
Abstract
Objective:
Although breast self-examination has been shown to be the least-expensive, less time-consuming, and non-invasive screening method, still there is a gap in practice. Furthermore, the information among more risky population which attends anti-retroviral therapy is too limited. Therefore, the aim of this study is to assess breast self-examination practices and its associated factors among women who attended the anti-retroviral therapy clinic in Bahir Dar city administration, Northwest Ethiopia.
Methods:
An institution-based cross-sectional study was conducted among 660 women who attended anti-retroviral therapy clinics from March 1 to March 30, 2020. A systematic random sampling technique was used to select study participants. Pre-tested interviewer-administered questionnaires were used to collect data. Data were entered in to EPI data 3.1 and exported to Statistical Package for the Social Sciences version 23.00 software for analysis. A binary logistic regression model was fitted to identify factors associated with self-breast examination. Variables with a p value less than 0.2 in bivariable regression were candidates for multivariable regression. Adjusted odds ratios with a 95% confidence intervals and p values less than 0.05 were used to determine the association between independent and dependent variables. Hosmer–Lemeshow Test was used to determine model fitness.
Result:
Among 641 study participants, 224 (34.9%) have ever practiced breast self-examination. Women who attended college or above (adjusted odds ratio = 4.04, 95% confidence interval (1.65,9.90)), rich (adjusted odds ratio = 6.64, 95% confidence interval (2.72,16.20)), knowledgeable about signs and symptoms of breast cancer (adjusted odds ratio = 5.13, 95% confidence interval ( 2.55,10.31)), risk factors for breast cancer (adjusted odds ratio = 3.62, 95% confidence interval (1.85,7.07)), positive attitude toward breast self-examination (adjusted odds ratio = 2.76,95% confidence interval (1.41,11.84)), family history of breast cancer (adjusted odds ratio = 3.68,95% confidence interval (1.14,11.84)), and knowledge about breast self-examination technique (adjusted odds ratio = 2.64, 95% confidence interval (1.23,5.66)) had higher odds of breast self-examination practice.
Conclusion:
The practice of breast self-examination was low. During their regular visits for other issues, education and information dissemination about the benefits and techniques of self-breast examination is recommended.
Introduction
Breast cancer is the most prevalent type of non-AIDS-defining cancer (NADC) among human immune deficiency virus (HIV)-positive women.1–3 Historically, AIDS-defining cancers (ADCs), especially Kaposi sarcoma (KS) and non-Hodgkin lymphoma (NHL) accounted for a substantial proportion of the morbidity and mortality in HIV-infected individuals; with the use of anti-retroviral therapy (ART), the incidence of these malignancies has decreased. 4 However, there has been an increase in NADCs from 1.6/1000 persons-years in 1999–2000 to 2.1 in 2009–2011. 5
According to the American cancer society, breast cancer screening methods are breast self-examination (BSE), clinical breast examination (CBE), and mammography, so far, these are usually done in combination. 6 Among these methods, mammography is the only one that has been proven to be effective, but the method is only cost-effective and feasible in countries with good health infrastructure. 7
The American Cancer Society recommends the use of BSE as a tool for breast cancer screening, stating that palpable lesions can be detected through BSE and is a more important recommended method in developing countries including Ethiopia because it is easy, convenient, private, and safe that does not require specific equipment. 8
The concept of BSE was promoted in the 1950s by Cushman Haagensen, a breast surgeon from the United States, at a time when mammography was yet to be developed and many women were diagnosed when the tumor had become large and inoperable. 9 Programs to support and encourage monthly BSE were first established in Europe, Australia, and North America in the 1950s and implemented until recently. 10
Breast cancer is one of the most commonly diagnosed cancers worldwide. It is briefly outlined that in 2022, an estimated 1.9 million new cancer cases diagnosed and 609,360 cancer deaths in the United States. 11 Although breast cancer is to be as a disease in developed countries, reports showed that the rate of breast cancer is to be 92.6 cases per 100,000 people in Western Europe, while it stands at 45.3 cases per 100,000 populations in Western Asian countries including Turkey. 12 Similarly, the incidence rate of breast cancer in women in Western Africa is 37.3 per 100,000 women. According to Global Cancer (GLOBCAN) report in 2018, the number of new cases of breast cancer in Ethiopia was 15,244 (32.9%). 13
