
Abstract
Background:
The intensive care unit (ICU) is a setting where critically ill and high-risk patients undergo intensive therapy under continuous monitoring. Throughout their stay, patients undergo multiple tests and a range of medical and surgical procedures, with each case presenting various risk factors and complications. The study sought to evaluate risk factors in ICUs and identify those that present the greatest risk.
Methods:
A cross-sectional study was conducted among ICU patients with risk factors who developed complications during their stay. Forty-seven patients of diverse ages and genders were admitted to the ICU. The analysis was conducted using IBM SPSS 26.
Results:
Analysis of the patient data regarding hospital stay and discharge conditions indicated no statistically significant difference (P > 0.05). In relation to ventilation techniques, a statistically significant difference (P < 0.05) was observed when comparing it with hospital stay duration; patients who remained in the ICU for more than 20 days encountered various ventilation techniques (18 patients). A statistically significant association was observed on Day 5 for the Cured group (P = 0.034). Fluid balance on Day 2 showed a highly statistically significant relationship with the Cancer system (P < 0.001). The odds ratio (OR) was 1.081 (95% CI: 1.076–1.086). A negative fluid balance correlated with decreased mortality rates, shorter hospitalization durations, and a reduced incidence of sepsis.
Conclusions:
A prolonged hospital stay correlates with elevated mortality rates, increased infection risk, and a higher incidence of complications. The past medical history and fluid balance of each patient are essential factors in identifying the most appropriate therapeutic strategy.
Keywords
Introduction
The intensive care unit (ICU) is a specialized hospital ward designed to manage critically ill and high-risk patients, providing rigorous therapy and continuous monitoring using both invasive and non-invasive methods. These devices provide medical practitioners with continuous updates on patients’ physiological characteristics, facilitating the administration of titrated therapy. 1
Patients in the ICU are individuals with life-threatening conditions and injuries necessitating critical medical intervention. Throughout their stay, individuals undergo multiple tests and medical or surgical procedures, each presenting distinct risks and complications that may influence the efficacy of the healing process. 2
ICU patients may experience various complications, including multi-organ failure, circulatory issues, cardio-respiratory arrest (CRA), deep vein thrombosis (DVT), hypothermia, hypotension, renal dysfunction, hemorrhagic shock, myocardial infarction, and sepsis, all of which pose significant threats to life. 3 Risk assessment offers essential insights for determining risk reduction strategies, enhancing current control systems, and formulating suitable response plans. 2 Investigating risk factors for outcome complications in ICUs is essential to enhancing patient care. The intricacy of ICU cases requires a comprehensive understanding of possible complications. Age, comorbidities, and illness severity are frequently examined in these studies. The influence of pre-existing conditions on ICU outcomes represents a critical area of research inquiry. The type and duration of mechanical ventilation are critical factors in predicting complications, significantly increasing the risk of lung or cardiac compromise and systemic inflammation, such as ventilator-associated pneumonia; many of these complications should be avoided or minimized. 4
Patients in ICUs face risks such as blood clots, infections, organ failure, and complications arising from prolonged immobilization. Additionally, age and pre-existing medical conditions may influence the outcomes. Effective management of these hazards requires prompt medical intervention and regular monitoring. 5 Pharmacological interventions and their associated side effects complicate ICU cases. Antimicrobial agents are routinely used in the ICU to treat infections, a common problem among critically ill patients. Antibiotic selection is frequently guided by culture and sensitivity results, which target specific infections.6,7 Nutritional status and the adequacy of support are essential determinants of patient recovery. Examining healthcare providers’ experience and staffing levels on outcomes yields significant insights. The timing and appropriateness of interventions, such as surgery, significantly influence patient prognosis. Recognizing the complications underscores the importance of early identification and management of sepsis to prevent negative outcomes. 8
A prospective observational study was conducted between July 25 and August 18, 2024. The selection of study participants was convenient, and participants matched the selection criteria. A total of 47 patients were admitted to the ICU at Shar Teaching Hospital for various causes, aged 10–77 years, and participated in the study.
Materials and methods
Study design and setting
A prospective observational study was carried out from July 25 to August 18, 2024. The study participants were selected based on convenience and met the established selection criteria. A total of 47 patients, aged 18 to 77 years, were admitted to the ICU at Shar Teaching Hospital for various reasons and participated in the study.
