
Abstract
Radiation and tumor infiltration confer a high risk of bleeding on surgical removal of tumor. We report on the case of a 42-year-old woman with a recurrent occult subclavian tumor in her right breast. Computed tomography revealed enhanced tumor adhesion to the subclavian artery at the infraclavicular lymph node. No other metastases were detected. We pre-operatively performed stenting of the right subclavian artery, and the tumor was resected completely and safely.
Keywords
Histopathological examination of the resected specimen revealed that the tumor was an adenocarcinoma, which was the same as the patient’s initial tumor. The cancer had invaded the adventitia of the subclavian artery, but not the media and intima of the artery. We considered the tumor to be completely resected. Placement of a stent into the tumor-infiltrating artery before surgery aided in the complete and safe removal of the tumor.
Radiation can induce degeneration of the fibroelastic intima and media of arteries, and tumor infiltration can also change the properties of an artery.1,2 These factors confer a high risk of bleeding on surgical removal of a tumor that has adhered to an artery. We were faced with this prospect in a patient with tumor invasion of the subclavian artery and came up with the idea of placing a stent in that artery before tumor resection. To our knowledge, there are no prior examples in the literature of a stent being used for this purpose.
Case
In 2014, a 42-year-old woman was referred to our hospital for complete resection of a right subclavian tumor. She had originally undergone right axillary, subclavian, and Rotter’s lymph node resection for right occult breast cancer in 2009. After resection, she was administered chemotherapy and actinotherapy. In 2011, she returned with recurrence of a tumor in her right subclavian area. At that time, surgical removal of the tumor was attempted but abandoned because the tumor had tightly adhered to the subclavian artery. However, she did have a complete response to chemotherapy and actinotherapy. The tumor shrank in size, and she was considered to be in a state of complete tumor response (CR).
When she was referred to us, computerized tomography revealed a poorly marginated and enhanced tumor that had occluded the subclavian vein and adhered to the subclavian artery at the infraclavicular lymph node (Figure 1). Various other examinations determined that she did not have any other metastases. The patient was relatively young and desired to have the tumor removed. We made the decision to perform a complete resection of the tumor together with the sections of the subclavian vein and artery involved. Based on the imaging results, we expected that it would be difficult to control bleeding and to prevent subclavian arterial decortication during the tumorectomy. One of our surgical team suggested that we performed subclavian artery stenting prior to tumor resection to minimize bleeding risk, and we attempted this.

Pre-operative computed tomographic images showing the poorly marginated and enhanced tumor that had occluded the subclavian vein and adhered to the subclavian artery at the infraclavicular lymph node (arrow).
After obtaining informed consent from the patient and approval from the Hospital Ethics Committee, we decided to place stents (Niti-S ComVi stent 8 mm × 8 cm; Taewoong Medical, Seoul, Korea) in the subclavian artery. We placed two stents so that their overlap reached the middle of the tumor, and the landing length was 3 cm from the right brachiocephalic artery.
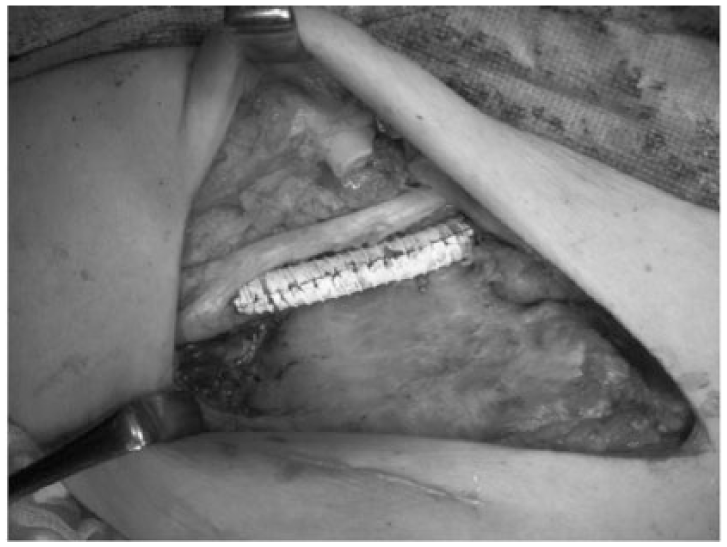
Surgery was performed 1 week after stent placement. We removed the right clavicle to allow access to the tumor. We identified and controlled bleeding from the right subclavian artery and the axillary artery, which came from a small incision in the axillary artery. We removed the tumor with the arterial wall including intima, and we were able to detect the placed stent. Surgical bleeding was not observed (Figure 2). To prevent the stent from moving and causing bleeding, we wrapped the entire length of the stent with an artificial blood vessel (8 mm Advanta™ VXT with ring; Atrium Medical Corporation, Ethicon, USA) and fixed the artificial vessel to the proximal and distal sides of the native artery with a running suture with 6-0 prolene (Figure 3). We excised the subclavian vein, which strongly adhered to the tumor, en bloc. The tumor was 21 mm × 13 mm, and pathological analysis showed that it was an adenocarcinoma, which was the same as the patient’s previous tumor. Therefore, the tumor was diagnosed as metastatic adenocarcinoma. We did not detect malignancy in the resected subclavian vein. Cancer had invaded the adventitia of the subclavian artery, but the media and intima of the artery were not invaded.