HIV is a major burden in sub-Saharan Africa (SSA), with up to 70% of global cases being reported in this region. 14 A review from South Africa, showed that HIV-positive patients have an increased risk of developing breast cancer as well as increased mortality and morbidity from the disease. 15 Thirty per 100,000 women in SSA with breast cancer have associated HIV comorbidity. 16 A study suggested that beyond the “classic” risk factors of breast cancer additionally, HIV-related risk factors such as immunodeficiency, chronic persistence of viral infections associated with HIV as well as a metabolic disorder related to ART drug was a predominant factor for breast cancer disease. 16
Screening tests are effective therapeutic and preventive strategies needed to reduce cancer burden especially among people living with HIV . It is highly likely that early diagnosis remains an important early detection strategy, particularly in low- and middle-income countries where breast cancer is diagnosed in the late-stage, and resources are scarce as in Ethiopia. 17 The American Cancer Society recommends that women starting from the age of 20 years should undergo monthly BSE. 8
The World Health Organization (WHO) promotes breast cancer control within the context of comprehensive national cancer control programs integrated into non-communicable diseases and other related problems. 18 Another key point is that the sustainable development goal (SDG), goal-3 target states that maternal health can be improved by reducing the global maternal mortality ratio below 70 per 100,000 live births by 2030. For the purpose of this, numerous interventions have been designed and implemented by different nations to achieve the SDG target. 19
The Ethiopian Federal Ministry of health (FMOH) recommends breast cancer self-examination as a means of empowering women’s health. 20 In 2015, the Ethiopian healthcare authorities developed a cancer control plan that focuses on prevention as well as the general improvement of cancer care in the country. 21 Despite this effort, the incidence of breast cancer is growing and it is the most common among reproductive age-group women in Ethiopia. 22
Although BSE is the least-expensive, less time-consuming, and non-invasive screening method, studies conducted in Ethiopia showed that the practice of BSE is poor. 22 Previous studies reported that a skill gap in the techniques of performing BSE, not having a history of breast-related problems or symptoms, lack of knowledge about signs and symptoms of breast cancer, fear of being diagnosed with breast cancer and lack of advice from health extension workers were associated with BSE.23–25 Previous studies mainly focus on all women, but this study specifically focus on ART women who are more exposed for breast cancer, as well as to the best of our knowledge, there is a dearth of information on the practice and associated factors of BSE among women who attend ART clinic in Bahir Dar city administration. Therefore, the aim of this study was to assess BSE practices and associated factors among women attending ART clinics in Bahir Dar City, 2020.
Methods
Study design and period
An institution-based cross-sectional study was conducted in Bahir Dar city administration, Norwest Ethiopia from March 1 to March 1, 2020.
Population
The source population was all women who attended ART clinics in Bahir Dar city administration, whereas the study population was all women who attended ART in the selected ART clinic of the city administration. All women who received ART at a selected ART site and whose age was greater than or equal to 18 years were included while women who were severely ill, unable to communicate, and had already undergone breast surgery were excluded from this study.
Sample size determination and sampling procedure
The sample size was determined using a single population proportion formula considering the following assumptions: 95% confidence level, 5% margin of error, the proportion of BSE (26.6%) from a study conducted in Dire Dawa, 26 two design effects, and 10% of non-response rate.

Considering a 10% non-response rate, the final sample size was 660.
In Bahir Dar city administration, both private and public health institutions (five hospitals, one NGO clinic, and nine health centers) deliver ART services. Two hospitals (Felege Hiwot Referral Hospital and Gamby General Hospital) and two health centers (Bahir Dar health center and Han health center) were selected for this study by a lottery method. Based on 2019/2020 6-month client flow of each selected health institution, the average monthly client population has been determined (Felege Hiwot Referral Hospital 3140, Gamby General Hospital 198, Bahir Dar health center 802, Han health center 738). Then from selected health institution 660 samples were determined using proportional allocation to sample size (PAS). Women were selected for interview after they had finished their follow-up visit using a systematic sampling technique.