Data collection tools and methods
The patient flow process encompassed admission to discharge, including triage, assessment, care, and transfer. The reasons for sampling included diagnosis, continuous monitoring, and assessment of clinical outcomes. Following the collection of their medical history and current health status, including drug history, chronic conditions, social history, ventilation methods, and any complications encountered during their ICU stay, we assessed their fluid balance over a 7-day follow-up period. The ventilation technique was considered, as numerous changes in ventilation occur during ICU stays. Patients used the device; some were transferred, while others were discharged home. The existing ICU chart facilitated the process, minimizing disruption to patients and their families. The chart included data on vital signs, medications, and fluid intake and output, which were utilized to assess fluid balance. On each visiting day, as new complications emerged, we investigated the underlying causes and noted the necessary management strategies implemented. The patient’s progress was monitored in the ICU until transfer to the wards, discharge, or death occurred. The medical terminology used to describe patient progress as a discharge criterion includes “Cured,” indicating full recovery and direct discharge from the ICU. Partially cured: advancing towards complete recovery and transition to a general ward. No improvement observed since discharge; patient remains in ICU. Died: Cease to exist. The information and parameters were gathered using a case-recording sheet developed by the authors. The form includes fundamental socio-demographic characteristics, conditions of admission and discharge, complications, and a fluid balance chart, which encompasses fluid input, NG/feeding, and fluid output.
Statistical analysis
Statistical analyses were conducted utilizing IBM SPSS (Statistical Package for the Social Sciences; IBM Corp) version 26. Quantitative data were expressed as means. Qualitative data were reported as frequencies and percentages. The chi-square (χ²) test was employed to determine the relationship between categorical variables. Multinomial logistic regression is a statistical method used to predict the outcome of a categorical dependent variable that has multiple discrete levels or classes. A P-value of ⩽0.05 was deemed statistically significant.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki 9 and received approval from the Ethics Committee of the College of Health and Medical Technology, Sulaimani Polytechnic University (Approval No. 3, dated June 9, 2024). Informed verbal consent for participation and data use was obtained from the patients or their Legally Authorized Representative prior to death, in accordance with institutional and international ethical standards. Given the patients’ inability to respond, the study’s objectives were clearly explained to the patients’ companions at the outset of each interview, and informed verbal consent was obtained. This verbal consent procedure was specifically approved by the Ethics Committee. Throughout the study, strict measures were taken to ensure the privacy and confidentiality of all participants. Participants were explicitly informed of their right to withdraw from the study at any stage without any consequences. Any adverse events occurring during the study were promptly addressed, and appropriate medical care was provided.
Inclusion criteria
Patients admitted to the ICU were included in the study.
Patients aged 18 years or older were included in this study.
All individuals were included, regardless of gender or religion.
The included patients were companions who accepted and were prepared to participate.
Exclusion criteria
Individuals under the age of 18 were excluded from this study.
Those not prepared to participate were excluded from the study.
The patients excluded were those companions who declined to participate.
Results
This study involved 47 participants, of whom 68.1% identified as male and 31.9% as female. A significant proportion (44.7%) were aged 60 years or older. About 42.5% of the participants exhibited hypertension, while 21.2% were diagnosed with diabetes mellitus (Figure 1).

Distribution of patients’ medical history.
Sociodemographics
Throughout the patient’s ICU stay, 23 individuals experienced no complications, 11 encountered 1–2 complications, eight encountered 2–3 complications, and five encountered more than three complications. A significant proportion of female patients presented with brain conditions (46.7%), similarly observed in male patients (43.8%). Additionally, seven male patients were identified with urinary conditions (21.9%). The association was statistically significant, indicated by a P-value of 0.03. Among 21 cases aged 60 years or older, 7 (33.3%) had brain conditions. In contrast, among the 13 cases aged 20–40 years, 8 (61.5%) presented with brain conditions. The data demonstrates statistical significance, indicated by a P-value of less than 0.05 (0.04). Among the 23 patients without complications, 9 (39.1%) presented with brain conditions; the P-value was greater than 0.05 (0.08). The data in this table indicate that ICU patients have a higher prevalence of brain conditions than patients in other systems (Table 1).
Distribution of exposed systems by certain sociodemographics and the number of complications.

GIT: gastrointestinal tract.
