
Abstract
Background:
Acne vulgaris is a common inflammatory skin condition in adolescence and early adulthood. Although multiple factors contribute to acne, the role of diet remains debated. This study examined associations between acne and nutrition-related variables in young adults.
Methods:
We conducted an unmatched case–control study among adults aged 18–25 years in Hebron. Cases were recruited by convenience sampling from dermatology clinics, and controls were recruited voluntarily from the community (universities/social media). Data included sociodemographics, medical history, self-reported BMI, screening for eating-disorder risk (SCOFF), adherence to a Mediterranean diet, and an acne-related food frequency questionnaire. Although 200 cases and 100 controls were initially targeted, the final analyzed sample comprised 199 cases and 101 controls (N = 300) due to missing responses in key dietary questionnaire items required for analysis.
Results:
Compared with controls, cases had a higher proportion of females (76.9% versus 59.4%) and more non-normal BMI (36.7% versus 19.8%). In adjusted analysis, acne was associated with female sex in this clinic versus community sampling frame (aOR 2.66, 95% CI 1.50–4.72), overweight BMI (aOR 2.72, 95% CI 1.29–5.75), and intake of other white cereal products ⩾21/week versus 0–1/week (aOR 3.39, 95% CI 1.02–11.25); salty snacks were not independently associated. Among cases, 68.8% had mild acne, 21.1% moderate, and 10.1% severe/very severe. In the severity model, age was associated with moderate/severe acne (aOR 1.23 per year, 95% CI 1.00–1.50), while diet variables were not significant.
Conclusion:
In this unmatched case–control sample, acne was independently associated with overweight BMI and high intake of other white cereal products, while salty snack intake did not remain significant after adjustment. The observed association with female sex should be interpreted cautiously because different recruitment sources for cases and controls may introduce selection bias and reflect healthcare-seeking or participation differences rather than a population risk effect. Findings should be interpreted as associations that may be influenced by sampling and self-reporting biases. Prospective and interventional studies are needed to clarify whether dietary factors independently contribute to acne risk and severity.
Background
Acne vulgaris is a common chronic inflammatory disorder of the pilosebaceous unit (the hair follicle and sebaceous gland complex). It typically presents with open and closed comedones, inflammatory papules, and pustules, and in more severe disease, it can progress to nodules or cysts, post-inflammatory scarring, and dyspigmentation.1,2 From a population perspective, acne is most frequent during adolescence and early adulthood, and community studies often report that a large majority of adolescents are affected at some point. Importantly, a meaningful proportion of individuals continue to experience acne beyond adolescence, and persistent or late-onset acne is commonly reported among women.2,3
Acne can create a substantial psychosocial burden, including reduced quality of life, embarrassment, social withdrawal, and symptoms of anxiety or depression, even when lesions appear clinically mild. 4 While many cases are self-limited, evidence-based treatment is recommended when acne is persistent, inflammatory, scarring, or distressing. Current guideline-based management typically uses topical retinoids and benzoyl peroxide (alone or in combination), with escalation to topical or oral antibiotics (used with benzoyl peroxide to reduce resistance), hormonal therapy (for example, combined oral contraceptives or spironolactone where appropriate), or oral isotretinoin for severe or refractory acne.5,6
Acne is multifactorial, reflecting interactions among genetics, endocrine factors, sebum production, follicular hyperkeratinization, inflammation, and the cutaneous microbiome. 2 Genetic susceptibility is increasingly supported by studies of acne-associated variants. 1 In parallel, modifiable lifestyle factors, including body weight and dietary patterns, have attracted renewed interest because they may influence endocrine signaling and inflammatory pathways relevant to acne. 7
Diet-related factors remain debated, but the evidence base has grown in the last decade. A recent systematic review concluded that higher glycemic index or glycemic load patterns show a modest but statistically significant pro-acne association, and randomized trials in some settings support clinical improvement with lower glycemic load approaches. 8 Evidence synthesis also indicates that dairy intake is associated with higher odds of acne, although heterogeneity and bias across observational studies mean results should be interpreted cautiously.9,10 In parallel, evidence syntheses examining Mediterranean diet (MD) adherence suggest potential links with acne severity, but the overall certainty of evidence has been rated as low, and heterogeneity is substantial. 11 Small randomized studies also suggest that omega-3 fatty acids may offer adjunctive benefit for inflammatory lesions, but effect sizes vary, and replication across populations is needed. 12
In Palestine, published work on acne is emerging, including data among medical students documenting high prevalence, quality-of-life impairment, and diet-related correlations. 13 However, evidence remains limited regarding acne in relation to nutrition patterns and eating-related risk screening in community-based young adults, particularly when multiple nutrition-related domains are examined simultaneously and adjusted for key confounders such as sex and BMI. Therefore, this study aimed to evaluate associations between acne status and nutrition-related variables, including BMI, MD adherence, acne-related food intake frequency, and eating disorder risk screening, among young adults in Hebron, Palestine, recognizing that observational findings indicate associations rather than causation.