Variables of the study
Dependent variable: Practice of BSE (yes/no)
Independent variables Socio-demographic variables: age, residence, occupation, marital status, educational status of the women, educational and occupational status of husbands, household income, mass media, social media, knowledge of risk factors, signs and symptoms of breast cancer and on self-breast examination, history of breast problem: family history of breast cancer and personal breast problem and attitudes toward BSE.
Measurement and definition
Regular practice of BSE: women who practice BSE monthly within 7–10 days after menses using at least one of the following techniques: inspection, palpation, or squeezing. 27
There were about 15 knowledge-related questions, and each question scored 0 and 1 (0 = No, 1 = Yes). We took those participants who answered less than mean points out of the 15 questions as have poor knowledge, whereas those who answered a mean point and above the mean point as having a good knowledge on BSE. There were also about 35 attitude-related questions, and each question scored 0 and 1 (0 = No, 1 = Yes). We took those participants who answered less than mean points out of the 35 questions as have an unfavorable attitude, whereas those who answered a mean point and above the mean point as having a favorable attitude. 27
Data collection tools and procedures
A structured interviewer-administered questionnaire was used to collect information from study participants. The tool was adapted from Ethiopian EDHS 2016 and from other literatures.26,27 The questionnaire was prepared in English language and then translated to local language (Amharic) and then back translated to English by a third person to check consistency. The tool included the following sections; socio-demographic characteristics, household assets of the participant, knowledge on breast cancer and self-breast examination, attitude and practice on BSE. Four diploma nurses for data collector and two bachelor degree nurses for supervisor were recruited.
Data quality control
The quality of data was assured by proper designing and pre-testing the questionnaires on 5% of the sample at non-selected ART clinic in Bahir Dar city administration. A 2-day training was provided on the purpose of the study, data collection techniques, and on how to approach participants during interview period. The supervisors and the principal investigator reviewed each collected question on the daily basis to check for completeness.
Statistical analysis
The collected data were entered and cleaned using Epi data version 3.1, then exported to SPSS version 23 for analysis. A descriptive analysis was conducted to summarize the data, and the final results of the study were interpreted in the form of text, figures, and tables. Binary logistic regression analysis was performed to determine to see the association between independent and dependent variables. All explanatory variables with p < 0.2 in bivariable logistic regression were entered into multivariable logistic regression analysis and significant associations were identified based on p < 0.05 and odds ratio with 95% confidence interval (CI) in multivariable logistic regression. The final model fitness was checked using Hosmer–Lemeshow Goodness of Fit test. Principal component analysis () was done to determine the wealth status of respondents by using “Kaiser’s rule.” 28
A PCA was performed to obtain a wealth index. In the first analysis, components with eigenvalues (variance) greater than 1 were extracted. According to “Kaiser’s rule,” only those components with eigenvalues a greater than 1 should be retained based on Kaiser’s rule the study decided to retain the first component because it had greater eigenvalue (variance) than other components. In the first component, the variables that had correlation and coefficients score of less than 0.3 was excluded in the second analysis. 29 Finally, two components with eigenvalues greater than one were extracted. Based on the same rule “Kaiser’s rule,” the first component was retained because it had a greater eigenvalue than the second component and this first component was the one used to determine the participant’s wealth index score with ref no: BDU/IRB/9821/2020.
Ethical consideration
Ethical clearance was obtained from IRB of Bahir Dar University, College of Medicine and Health Sciences with ref no: BDU/IRB/9821/2020. Further approval was also granted from Bahir Dar city health office and respective health facilities. Informed written consent was obtained from each study participants. All information collected from participants was kept strictly confidential and names of patients did not include in the checklist. To keep confidentiality, all collected data were coded and entered into a computer with personal password.