Discharge conditions
Figure 2 illustrates the relationship between patient count and discharge conditions. Of the patients, 11 (23.4%) remained in the ICU, 12 (25.5%) were cured, six (12.8%) died, and 18 (38.3%) were partially cured and transferred to hospital wards (Figure 2).

Discharge conditions of the patients.
Hospital staying
Table 2 outlines the correlation between age group and duration of hospital stay, along with discharge status. In terms of hospital stays, 18 patients (38.3%) were admitted for less than 10 days, 11 patients (23.4%) for 10 to 20 days, and 18 patients (38.3%) for more than 20 days. Patients indicate that individuals over 60 years exhibit longer ICU stays (10–20 days) at a rate of 63.6% and a higher mortality rate of 66.7%. The data are not significant, as the P-value s exceed 0.05 (Table 2).
Age group association with hospital stay and discharge conditions.

Chi-square test and Fisher’s exact test applied.
Ventilation techniques
Table 3 presents the different ventilation applications by system used, the complications encountered by each patient, and the duration of hospital stay. A total of 21 patients (44.6%) were admitted for brain conditions, followed by urinary conditions (seven cases, 14.8%) and both cardiac and respiratory conditions (five cases each, 10.6%). The majority of brain cases (21) were primarily treated with CMV (5), while a new combined technique (PCV-VG) was also utilized frequently (4). However, the data are not statistically significant, as the P-value exceeds 0.05. Among the 23 cases without complications, nine were managed using PCV-VG, four with CMV, and four with PRVC. The P-value of 0.4, which exceeds 0.05, indicates that the data are not statistically significant. Among the 18 cases that remained hospitalized for fewer than 10 days, five were placed on CMV, four on CPAP, two each on PCV (PCV-VG) and a mask, and one was placed on PSV and CPAP. Among the 18 patients who remained hospitalized for more than 20 days, eight were administered PCV-VG. This finding is statistically significant, with a P-value of less than 0.05 (0.04) (Table 3).
Distribution of ventilation techniques in relation to specific conditions.
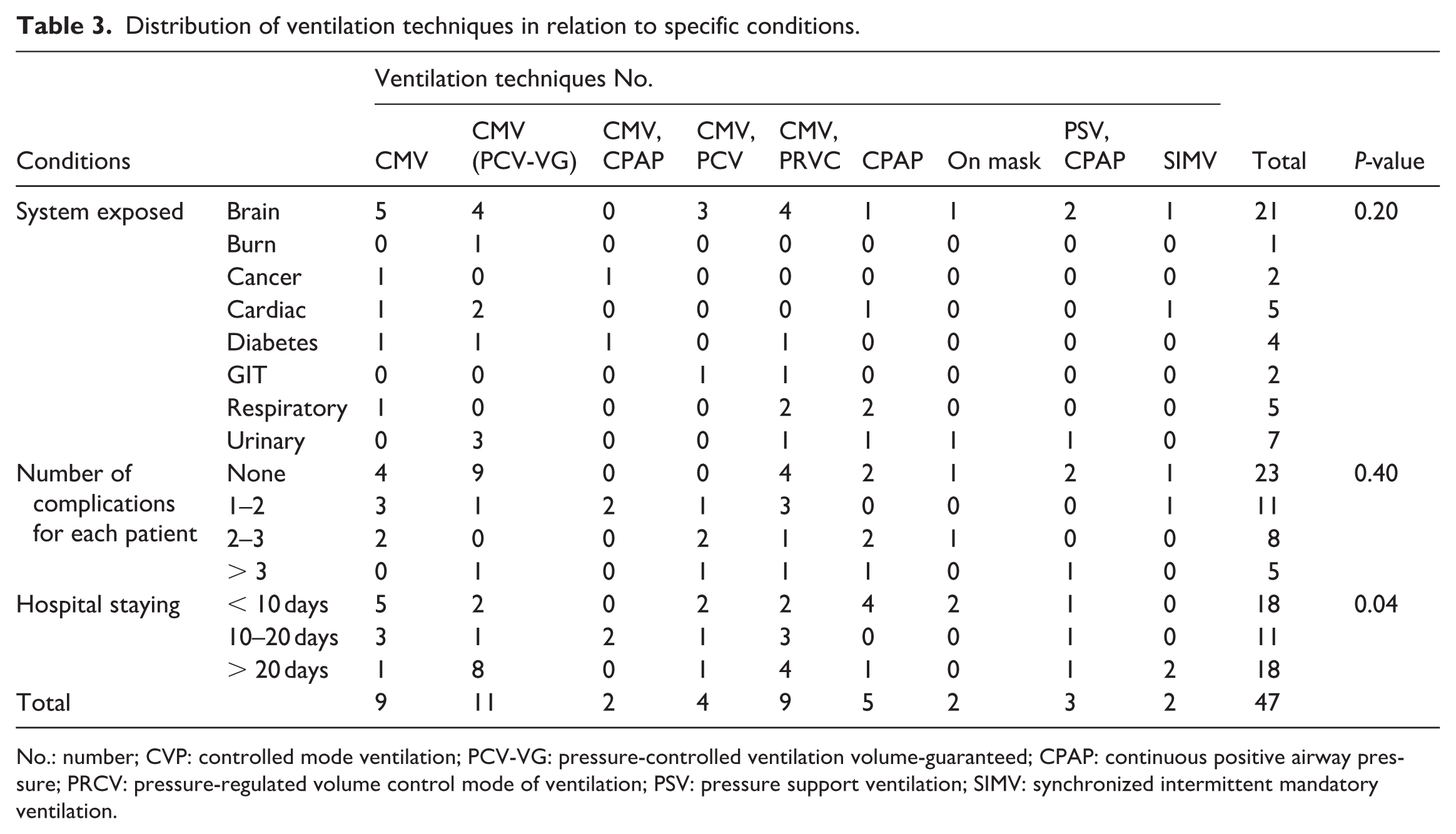