Methods
Study design, settings, and population
This unmatched case–control study was conducted in Hebron, Palestine, between February and April 2023 among young adults aged 18–25 years. Cases were acne patients recruited from dermatology clinics, and controls were acne-free individuals recruited from the community (universities, social media). Data included sociodemographic characteristics, self-reported anthropometrics (BMI category), nutrition-related measures (MD adherence and acne-related food frequency), eating-disorder screening, and clinician-assessed acne severity (cases only). Findings should be interpreted in the context of the study setting and recruitment sources.
Sample size calculation and sampling method
Sample size was determined using G*Power (alpha 0.05, two-sided, power 80%). The a priori calculation assumed a 1:1 allocation (100 cases, 100 controls) for the primary case–control comparison. Because a secondary objective was to explore dietary patterns across acne severity categories, we oversampled cases (approximately 2:1 case–control ratio) to improve precision for severity-stratified analyses, while keeping the primary analyses focused on acne status. Using the same assumptions as the a priori calculation, we re-checked that the final sample size and allocation provided at least 80% power for the primary comparison.
A total of 200 eligible acne patients and 100 eligible controls were approached/recruited. After applying the pre-specified eligibility criteria and conducting data cleaning for completeness, the final analyzed sample comprised 199 acne cases and 101 controls (N = 300). Specifically, one case was excluded due to missing key questionnaire data required for the main analyses, and one additional eligible control was included to maintain the completeness of the control dataset. While increasing the number of controls per case can improve statistical efficiency (with diminishing returns beyond ~4 controls per case), we oversampled cases because severity-stratified analyses required sufficient numbers within severity categories.
Cases were recruited by convenience sampling from dermatology clinics in Hebron. Controls were recruited voluntarily through universities and social media from the same age range and geographic area. Controls were not individually matched to cases; therefore, we treated the study as an unmatched case–control design and planned adjustment for key imbalances (e.g. sex and BMI) in multivariable analyses.
Inclusion criteria (cases) were male and female patients aged 18–25 years presenting with acne as a chief complaint. Controls were acne-free and reported no prior skin disorder requiring medical intervention. Exclusion criteria for both groups were chronic GI disease that required a strict diet or affected lifestyle, for example, celiac disease or inflammatory bowel disease (IBD), psychological disorder, and autoimmune diseases with skin manifestations. Participants with incomplete responses on core exposure or outcome variables were excluded from the relevant analyses (complete-case approach) to ensure valid comparisons.
Ethical considerations
The research protocols adhered to the guidelines outlined in the Declaration of Helsinki and were reported in accordance with the STROBE checklist for case–control studies. The study protocol obtained approval from the Ethical Committee of the Deanship of Scientific Research at Palestine Polytechnic University in 2019, under reference number KA/41/2022. Written informed consent was obtained from all participants before data collection.
Data collection and research tool
Data were collected by four trained nutritionists. Non-diet variables were collected using a brief author-developed self-administered questionnaire, and dietary variables were collected using structured interviews by trained nutritionists. Acne diagnosis and severity (cases only) were assessed by dermatologists; dermatologists did not collect dietary data. Dermatologists were not blinded to dietary responses; therefore, observer bias cannot be excluded. Controls completed the same non-acne components. The English version of the questionnaires is provided in Supplemental File.
The collected data included: (1) demographic data: age, sex, marital status, area of living, living status, level of education, and average household income and (2) nutrition-related data: anthropometric data and BMI were self-reported and were used to evaluate the participants’ weight status, and the WHO cut-off points were employed to classify them into categories of underweight, normal weight, overweight, and obese.
The adherence to the MD dietary pattern and acne-related food frequency questionnaire was done using the validated Arabic version of MD Adherence Screener (MEDAS). 14 The food frequency questionnaire form utilized in this study on acne was obtained from a recently published research after obtaining permission from the corresponding author. 15 This questionnaire comprises 14 items assessing the main components of Mediterranean diet adherence, including olive oil use, olive oil intake, vegetable intake, fruit intake, red meat intake, butter/margarine/cream intake, sugar-sweetened beverage intake, wine consumption, pulse intake, fish/seafood intake, commercial pastry intake, nut intake, preference for white over red/processed meat, and consumption of dishes prepared with tomato, garlic, onion, or leeks sautéed in olive oil. The purpose of this questionnaire is to ascertain the frequency of consumption of these food items among the participants. We focused on commonly consumed food items in the Palestinian context; therefore, the questionnaire did not differentiate milk types (e.g., skimmed versus full-fat), which may limit comparisons with studies emphasizing low-fat dairy.