Results
Socio-demographic characteristics of women and their husbands
Among the total of 660 women, 641 participated in the study with a response rate of 97.1%. The participants were from 18 to 56 years old with a mean age of 32.04 (SD ± 6.44). The highest proportion of women (54.3%) was in the age group of 29–38 years. Almost all women (95.6%) lived in urban areas. Regarding educational status of women, 141 (22%) participants had attended college or above. Regarding the educational status of their husbands, 145 (35.2%) had attended college or higher (Table 1).
Socio-demographic characteristics of women who attended ART clinic in Bahir Dar city administration 2020 (n = 641).

Daily labor, merchant, housewife, student, and farmer.
Knowledge and source of information about breast cancer and self-breast examination
A total of 214 (33.4%) women had heard about self-breast examination and 430 women had heard about breast cancer. Regarding the source of information, 172 (59.5%) women reported that the main source of information for BSE was health professionals. One hundred seventy-six (27.5%) women were informed that the recommended frequency of self-breast examinations was monthly. One hundred seventy-seven (27.6%) women understood about self-breast examination techniques. Concerning maternal knowledge of breast cancer, almost two-thirds of the women 411 (64.1%) were aware of its signs and symptoms, and 395 (61.6%) of them knew the risk factors of breast cancer (Figure 1).

Information sources of self-breast examination among women who attended ART clinic in Bahir Dar City administration, 2020.
Attitude and history of breast problem–related characteristics
Accordingly, over half of (52.7%) participants had a positive attitude toward BSE. Regarding history of breast problem, 48 (4.68%) women had a history of breast problems. Whereas, 71 (11.1%) of women reported a family history of breast cancer. Regarding kinship, 20 (28.1%) participants were their mothers, 20 (28.1%) were sisters, 18 (25.4%) were aunts, and 13 (18.3%) were grandmothers.
BSE practice
