
Abstract
Coronary artery fistula is an uncommon congenital disease that requires invasive treatment for symptomatic patients. Although percutaneous intervention has become the popular treatment option, surgical treatment is preferred for severely tortuous coronary artery fistulas. We report a case of an extremely tortuous coronary artery fistula successfully treated with the support of the GuideLiner catheter and the mother-grandchild technique.
Introduction
Congenital coronary artery fistula (CAF) is an uncommon anomaly, connecting to the pulmonary artery, cardiac chamber, coronary sinus, or pulmonary vein.1,2 The observed incidence of CAF varies from 0.06% to 0.2%. 3 Although asymptomatic patients with small fistulas may be left untreated, symptomatic patients with myocardial ischemia or heart failure should be considered for closure. 1 With the advancement of endovascular techniques and devices, percutaneous closure has become an attractive treatment option. CAFs possess diverse anatomical variations, and in cases with extremely tortuous fistulas, care must be taken to avoid distal embolization of the coils, which is a serious complication.4,5 In this report, we demonstrate how the GuideLiner catheter provided extra support to deliver the microcatheter to the distal portion, enabling a safe procedure.
Case report
A 58-year-old man was referred to our hospital with a 3-month history of chest pain on exertion (Canadian Cardiovascular Society Class 3). The patient was normal on physical examination. Transthoracic echocardiography showed normal left ventricular systolic function. An electrocardiogram was interpreted as within normal limits. His cardiac biomarkers were normal including a creatine kinase of 108 U/L, troponin T of 0.005 ng/mL, and BNP of 13.8 pg/mL.
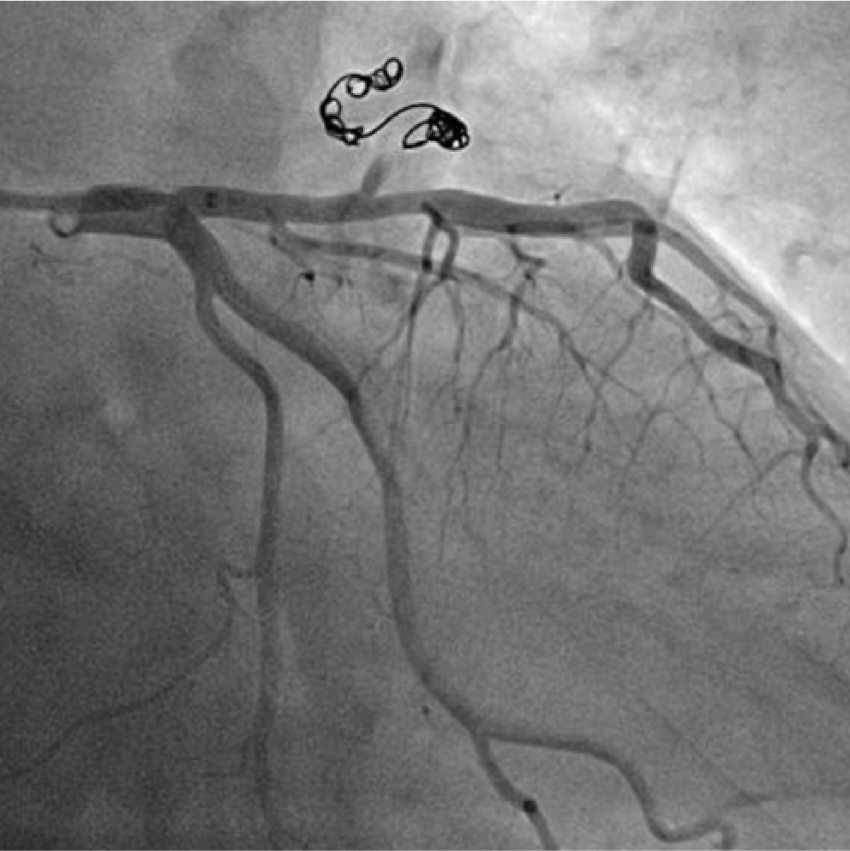
Diagnostic coronary angiography revealed a severely tortuous coronary artery to pulmonary artery fistula originating from the proximal part of the left anterior descending artery (LAD; Figure 1). There was no significant stenosis, but there was moderate stenosis in the distal part of the LAD.

Coronary angiography depicting the severely tortuous coronary artery fistula originating from the proximal left anterior descending artery.
We planned to perform closure of the coronary artery fistula because the radionuclide stress test showed evidence of ischemia in the LAD lesion, presumably caused by the coronary steal resulting from the coronary artery fistula. Multi-detector computed tomography was also performed to observe the anatomy of the LAD and the coronary fistula (Figure 2).