No.: number; CVP: controlled mode ventilation; PCV-VG: pressure-controlled ventilation volume-guaranteed; CPAP: continuous positive airway pressure; PRCV: pressure-regulated volume control mode of ventilation; PSV: pressure support ventilation; SIMV: synchronized intermittent mandatory ventilation.
Fluid balance status
We analyzed the correlation between the average fluid balance over a 7-day period and each patient’s discharge conditions. Patients who deceased (six patients) exhibited a higher mean fluid balance (Figure 3).

Comparison of the mean of total fluid balance with the discharge condition of patients.
Figure 4 presents the total mean fluid balance distribution over the seven follow-up days, classified by the number of complications each patient experienced. Patients without complications exhibit a more balanced fluid ratio. Patients with 1–2 complications demonstrated elevated fluid balance, which has been progressively declining. Patients experiencing 2–3 complications exhibited a low fluid balance that progressively stabilized to a constant state. Patients with more than three complications exhibited a high fluid balance, characterized by intermittent fluctuations between decreased and increased states (Figure 4).

Distributions of mean total fluid balance according to the number of complications presented for each patient.
Figure 5 depicts the correlation between the overall mean of fluid balance over a 7-day follow-up period and systemic factors. Cancer patients exhibited elevated fluid balances that diminished over time. The diabetes and cardiac systems exhibited a more adverse fluid balance status compared to other systems. Urinary cases exhibited the most variable outcomes (Figure 5).

Distributions of mean total fluid balance according to the system exposed.
A multinomial logistic regression analysis was conducted in Table 4 to investigate the relationship between daily fluid balance (Days 1 to 7) and patient discharge outcomes (n = 47). The discharge conditions were classified into three categories: “Cured,” “Partially Cured,” and “Remained,” with “Died” designated as the reference category.
Logistic regression analysis for discharge conditions of patients. (n = 47).