In this study, 224 (34.9%) women ever practice self-breast examination. Of those 89 (13.9%) women reported that they performed BSE consistently on a monthly basis using any of the three techniques: inspection, palpation, and squeezing. The major reason for respondent women for BSE practice was health provider recommendation 120 (53.5%) followed by fear of developing breast cancer 40 (6.2%), from family history 25 (11.1%), for early detection and treatment 20 (8.9%), had previous breast problem 19 (8.4%). Of the women who were practiced BSE, 53 (23.6%) women found their breast changes during examination.
Reasons not to practice BSE
The main reason for women did not practice self-breast examination was did not know how to practice it which was 59.9% (Figure 2).
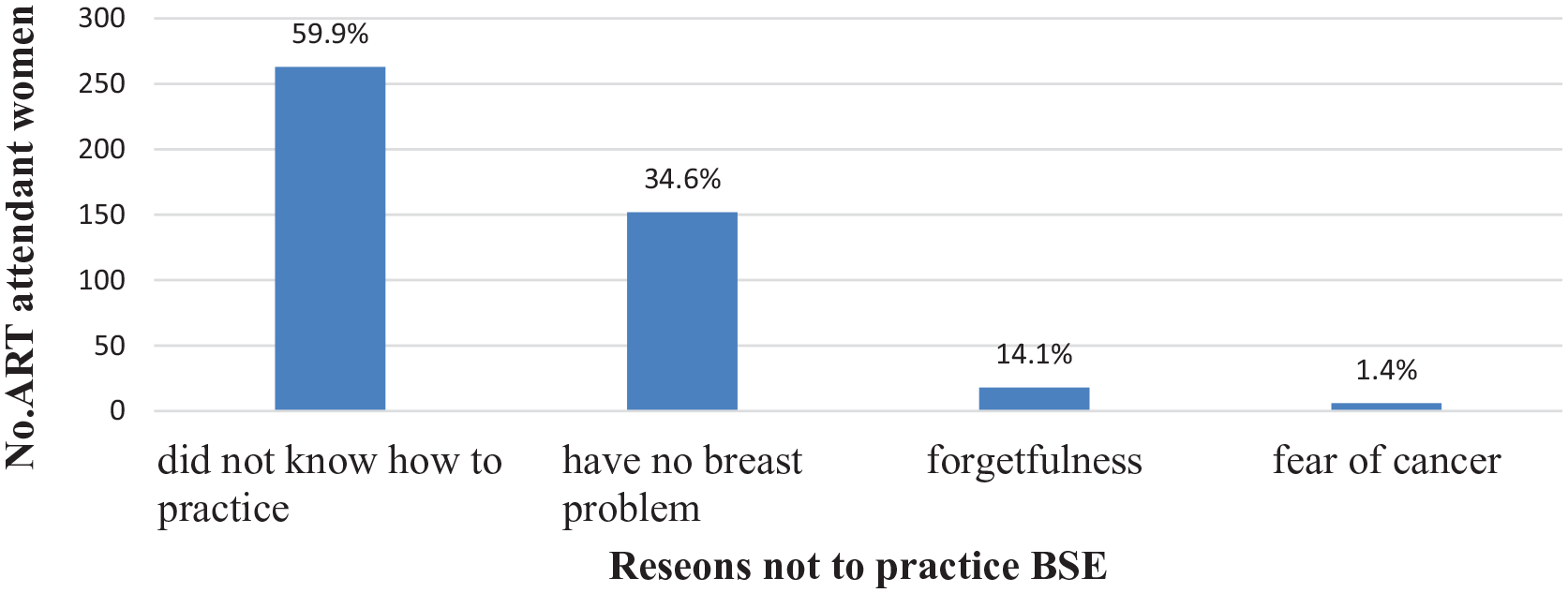
Reasons not to practice breast self-examination among women who attended ART clinic in Bahir Dar city administration, 2020.
Factors associated with BSE practice among ART attendant women
The odds of practicing BSE among women who attended college or above was 4.04 times (adjusted odds ratio (AOR) = 4.04, 95% CI (1.65–9.90)) compared to those who have attended other education levels. An employed women were 3.07 times (AOR = 3.07, 95% CI (1.49–6.33)) higher odds of practicing BSE as compared to unemployed ones. Women who had family history of breast cancer were 3.68 times (AOR = 3.68, 95% CI (1.14–11.8)) more likely to practice BSE than those who had not have family history of breast cancer.
Women who were knowledgeable on sign and symptom of breast cancer were 5.13 times (AOR = 5.13, 95% CI (2.55–10.31)) more likely to practice BSE than women who did not have any knowledge on sign and symptom. Women who were knowledgeable on risk factors of breast cancer were 3.62 times (AOR = 3.62, 95% CI (1.85–7.07)) more likely to practice BSE than who had no any knowledge on risk factors of breast cancer. It was also found that women who had knowledge on techniques of BSE were 2.64 times (AOR = 2.64, 95% CI (1.23–5.66)) more likely to practice BSE than those who had no knowledge on techniques of BSE practice.
Women who are rich in wealth index were 6.64 times (AOR = 6.64, 95% CI (2.72–16.2)) more efficiently practiced BSE than those who are not rich in wealth index. Women who had positive attitude toward self-breast examination were 2.76 times (AOR = 2.76, 95% CI (1.41–11.84)) more likely to practice BSE when compared with women who had negative attitude on BSE (Table 2).
Multivariable analysis and breast self-examination practice among women attending ART clinic in Bahr Dar city administration, 2020 (n = 641).