The eating disorder screening was done using the validated Arabic version of the SCOFF questionnaire, which consists of five binary questions, where respondents are required to answer either “yes” or “no.” The overall score is obtained by summing the number of affirmative responses to the five yes/no items on the SCOFF questionnaire. A proposed threshold value of 3 has been recommended as the optimal balance between sensitivity and specificity. 16 A meta-analysis conducted by Kutz et al. (2020) supported the effectiveness of the SCOFF as a reliable screening tool for identifying young participants who are at risk of developing anorexia nervosa (AN) and bulimia nervosa (BN). 17 SCOFF was used as a screening measure (not a diagnostic tool).
The questionnaire was pilot-tested in 30 participants (10% of the target sample) to assess clarity, comprehension, and completion time; minor wording revisions were made accordingly before full data collection.
Acne severity
Severity was assessed by dermatologists using GAGS and categorized as mild (1–18), moderate (19–30), severe (31–38), or very severe (39 or higher). 18 Acne severity analyses were conducted as secondary analyses and were evaluated analytically (severity regression) rather than reported only as descriptive percentages.
Statistical analysis
Analyses were conducted using IBM SPSS Statistics version 23.0. Continuous variables were summarized as mean (SD) and categorical variables as n (%). Acne versus control comparisons used an independent-samples t-test (continuous) and a chi-square test (categorical), two-sided, P < 0.05. For the primary outcome (acne status), multivariable logistic regression was performed to adjust for potential confounding, including sex, age, BMI category, household income, and key dietary variables, and results were reported as adjusted odds ratios with 95% confidence intervals. For severity, a secondary multivariable logistic regression was conducted among acne cases only to compare moderate or severe acne versus mild acne. Participants with incomplete responses on core exposure or outcome variables were excluded from the relevant analyses (complete-case approach) to ensure valid comparisons.
Results
Participants’ sociodemographic characteristics
Table 1 outlines the sociodemographic and nutrition-related characteristics of the study participants. A total of 300 individuals were included, comprising 199 acne cases and 101 controls. The mean age of participants did not significantly differ between the acne group (19.70 ± 1.7 years) and the control group (19.75 ± 1.4 years, P = 0.823).
Sociodemographic characteristics and nutrition-related data according to the group presented in n (%).

Significant at P < 0.05 using chi-square test.
A statistically significant difference was observed in sex distribution (P = 0.001), with a higher proportion of females in the acne group (76.9%) compared to the control group (59.4%). Given that cases and controls were recruited from different sources (clinics versus community), this sex imbalance is described as a sample characteristic and should not be interpreted as reflecting population prevalence. No significant differences were found between groups with respect to living location (P = 0.383), marital status (P = 0.083), income level (P = 0.115), or living status (P = 0.200).
Regarding body mass index (BMI), a significantly higher proportion of participants in the control group had a normal weight (80.2%) compared to the acne group (63.3%) (P = 0.002). MD adherence, assessed by MEDAS categories, did not differ significantly between groups (P = 0.555), with most participants showing moderate adherence in both groups.
Table 2 presents dietary intake data (unadjusted comparisons) based on servings per week. Most food groups did not show statistically significant differences between the acne and control groups. In these unadjusted analyses, white cereal product intake, were significantly higher in the acne group (5.66 ± 9.71 servings/week) compared to the control group (3.28 ± 5.82 servings/week, P = 0.024), indicating a potential association between high intake of refined cereals and acne. Moreover, salty snacks were also consumed more frequently among acne cases (7.95 ± 9.65 servings/week) than controls (5.62 ± 7.10 servings/week, P = 0.033).
Acne-specific Food Frequency Questionnaire (Acne-FFQ).