Multi-detected computed tomography demonstrating the coronary artery fistula.
A 6-Fr Special Support (SS) guiding catheter (Profit, Goodman, Nagoya, Japan) was inserted into the left coronary artery via the right radial artery. A 0.014-inch SION blue coronary guidewire (Asahi Intecc, Nagoya, Japan) easily crossed to the distal portion of the fistula. However, when we tried to deliver the 2.5-Fr Renegade™-18 microcatheter (Boston Scientific, Natick, MA, USA), it could not pass the first bend (Figure 3(a); Supplementary Movie 1). We concluded that we needed more support and decided to use the 5.5-Fr GuideLiner catheter as an inner catheter. The GuideLiner catheter was advanced to the entry point of the fistula. This “Mother-child-grandchild” technique provided enough support to introduce the Renegade microcatheter into the distally dilated portion of the fistula over the wire (Figure 3(b); Supplementary Movie 2). With the secured system, we initially delivered a 2-mm Interlock™ coil into the dilated part of the fistula, followed by two 2-mm Interlock™ coils (Figure 3(c); Supplementary Movie 3). These coils occluded our initial targeted coronary fistula, but coronary angiography revealed another fistula arising from the proximal portion. Thus, we placed another 6-mm Interlock™ coil at the ostium of the fistula. The final angiogram revealed the complete obliteration of the CAF, resulting in improved flow to the distal portion of the LAD (Figure 4; Supplementary Movie 4).

Fluoroscopy during the coil implantation: (a) the 2.5-Fr Renegade™-18 microcatheter (Boston Scientific, Natick, MA, USA) could not pass the first bend without the support of the GuildeLiner; (b) when the GuideLiner catheter (lined arrow) was advanced to the entry point of the fistula, the Renegade microcatheter (dotted arrow) easily reached the distally dilated portion of the fistula; and (c) 2-mm Interlock™ coil being delivered to the dilated part of the fistula with the support of the GuildeLiner.
Final coronary angiography. It shows complete obliteration of the coronary artery fistula.
Supplementary Movies 1–4 demonstrate moving image of Figure 3(a)–(c), Figure 4, respectively.
The administration of aspirin was discontinued after the procedure to induce thrombus in the coiled fistula. The patient was discharged the following day without complications. Examination of the blood the day after the procedure revealed cardiac biomarkers within normal limits; creatine kinase of 107 U/L and troponin T of 0.012 ng/mL. The patient remained symptom-free at the 2-month follow-up and there was no significant change on his electrocardiogram.
Discussion
No consensus has been established regarding the optimal treatment for CAF, owing to its low prevalence. Although percutaneous intervention is an ideal choice for CAF, 6 past reports have recommended surgical treatment for extremely tortuous fistulas.1,4,6 After evaluating the angiogram of this patient, we considered surgery a safe option because of the severe tortuousness of the fistula and explained this to the patient. However, the patient opted to be treated by the percutaneous approach, as it is less invasive than surgery.
We planned to perform a safe and reliable percutaneous strategy. Occlusion of the LAD was to be avoided; thus, we took measures to minimize the risk of distal embolization. Care was also taken regarding the manipulation of the microcatheter and coils. Although a microcatheter such as Renegade™ does provide some support, it could prolapse during procedures involving tortuous lesions. In this case, the GuideLiner played a pivotal role in the procedure to lend extra support and safety to the system. The GuideLiner, which is quite often used in complex percutaneous coronary intervention procedures, has a rapid exchange system with a 25-cm soft and flexible tube connected to a stainless-steel rod. 7 It provides strong support to the guiding catheter, when deeply inserted into the coronary artery using the “Mother and child” technique. Consequently, it allows the delivery of devices in patients with heavy calcification or severe tortuousness. 8 We preferred to use the GuideLiner instead of the conventional catheter utilized for the “Mother and child” technique to treat the CAF 9 because the GuideLiner is easier to handle with a rapid exchange system that does not require a second hemostat valve. 8 As the 2.5-Fr Renegade™ microcatheter was advanced through the inner 5.5-Fr GuideLiner catheter, which was inserted into the 6-Fr guiding catheter, the “Mother-child-grandchild” technique proposed by Ashikaga et al. 10 may describe our case more precisely. Stent-assisted coil embolization, which was recently proposed by Fede et al., 11 could have been another option for our case. However, we wanted to avoid placing a stent in the healthy LAD because this could have provoked stent thrombosis in the future. Larger devices such as the Amplatzer occluder 9 would have been unnecessarily large for our case, with a moderate-sized CAF. To conform to the concept of minimally invasive treatment, we choose the transradial intervention, which is reportedly safer than the conventional transfemoral approach. 12
There are some potential risks that the operator must consider when using the GuideLiner catheter. First, there is a risk of coronary injury, especially in cases associated with proximal atherosclerotic lesions.13,14 Second, there is a risk of air embolism and distal thromboembolism. 15 Operators must consistently check for air and thrombus in the guiding catheter after the insertion and removal of the GuideLiner catheter.
Conclusion
In conclusion, we introduced a safe and practical percutaneous strategy to treat a severely tortuous CAF using the GuideLiner catheter. Special attention is required when manipulating the GuideLiner catheter to minimize the risk of its specific complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this case report involving human participants were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for publication of this case report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.