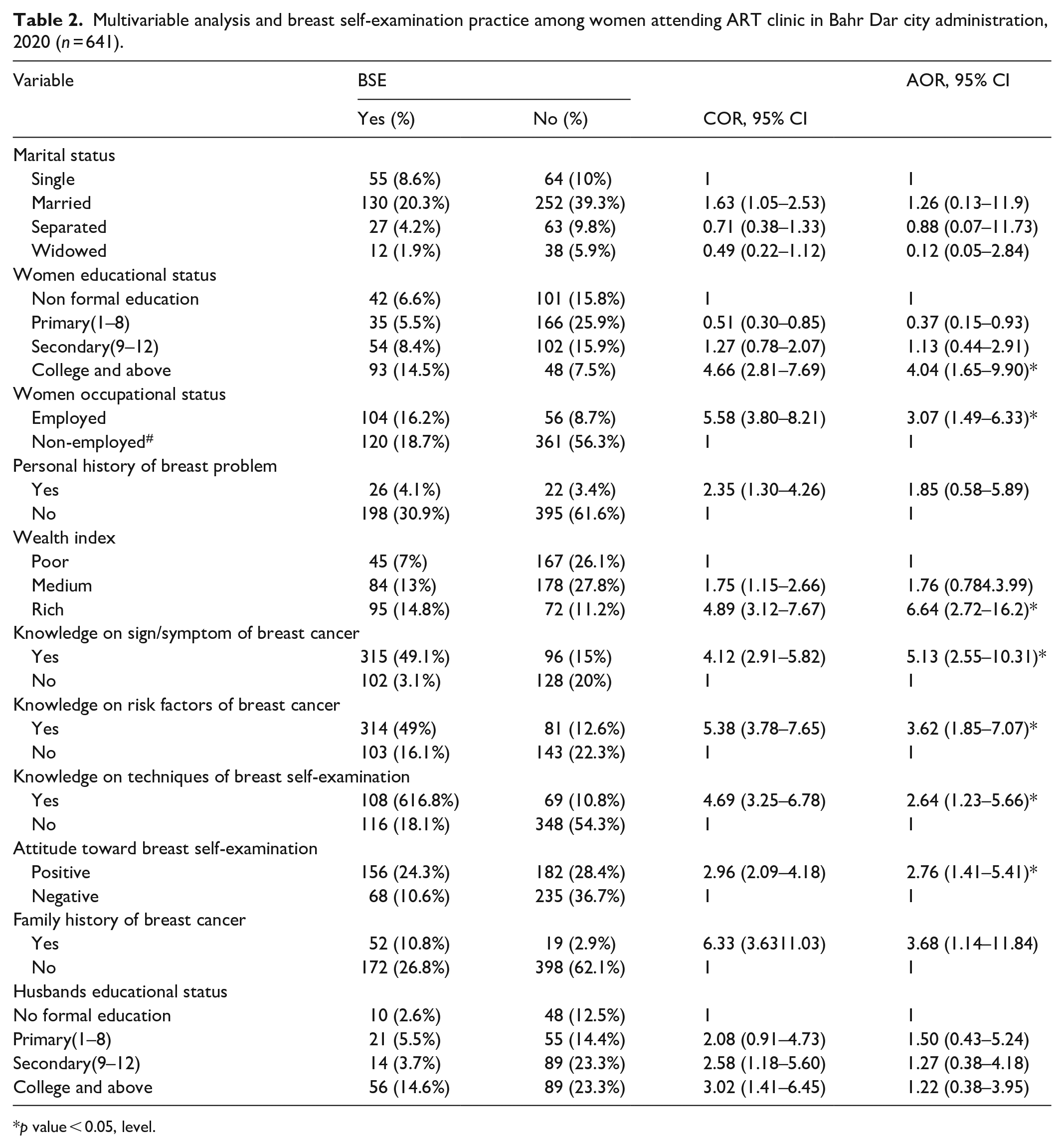
p value < 0.05, level.
Discussion
According to this study, the overall ever practice of BSE was 34.9% which was consistent with the study conducted in Debre tabor (32.5%). 27 However, the findings of this study was lower than study conducted in Gambella (42.9%). 29 This variation might be due to the difference in study population since a study conducted in Gambella study, participants were health workers who had better knowledge and awareness about breast cancer and BSE practice. Similarly, the current finding is lower than study conducted in Indonesia 44% 30 and Turkey 57.3%. 22 The difference might be due to study participants, knowledge, accessibility of information and study areas in considering of signs and symptoms of breast cancer and BSE practice.
Self-breast examination practice in this study was higher than study conducted in Kersa district 3.6% 31 and Zambia 28.2%. 32 This might be due to the reason that in this study most participants were urban in residence, literates, and had ART follow-up visits which had information access about breast cancer and BSE from health professionals through information dissemination and education programs.