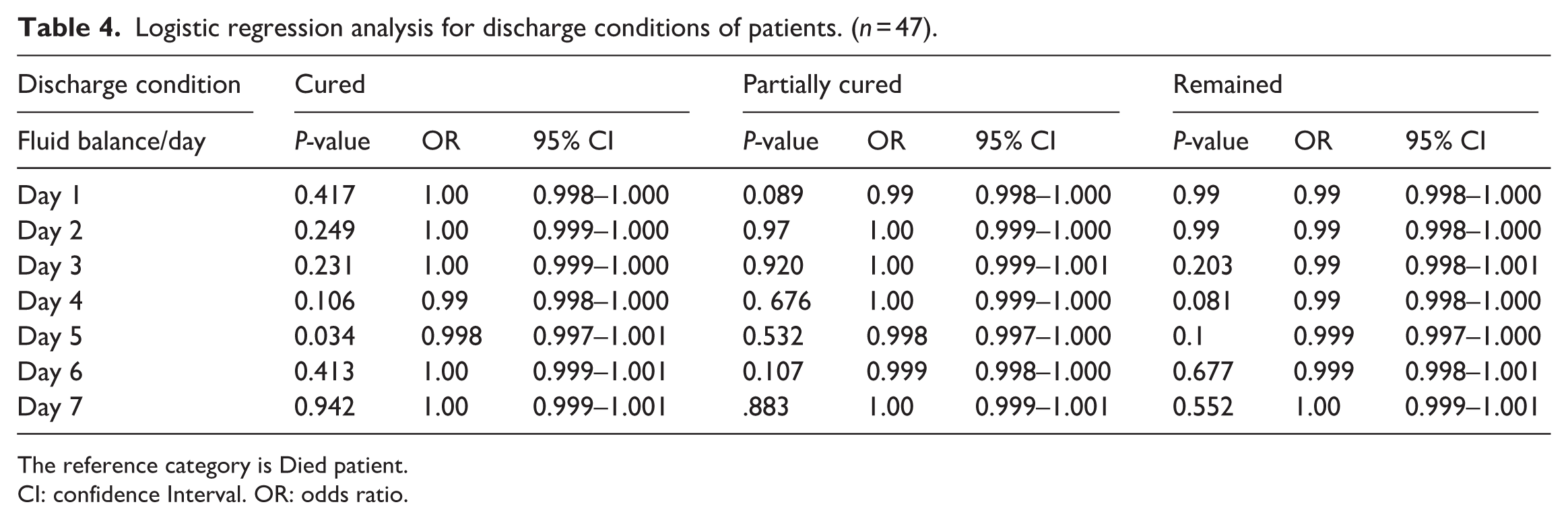
The reference category is Died patient.
CI: confidence Interval. OR: odds ratio.
The analysis indicated that daily fluid balance was typically not a significant predictor of discharge status for most of the observed days. A statistically significant association was noted on Day 5 for the Cured group (P = 0.034). The odds ratio (OR) for Day 5 was 0.998 (95% confidence interval [CI]: 0.997–1.001), suggesting that an increased fluid balance on this day correlated with marginally lower odds of achieving a cure relative to the reference group. No statistically significant relationships were observed between fluid balance and any of the discharge conditions for the remaining days (Days 1, 2, 3, 4, 6, and 7) (P > 0.05). Borderline trends were observed on Day 1 for the “Partially Cured” group (P = 0.089) and on Day 4 for the “Remained” group (P = 0.081); however, these findings did not achieve statistical significance. The ORs for the non-significant days were approximately 1.00, indicating that variations in fluid balance on these days had minimal influence on discharge outcomes within this sample.
Table 5 shows the following illustrations:
Logistic regression analysis for number of complication suspected. (n = 47).

The reference category is patients have >3 complications.
CI: confidence interval; OR: odds ratio.
Overall significance: The analysis indicated no statistically significant relationship between fluid balance and the incidence of complications across all recorded days (Day 1 to Day 7). All P-values were greater than the significance threshold of 0.05.
ORs: Throughout all days and categories, the ORs consistently approached 1.000. This suggests that variations in daily fluid balance did not affect the likelihood of falling into a lower complication category when compared to the reference group (>3 complications).
Day 1: The P-values for the “None,” “1–2,” and “2–3” complication groups were 0.953, 0.425, and 0.600, respectively, with all ORs equal to 1.000.
Day 7: By Day 7, no significant relationship was observed, with P-values between 0.231 (for 1–2 complications) and 0.692 (for none), and ORs consistently at 1.000 or 1.001.
According the result in Table 6:
Logistic regression analysis for system expose of the patients. (n = 47).