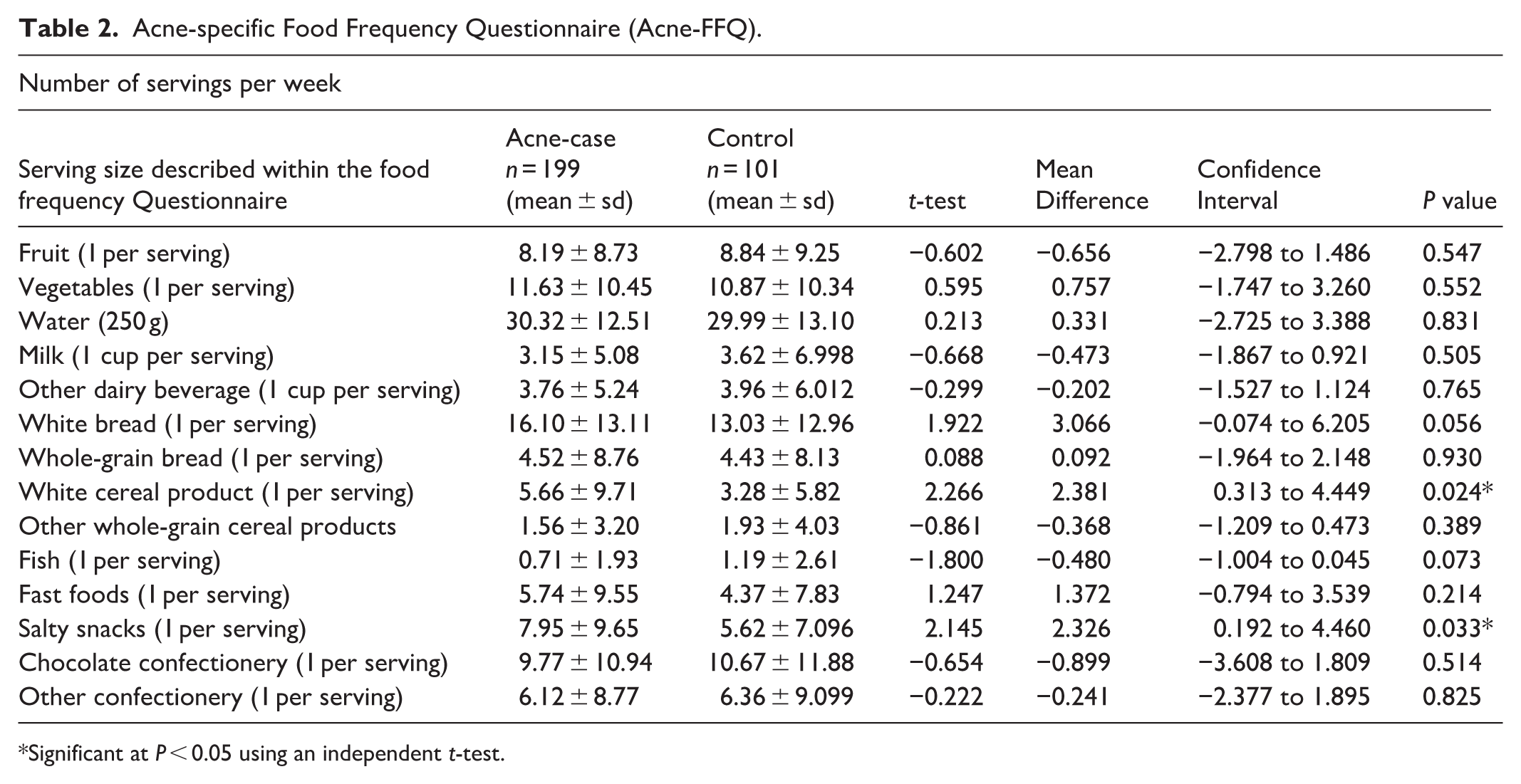
Significant at P < 0.05 using an independent t-test.
Although white bread consumption approached significance (16.10 ± 13.11 in acne cases versus 13.03 ± 12.96 in controls; P = 0.056), it did not reach the threshold. Other food items such as fruits, vegetables, water, dairy products, fast foods, chocolate, and confectionery showed no significant differences between groups.
Eating disorder screening
The prevalence of disordered eating, as assessed by the SCOFF questionnaire, did not significantly differ between the acne and control groups. Figure 1 illustrates the distribution, confirming no statistical association between SCOFF screening status and acne group in the unadjusted chi-square comparison (P > 0.05).

Eating disorders of the case and control group.
Acne severity among the acne cases
Figure 2 displays the severity distribution of acne among the 199 acne cases. A majority (68.8%, n = 137) had mild acne, followed by moderate acne in 21.1% (n = 42), severe acne in 7.5% (n = 15), and very severe acne in 2.5% (n = 5). This suggests that most participants had low to moderate severity.

Degree of acne among the case group.
Independent associations with acne status
In multivariable logistic regression adjusting for age, sex, household income, and BMI category (Table 3), female sex was associated with higher odds of being classified as an acne case in this clinic-recruited case versus community control comparison (aOR = 2.66, 95% CI 1.50–4.72; P = 0.001), and overweight was associated with higher odds of acne case status (aOR = 2.72, 95% CI 1.29–5.75; P = 0.009). Compared with participants consuming other white cereal products 0–1 times/week, consumption ⩾21 times/week was associated with higher odds of acne case status (aOR = 3.39, 95% CI 1.02–11.25; P = 0.046), whereas salty snack intake was not independently associated with acne case status after adjustment. These estimates should be interpreted in the context of the unmatched design and different recruitment sources for cases and controls.
Multivariable logistic regression for adjusted odds of acne case status (clinic-recruited cases versus community controls) among young adults in Hebron (N = 300).