This result revealed that women’s educational status was significantly associated with self-breast examination practice. Women who attended college or above education level had higher odds of BSE practice compared to those who attended secondary school or lesser. This finding was supported by study conducted in Adama and Adwa.33,34 Similar results were obtained with study conducted in Turkey, Saudi Arabia, Iran, Zambia, and Nigeria.22,32,35–37 This might be due to the reason that when educational status of women goes high, their awareness and information related to breast cancer and BSE increase, since this encourages a women to practice BSE.
Women who were employed had higher odds of self-breast examination as compared to women who were unemployed. This finding was supported by study conducted in Welayta Sodo, Mekelle and Adama.24,33,38 This might be due to when women employed, they had a capacity to access information about breast cancer and BSE. With this, they motivated to practice BSE.
Women who were knowledgeable on sign/symptom and risk factors of breast cancer had higher odds of self-breast examination practice compared to women who were not knowledgeable. Apart from this, women who had knowledge on methods of BSE techniques had also higher odds of BSE practice. This finding was supported by the studies conducted in Dire Dawa, Adwa, Addis Ababa, and Debre Tabor. 22 ,27,39,40 It was also similar to studies conducted in Pakistan and Thailand.6,12 This might be due to the fact that women’s knowledge of breast cancer and BSE practice encourage women to increase their understanding of the advantages of breast cancer screening and BSE.
Women who were rich in household wealth had higher odds of BSE practice. This finding was supported by study conducted in Addis Ababa 41 and Mexico. 42 It could be because rich women give attention for their health and having a potential to acquire knowledge regarding breast cancer and BSE screening techniques. And also they motivate to practice BSE to know any change regarding their breast.
This study revealed that the presence of family history of breast cancer was significantly associated with BSE. Women who had family history of breast cancer had higher odds of practicing BSE when compared to their counterparts. This was consistent with study conducted in Addis Ababa and Debre Tabor.22,27 This finding was also consistent with study conducted in Indonesia and Malaysia.29,41 This could be due to women who had a family history of breast cancer feeling at risk and becoming more sensitive to the issue than women who had no family history of breast cancer. This gave them a chance to search a piece of information and increases health-seeking behavior.
Attitude toward self-breast examination was significantly associated with self-breast examination practice. Women who have a positive attitude toward BSE had higher odds of practicing BSE compared to their counterparts. This result was consistent with studies conducted in Dire Dawa and Addis Ababa.24,22 This finding was also similar with studies conducted in Zambia and Bangladesh.32,42 This might be because women with a positive attitude toward BSE had a potential to acquire knowledge for early detection of a breast abnormality and in practicing BSE, as fact that attitude is a predisposing factor. Even though we used our maximum effort, this paper had limitations. Cross-sectional nature of this study limits to set causal effect relationship of independent and dependent variables. Since it was based on women’s report, it is difficult to get accurate information whether they practice BSE or not.
Conclusion
This study showed that the prevalence of self-breast examination practice is low in the study area. Lack of knowledge about breast cancer and how to practice self-breast examination is the main reason for low practice of self-breast examination. Women’s educational and occupational status, being rich, family history of breast cancer, knowledge on breast cancer and self-breast examination, and positive attitude toward BSE had statistically significant association with practice of self-breast examination.
Footnotes
Acknowledgements
The authors are sincerely grateful to the participants who voluntarily participated in the study. They are especially grateful to the Bahir Dar University and Bahir Dar health office as well as respective stakeholders for their support during the implementation of the study. They particularly acknowledge data collectors and supervisors for their contribution in the collection process.
Authors’ contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from * Ethical clearance was obtained from IRB of Bahir Dar University, College of Medicine and Health Sciences with Ref No: BDU/IRB/9821/2020. Following approval, A formal letter was given to the selected hospitals and health centers from the school of public health
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed written consent was obtained from all subjects before the study, and written informed consent was obtained from Amhara regional health office and from each health facilities’ representatives before the study. Informed written consent was obtained from all participants. Confidentiality was assured throughout the process. The names and addresses of the participants were not recorded in the questionnaire. Furthermore, all the basic principles of human research ethics (respect of persons, beneficence, voluntary participation, confidentiality, and justice) were respected.
Data availability
All related data have been presented within the manuscript. The data set supporting the conclusions of this article is available from the corresponding author upon reasonable request.