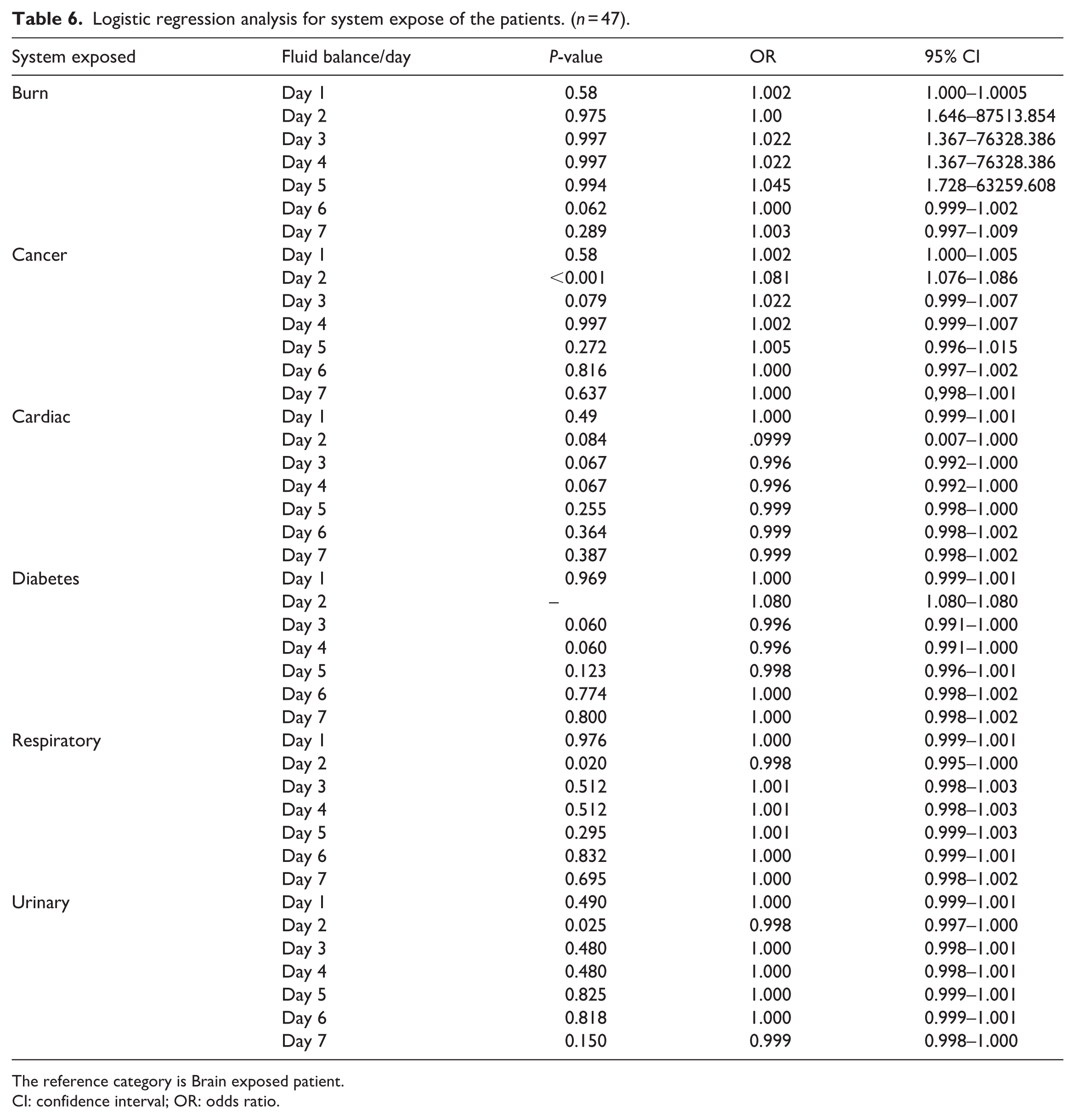
The reference category is Brain exposed patient.
CI: confidence interval; OR: odds ratio.
Cancer system: Fluid balance on Day 2 demonstrated a statistically significant correlation with the Cancer system (P < 0.001). The OR was 1.081 (95% CI: 1.076–1.086), suggesting a marginal increase in the probability of system exposure associated with fluid balance alterations on that day.
Respiratory system: On Day 2, fluid balance demonstrated statistical significance (P = 0.020), with an OR of 0.998 (95% CI: 0.995–1.000). Indicating a slight reduction in the likelihood of system exposure related to fluid balance changes on that day.
Urinary system: The fluid balance on Day 2 demonstrated statistical significance (P = 0.025), with an OR of 0.998 (95% CI: 0.997–1.000). A minor decrease in the probability of system exposure associated with fluid balance alterations on that day is indicated.
Burn system: No days exhibited statistically significant results (P > 0.05). Day 6 exhibited a trend nearing significance (P = 0.062). The CI for Day 2 was extensive (1.646–87,513.854), indicating significant variability or instability in the data for that measurement.
Cardiac system: No days achieved statistical significance. The lowest P-values were recorded on Day 3 and Day 4, both at P = 0.067, with an OR of 0.996.