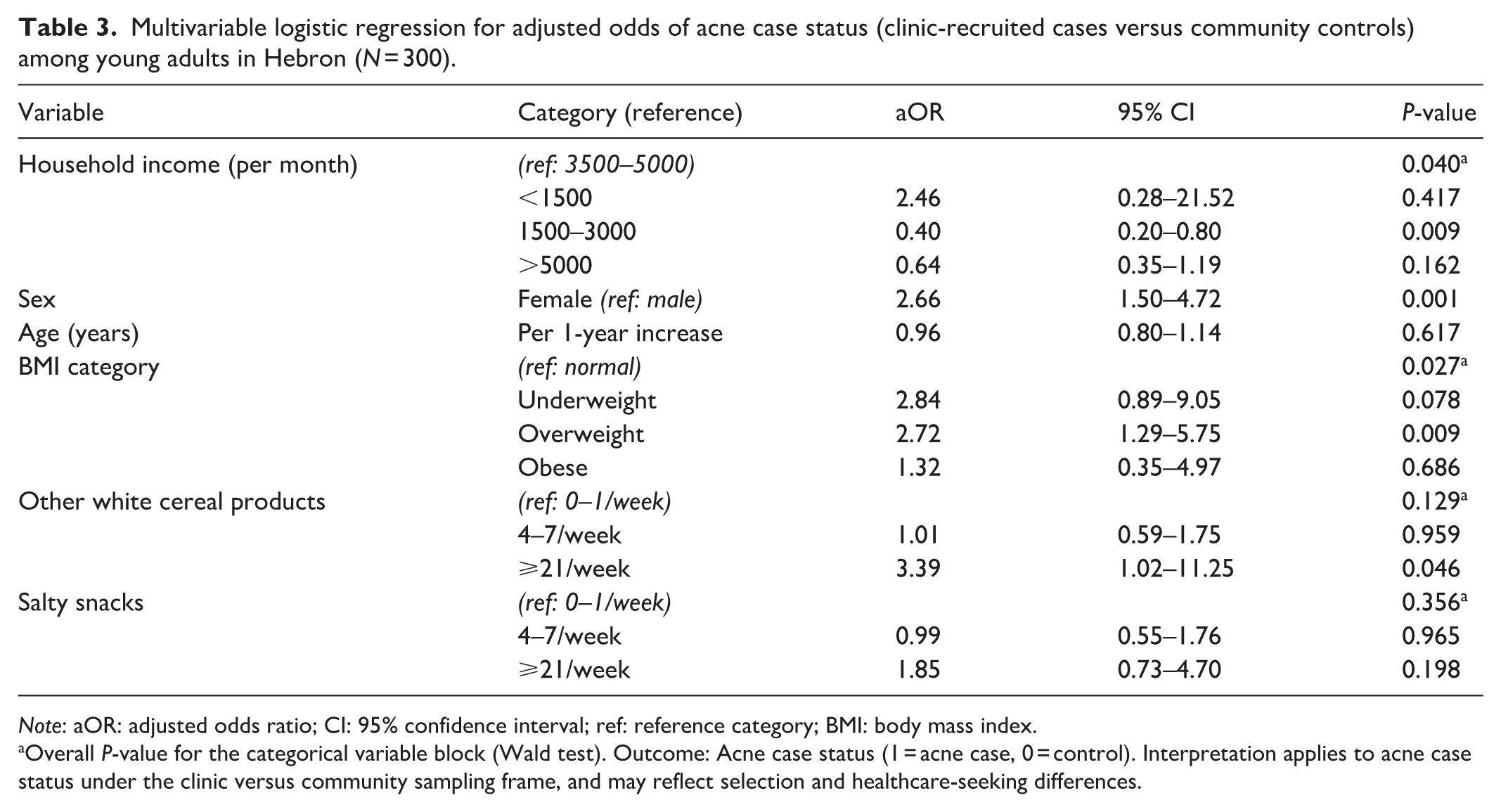
Note: aOR: adjusted odds ratio; CI: 95% confidence interval; ref: reference category; BMI: body mass index.
Overall P-value for the categorical variable block (Wald test). Outcome: Acne case status (1 = acne case, 0 = control). Interpretation applies to acne case status under the clinic versus community sampling frame, and may reflect selection and healthcare-seeking differences.
Acne severity analysis (cases only)
Among acne cases (N = 199), we performed multivariable logistic regression comparing moderate/severe versus mild acne, adjusting for sex, age, BMI category, household income, and dietary frequency categories (see Table 4). Age was associated with higher odds of moderate/severe acne (aOR = 1.23 per year, 95% CI 1.00–1.50; P = 0.045). High consumption of other white cereal products (⩾21/week) showed a borderline association with greater severity compared with 0–1/week (aOR = 2.77, 95% CI 0.92–8.34; P = 0.070), whereas salty snack intake was not associated with severity (P = 0.968). Because severity analyses were secondary and the number of moderate/severe cases was limited, these findings should be interpreted as exploratory.
Multivariable logistic regression for adjusted odds of moderate/severe acne (versus mild) among acne cases (N = 199).
