grasp the “spirit” of what MWM is trying to achieve. Carrying out MWM without understanding its purpose would reduce the effectiveness of the intervention, or even lead to higher anxiety levels in the PWeD.
Footnotes
Acknowledgements
The project team gratefully acknowledges the support of the participating NGOs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from The Hong Kong Polytechnic University Research Committee (Approval ID: HSEARS20130831001).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Ho Chung Shuk Yuen Charitable Foundation (PolyU #5ZH96).
Informed consent
The written informed consent of the patient was obtained from the patient’s primary caregiver (her husband) and the patient. Although the patient had a score of 1 in the Clinical Dementia Rating Scale (indicating mild dementia), she was aware what was going on around her and was capable of making her own decisions.