Diabetes system: No days were recorded with statistical significance. Data from Day 2 revealed an OR of 1.080; however, the source did not provide a calculated P-value. Days 3 and 4 exhibited equivalent outcomes (P = 0.060, OR: 0.996).
Distribution of sepsis
Table 4 illustrates the distribution of sepsis based on specific patient-related factors. Among the eight patients, 7 (87.5%) were male, and those over 60 years of age constituted the majority affected by sepsis (75.5%). Of the patients, 6 (75.05%) experienced ICU stays exceeding 20 days. Urinary tract infection patients and individuals with low fluid balance rates were the most prevalent cases, accounting for 4 (50.0%) and 6 (75%), respectively (Table 7).
Patients’ characteristics associated with the distribution of sepsis (n = 8).

Discussion
This study aimed to evaluate ICU complications and identify those associated with specific body systems. The present study indicates that male patients who are retired and over 60 years of age constitute the majority of individuals admitted to the ICU. Conversely, individuals under the age of 60 were reported less frequently. The identified variables facilitate data analysis and comparison to discern factors associated with ICU complications, suggesting that estrogen may confer a protective effect in critical illness. Estrogen is proposed to provide immune protection following trauma and significant blood loss, as well as in cases of sepsis, while androgens are shown to inhibit immune function. Women experience suboptimal management of acute respiratory distress syndrome compared to men. No consistent differences in sepsis outcomes based on sex have been identified; however, women experience delays in the initiation of antibiotic treatment. Women exhibit a higher incidence of hypoactive delirium in the ICU and demonstrate poorer functional outcomes post-discharge. This aligns with a prior study by Asrat et al. 10 The findings of this study indicate that the higher rate of medical admissions relative to surgical admissions in the ICU can be attributed to various factors. These include medical conditions such as pneumonia, sepsis, and heart failure, which necessitate intensive care characterized by ongoing monitoring and treatment, potentially reflecting the severity of illness. ICU admissions frequently include patients presenting with critical and life-threatening conditions, including septic shock and acute respiratory distress syndrome (ARDS). Critical care may also be necessary during surgical hospitalizations. However, they might not always be as severe or acute as some medical conditions, which could lead to a higher percentage of medical admissions to the ICU. According to system exposure, brain disorders accounted for the majority of admissions, with urinary disorders coming in second. This contradicts the study, which found that respiratory tract infections and cardiovascular disorders were the most common diagnoses that resulted in ICU admission. 11
Patients aged 60 years or older typically have longer hospitalizations in the ICU. They may require prolonged organ support, according to our findings and those of other studies on the association between age group and hospital stay. Overall, mortality rates rose as length of stay increased due to long-term illness, past medical history, or physiological changes, such as a decrease in respiratory capacity (hypoxia, loss of lung elasticity, and decreased muscle strength), which raises the risk of infection, respiratory failure, and ultimately death. 12 According to the study’s findings, patients aged 60 and older spent more time in the ICU, consistent with the idea that age affects ICU outcomes. The majority of patients were released from the ICU, according to the current study’s findings. The majority of the patients in our data are either fully or partially treated and are released. An earlier study conducted in Bangladesh supports this explanation. 13 The majority of patients stayed longer than 20 days, according to the study’s findings. Demographic information, the primary reason for ICU admission, comorbidities, major treatments, and survival status at ICU and hospital discharge were all examined in patients with extended ICU stays. 13 The majority of the participants in the current study had hypertension after taking their PMH, making it the most common prior medical issue. This may be because of poor diet, sedentary lifestyles, tobacco use, and obesity. Diabetes mellitus was the second cause; consequently, the results of an earlier investigation support this conclusion. 14
Regarding the relationship between each patient’s discharge circumstances and the average fluid balance. Fluid balance in the ICU, as assessed upon ICU discharge, was the main exposure. After controlling for indicators of illness severity and long-term medical disorders, positive fluid balance at the time of ICU discharge is linked to a higher risk of death, especially in patients with underlying heart or kidney disease. 10 One of the most common clinical issues in the ICU is fluid and electrolyte imbalance. An earlier study found that among critically sick patients, fluid and electrolyte abnormalities are linked to higher rates of morbidity and death. 15 In summary, daily fluid balance does not seem to be a significant predictor of the number of complications identified in this study.