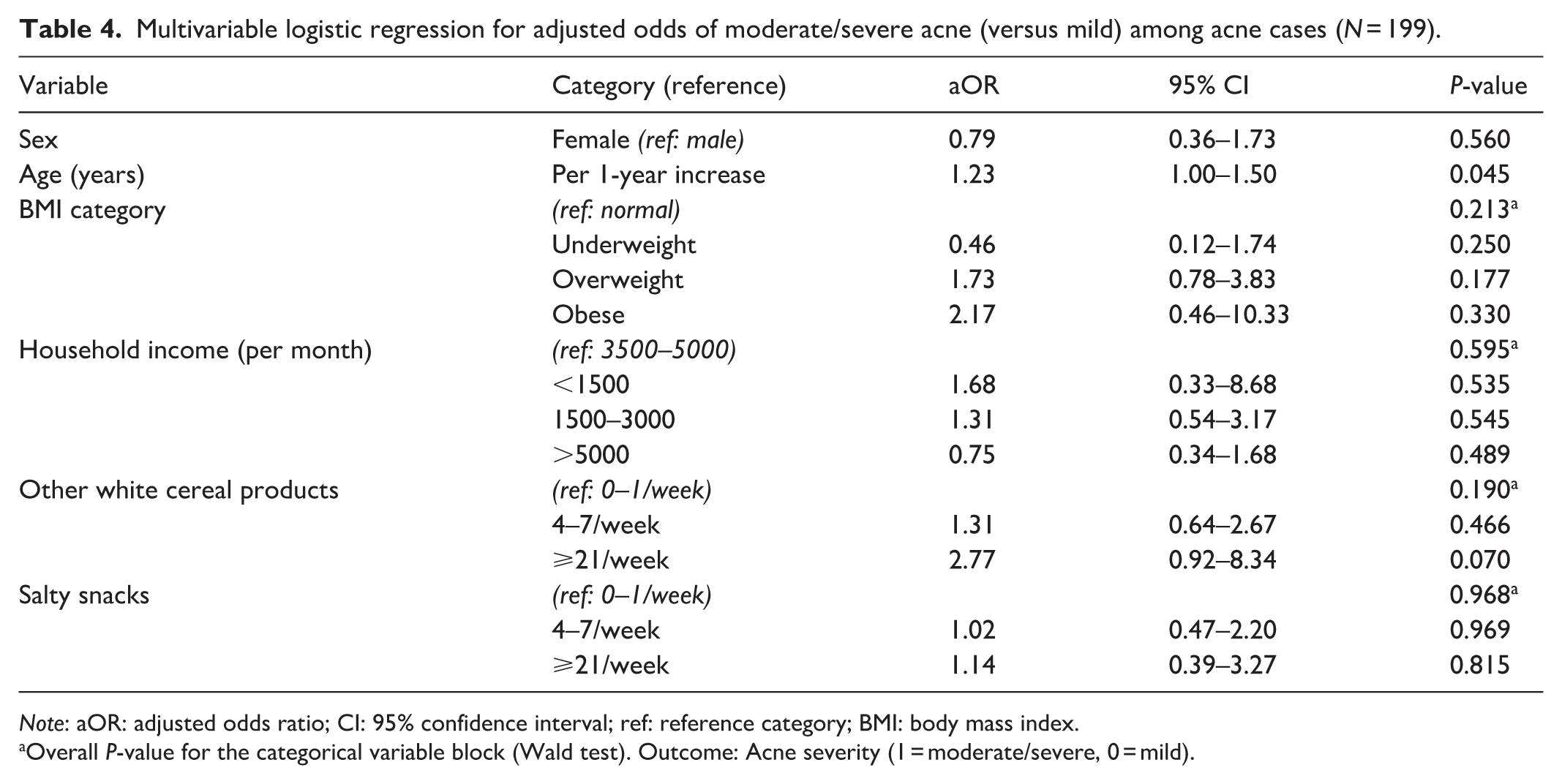
Note: aOR: adjusted odds ratio; CI: 95% confidence interval; ref: reference category; BMI: body mass index.
Overall P-value for the categorical variable block (Wald test). Outcome: Acne severity (1 = moderate/severe, 0 = mild).
Discussion
This study found that acne status in young adults in Hebron was independently associated with a small set of demographic and nutrition-related factors, while several hypothesized diet patterns and psychosocial factors were not supported. Abnormal BMI categories and frequent intake of refined, white cereal foods differentiated cases from controls, and these associations persisted after multivariable adjustment. In contrast, MD adherence and SCOFF screened disordered eating did not differ meaningfully between groups. Among participants with acne, severity was more closely related to participant characteristics than to the measured dietary exposures. In descriptive analyses, age did not differ between acne cases and controls, and there were no significant group differences in living location, marital status, household income, or living status, which suggests that the observed differences were more concentrated in sex distribution, BMI category, and selected dietary frequencies.