Intra-operative findings and removal of the adventitia of the subclavian artery. (a) After resection of the tumor and collarbone, the right subclavian artery and axillary artery (arrow) were controlled so that bleeding was not observed. (b) The subclavian and axillary arterial walls including intima were opened. Bleeding was not observed. (c) The arterial wall including intima was completely resected.
The entire length of the stent was wrapped with an artificial blood vessel (8 mm Advanta™ VXT with ring; Atrium Medical Corporation, USA) to prevent stent migration and bleeding.
We considered the tumor to be completely resected. The postoperative course was good, and postoperative neurological impairment was not observed. The patient received an oral antiplatelet drug after surgery.
Our institution does not require ethics approval for reporting individual cases. Our institution does not require informed consent to be obtained for reporting individual cases.
Discussion
In this case, tumor infiltration and adhesion to the artery and the fact that the area was in the radiation field were problems that complicated tumor resection. Radiation can induce degeneration of the fibroelastic intima and media of the artery, and tumor infiltration can change the properties of an artery.1,2 These factors make the surgical removal of a tumor that has adhered to an artery difficult, owing to a high risk of bleeding.
During complete resection of the tumor, we performed reconstruction using artificial blood vessels to allow removal of the artery. It has been reported that it is desirable to create a bypass between the vessels not exposed to radiation, and a bypass graft can be passed through the non-irradiated field. 3 In the present case, rebuilding the vessel with a synthetic graft would have made the operation more invasive. Before surgery, we placed a stent in the vessel that the tumor may have invaded in order to decrease bleeding and allow complete and safe resection of the tumor.
Because the diameter of the proximal vessel where the stent was placed was about 6 mm, and access through the brachial artery was only 3 mm, we were not able to use the leg stent approach that is used to treat abdominal aortic aneurysms. Of the covered stents that can be used in Japan, all are used as bile duct stents except the GraftMaster (Abbott Vascular Devices, Abbott Park, IL, USA), which is used during coronary artery rupture.
We selected the Niti-S because this stent is much thinner and quite flexible. There was no edge, and the coating material was expanded polytetrafluoroethylene (ePTFE). Cejna reported that stents coated with ePTFE were less likely to become stenotic compared with stents coated with polyester. Stents coated in polyester led to 50% stenosis, the nominal diameter for neointimal formation, in experiments using sheep. 4 Dolmatch et al. 5 also reported similar findings. We decided that Niti-S coated with ePTFE, which is widely used as an artificial blood vessel, was the best material.
For the actual removal of the tumor, the nutrient vessel going into the tumor was occluded by the stent placed in the subclavian artery in an attempt to reduce bleeding at the time of the synechiotomy. An endovascular stent before surgery made it possible to completely prevent bleeding, and we were able to remove the whole layer of the subclavian artery without bleeding. Based on the pathological examination, we determined that the tumor was completely resected.
Migration of the stent during the surgical procedure was a concern, but placing a longer stent prevented this. To prevent future migration and to reinforce the stent, we wrapped the stent in a synthetic graft.
In a recurrent tumor that adhered to and invaded an artery and that was also inside the irradiation field, placement of a stent in the tumor-infiltrated artery prior to surgery was extremely helpful for safe and complete tumor removal.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for profit sectors.