In critically ill patients, sufficient fluid resuscitation is crucial for restoring cardiac output, systemic blood pressure, and renal perfusion. Fluid overload is associated with heightened mortality and contributes to various complications, including pulmonary oedema, cardiac failure, delayed wound healing, tissue breakdown, and impaired bowel function. Fluid overload is commonly observed in critically ill patients experiencing acute kidney injury (AKI). 16 A negative fluid balance correlated with lower mortality, shorter hospital stays, and higher oxygen saturation. 17
This study aimed to assess the characteristics and outcomes of patients on mechanical ventilation. Mechanical ventilation was primarily indicated for respiratory failure and airway protection. Additional indications encompassed cardiovascular failure (shock) and neuromuscular disease. Patients on ventilators are susceptible to preventable complications, including ventilator-associated pneumonia, pneumothorax, pulmonary embolism, and atelectasis, despite the critical nature of their treatment.
In this study, brain conditions were the primary indication for mechanical ventilation. This finding differed from a study examining the characteristics and outcomes of mechanically ventilated patients in an adult ICU. 18
Our study found that sepsis is more prevalent among male patients compared to female patients. Male sex has been recognized as a potential risk factor for sepsis.19,20 Numerous nationwide and hospital-based epidemiologic studies have indicated a greater prevalence of sepsis among male patients compared to female patients. 21 Most studies indicate that the prevalence of sepsis in male patients ranges from 54% to 66%. 22 Females exhibit superior innate and adaptive immune responses compared to males, enabling more efficient pathogen elimination. 23 Estrogens enhance the humoral immune response in females by directly stimulating the production of immunoglobulins by B lymphocytes. 19
Conversely, testosterone, the primary male sex hormone, has been associated with sex-dependent differences in sepsis. Testosterone exerts significant immunosuppressive effects on both innate and adaptive immunity, resulting in reduced immunoglobulin levels, lymphocyte proliferation, and cytokine production. 21
The prevalence of sepsis is elevated among patients over 60 years of age in the present study. A study found that individuals aged 65 and older accounted for roughly 65% of sepsis cases. 22 The immune system in older adults exhibits aberrations, characterized by immunosenescence. The pathophysiology of immunosenescence is a complex, multifaceted phenomenon. Age-related functional impairments are evident in both cell-mediated and humoral immune responses. 24
This study found that 25% of patients with sepsis had diabetes mellitus. Diabetic individuals exhibit a higher susceptibility to infections, subsequently leading to an increased risk of sepsis development. 25 Elevated blood glucose levels and alterations in the glycaemia-dependent immune response are observed in both type 1 and type 2 diabetes, potentially influencing the pathogenesis and prognosis of sepsis. 26
The present study indicates that 50% of sepsis cases were observed in individuals with urinary tract infections. Urinary tract infections represent a significant contributor to sepsis incidence in hospital settings. 27 The observed result may be attributed to patients necessitating catheterization upon ICU admission. Biofilms are commonly associated with foreign bodies, including catheters and stones. Catheters facilitate bacterial entry into the urinary system, where biofilms can inhibit their elimination. Biofilms typically consist of various microorganisms. 27
Limitations of the study
The financial crisis limits patient access to a single public hospital in Sulaimani city, namely Shar Hospital. Although private hospitals exist in the town, their significantly higher costs restrict patient access, leading to a limited sample size from a single center. This presents a critical issue, leading to unstable estimates and wide CIs because the sample size may not fully represent the broader ICU patient population. Consequently, the findings may not be generalizable to patients admitted outside of the study timeframe or those with different demographic profiles.
Conclusion
The study indicated that the groups at the highest risk for ICU admissions are males and individuals aged over 60 years. Hypertension represents the predominant reason for admission to the ICU. Brain injury is the most prevalent organ exposure in the elderly population. Ventilation techniques are effective and significantly reduce ICU length of stay. Maintaining appropriate fluid balance decreases hospital length of stay and enhances system recovery.
Footnotes
Acknowledgements
We would like to thank all intensive care unit staff at Shar Teaching Hospital for granting permission to collect data, and all patients and other relevant participants who participated in this study.
Author contributions
KJR and HHR conceptualized and designed the study. BIHR performed the literature review and data curation. SMM drafted the manuscript. BIHR revised the manuscript. KJR and HHR supervised the study. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset used in this study is available from the corresponding author upon reasonable request.