In our adjusted model, female sex remained associated with acne case status, which is consistent with evidence that acne burden is often higher in women and that post-adolescent acne is commonly reported among women, although the magnitude of sex differences varies across studies depending on outcome ascertainment and recruitment setting.19,20 However, because cases were recruited from dermatology clinics and controls from community sources, this coefficient may partly reflect selection mechanisms, including sex differences in healthcare-seeking, self-perception, and willingness to participate, rather than a causal or population-level risk effect. Importantly, the higher proportion of females among cases in this study should not be interpreted as evidence that acne is more common among females in the general Palestinian population because the imbalance likely reflects recruitment patterns and healthcare seeking rather than underlying prevalence. Accordingly, sex is best interpreted here as a confounder requiring adjustment and as an indicator of potential selection bias, rather than as a definitive independent risk factor.
BMI emerged as an important correlate in the bivariate comparisons, and overweight remained independently associated with acne in the adjusted model. This is consistent with evidence linking acne with metabolic and endocrine correlates, including insulin resistance, even though the strength and direction of BMI associations have been inconsistent across studies and settings.19,21 The insulin resistance pathway remains a plausible contextual explanation because hyperinsulinemia can increase IGF-1 signaling and downstream sebaceous activity and inflammation, which may contribute to acne expression in susceptible individuals.11,21,22 At the same time, some studies have reported weak or null BMI associations after accounting for diet, puberty timing, and socioeconomic factors, suggesting that BMI may function partly as a proxy for correlated exposures rather than a direct driver.11,19 In our setting, BMI may also reflect recent dietary transitions and reduced physical activity among university-age adults, which could co-occur with higher intake of rapidly absorbable carbohydrates.
Dietary comparisons showed higher reported intake of refined, white cereal foods and salty snacks among cases, with a directionally opposite trend for fish. However, the adjusted model clarified the relative contribution of these exposures. Very frequent intake of refined, white cereal foods remained associated with acne after adjustment, while salty snack intake did not retain an independent association, a pattern that aligns with evidence linking higher-glycemic dietary patterns to acne but can differ from some observational cohorts where energy-dense snack-type foods remain independently associated. Such differences likely reflect variation in exposure definitions, cultural dietary context, and confounder control rather than a true biological contradiction.10,23,24
A plausible interpretation is that refined cereal foods may capture habitual glycemic exposure more directly in this population, whereas salty snacks may be more episodic, more vulnerable to recall error, or more strongly correlated with unmeasured behaviors that attenuate after adjustment. The inverse trend for fish is directionally consistent with anti-inflammatory hypotheses related to omega-3 fatty acids, although recent evidence still supports only modest and context-dependent effects, and the strongest causal inference remains limited by trial size and heterogeneity. 25
MD adherence did not differ between cases and controls and did not contribute independently in the adjusted acne model. This null finding is compatible with recent literature suggesting that MD signals, when present, may be more detectable for within-case severity differences than for acne presence versus absence, and adherence scores may not adequately capture the specific components most relevant to acne biology (e.g. glycemic quality, dairy subtype, and ultra-processed foods).11,26 In Palestine, Mediterranean-like foods may be common across both groups, which reduces contrast and limits the ability of a short adherence score to discriminate relevant dietary patterns. It is also possible that specific components, such as glycemic quality, dairy type, or ultra-processed foods, are more predictive than an overall Mediterranean adherence score in young adults.8,23
A key psychosocial finding was the absence of a detectable association between acne and SCOFF-screened disordered eating. This null result is plausible but requires careful interpretation. Acne can be associated with body image concerns and emotional distress, yet the pathway to clinically meaningful eating pathology is not universal and may depend on severity, duration, comorbid anxiety or depression, and baseline vulnerability.19,27 In addition, screening tools can underestimate disorder prevalence outside the high-risk populations in which sensitivity is highest. A diagnostic accuracy meta-analysis found that the SCOFF performs best in case–control designs involving young women with anorexia nervosa or bulimia nervosa, while sensitivity tends to be lower in broader community samples and for detecting the full range of DSM-5 eating disorders.17,28 Sample size and statistical power likely constrained detection of small to moderate associations, particularly if the true effect is mediated by psychological distress rather than directly related to acne status. These points align with broader screening evidence showing that population-level screening benefits remain uncertain, and tool performance varies by setting and subgroup. 29 Therefore, our null association should be interpreted as “no detectable relationship using this screening approach in this sample,” rather than evidence that acne and disordered eating are unrelated.
Finally, the two regression analyses add useful nuance to address earlier concerns about confounding and the role of severity. The acne status model supports independent associations for BMI category and very frequent refined cereal intake after adjustment, clarifying that not all bivariate dietary differences persist once key confounders are accounted for. The sex coefficient should be interpreted cautiously as noted above because recruitment source differences can induce selection bias. The severity model restricted to cases suggests that participant characteristics, rather than the measured dietary exposures, are more consistently related to severity in this dataset. This divergence is consistent with broader evidence that diet–acne associations are often modest and context dependent, and that within-case severity may be influenced by factors not captured here, such as treatment use, hormonal profiles, stress, lesion duration, and care-seeking behaviors.8,19,20 Because severity analyses were secondary and the distribution of severity categories limited precision, these results should be presented as exploratory, hypothesis-generating findings that justify larger, prospectively designed studies with more granular dietary assessment and stronger control of selection and information bias.
Implications
These findings have practical implications for Palestine. Clinically, dermatology and primary care services can add brief, non-stigmatizing lifestyle counseling that prioritizes sustainable dietary quality, particularly reducing frequent refined grain exposures and supporting healthy weight, while avoiding overly restrictive acne diets that may worsen distress. Educationally, university health programs in Hebron can integrate evidence-based acne self-care modules that combine skin care literacy, nutrition basics, and guidance on when to seek treatment. From a policy perspective, campus and community initiatives that improve access to affordable, healthier staples, including whole grains and minimally processed options, may have downstream benefits for metabolic health and possibly acne-related outcomes, although causal effects should not be assumed.
Strengths and limitations
Key strengths include the study’s focus on an understudied Palestinian context, with a case–control design that addresses a local evidence gap on acne and nutrition-related variables. Clinical acne severity was assessed by dermatologists using a standardized grading tool (GAGS), supporting outcome measurement quality, and multivariable logistic regression addressed reviewer concerns about unadjusted comparisons by adjusting for key confounders, including sex, age, BMI, and income.
Several limitations should shape interpretation. The study was observational and unmatched, therefore, findings support associations and cannot establish causality. Cases and controls were recruited from different sources (dermatology clinics versus universities and social media), which may introduce selection bias and reduce comparability due to differences in healthcare-seeking behavior and socioeconomic characteristics, with residual confounding possible despite adjustment. Accordingly, the sex coefficient in the adjusted model should be interpreted as an association with case status in this sampling frame, not as evidence of a population-level risk effect. Because controls may not represent the exposure distribution of the source population that generated the clinic cases, selection and participation mechanisms may partly explain the observed sex imbalance. The female predominance among cases likely reflects recruitment patterns rather than true population prevalence differences and should not be overinterpreted. Dietary intake and BMI were self-reported, which increases the risk of recall and reporting bias and may attenuate or distort associations. Acne assessment and dietary data collection were separated operationally, which reduces the likelihood of differential outcome assessment by dietary exposure, although formal blinding procedures were not implemented and some observer bias cannot be fully excluded. Eating disorder risk was measured using the SCOFF screening tool, which is not diagnostic and may have limited sensitivity in community settings; therefore, the null association should be interpreted cautiously. Finally, severity analyses were secondary and may not have been separately powered, and the number of moderate to severe cases was relatively small, which limits precision. Because acne is not rare in this age group, odds ratios should not be interpreted as approximations of risk ratios or risk differences when communicating implications to non-technical audiences.
Conclusion
In summary, this study suggests that, among young adults in Hebron, acne status is more closely aligned with BMI category and frequent refined cereal intake than with MD adherence or screened disordered eating. Although female sex was associated with acne case status after adjustment, this finding is not methodologically sufficient to infer that female sex is a population-level risk factor, given the different recruitment sources for cases and controls and the resulting potential for selection bias. The null eating disorder finding should be interpreted cautiously, given screening limitations and sample size, but it indicates that acne-related counseling should avoid assuming eating pathology while still attending to psychosocial well-being. Larger and more methodologically robust Palestinian studies are needed to guide culturally tailored prevention and management strategies. Overall, these findings should be interpreted as associations rather than evidence of prevalence differences or causality, given the observational, unmatched design, self-reported exposures, and recruitment from different sources.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121261431476 – Supplemental material for Eating disorder, dietary pattern, and nutritional behavior among patients with acne vulgaris: A case–control study
Supplemental material, sj-pdf-1-smo-10.1177_20503121261431476 for Eating disorder, dietary pattern, and nutritional behavior among patients with acne vulgaris: A case–control study by May Hamdan, Loai M. Zabin, Tasneem Abu Snoubar, Haneen Ghneimat, Jannat Ebido, Yasmen Abu Sharkh, Manal Badrasawi and Ali Shakhshir in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge the patients and the participants who participated in the study and agreed to join the study. Also, the author would like to acknowledge the dermatologists who classified the severity of the acne status.
Ethical considerations
The study protocol was approved in 2022 by the Ethical Committee of the Deanship of Scientific Research at Palestine Polytechnic University (Reference No. KA/41/2022). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before enrolment and data collection.
Consent of publication
No individually identifiable participant data are presented in this manuscript.
Author contributions
The authors have contributed to the manuscript as follows: MB, the principal investigator, has written the study proposal and protocol and supervised the data analysis. MH: supervised the data collection and applied for the ethical approval. TA: data cleaning and writing the first draft of the manuscript. HG, JE, and YA: draft the proposal, data collection, data entry, and primary data analysis. LMZ: rewrote the manuscript and formatted the tables and figures, and performed sensitivity analysis. AS: prepared and submitted the manuscript to the journal. All the authors approved the final version of the manuscript file.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset supporting the findings of this study is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.