
Abstract
Objectives:
Antibiotics have diminished mortality rates associated with bacterial infections. However, their misuse worsens antimicrobial resistance. This study aimed to evaluate antibiotic prescribing patterns using World Health Organization/International Network for Rational Use of Drug prescribing indicators and its determinants at public hospitals in Eastern Tigrai, Ethiopia.
Methods:
A multicenter cross-sectional study was done among encounters prescribed from 1 December 2023 to 30 November 2024 at Doctor Tsegay, Freweyni, and Fre-Semaetat Primary Hospitals. A total of 1800 encounters were selected using systematic random sampling. Data collected from 01 December 2024 to 31 January 2025 were analyzed using SPSS version 21. Binary logistic regression was done to identify determinants of antibiotic prescribing setting statistical significance at p < 0.05. A model fitness test was performed using the Hosmer–Lemeshow goodness-of-fit.
Results:
Antibiotics were prescribed in 65.7% of encounters (1183/1800), totaling 1465 antibiotics. The mean prescribing indicators were 1.24 (Standard deviation 0.48) antibiotics per encounter, and 26.4% of encounters included an injection. Nearly all antibiotics were prescribed from the essential medicine list (99.6%) and by generic name (97.5%). Overall, 67.0% of antibiotics were classified under the “Access” group and 33.0% under the “Watch” group, with none from the “Reserve” group. Factors significantly associated with antibiotic prescribing included being under 18 years of age (adjusted odds ratio = 2.6; 95% confidence interval: 1.54–4.2), receiving ⩾3 drugs (adjusted odds ratio = 7.8; 95% confidence interval: 5.4–11.4), having ⩾2 diseases (adjusted odds ratio = 2.1; 95% confidence interval: 1.27–3.4), and presenting diseases of the genitourinary system (adjusted odds ratio = 9.4; 95% confidence interval: 3.9–22.8).
Conclusion:
Antibiotic prescribing practices were not aligned with World Health Organization standards, indicating substantial overuse. Such patterns may contribute to the worsening of antimicrobial resistance. Strengthening adherence to World Health Organization and national treatment guidelines is essential to promote rational use of antibiotics in these hospitals.
Background
Antibiotics are the cornerstone of modern medicines, which significantly diminished mortality rates associated with bacterial infections. Currently, antibiotics are the most widely prescribed drugs globally.1,2 According to the World Health Organization’s (WHO) report, the worldwide proportion of patients receiving antibiotics was about 30% in 2011. 3 Studies estimated that antibiotics have contributed to the increment of life expectancy of human being by about 23 years. 4 However, indiscriminate use of antibiotics leads to the emergence of antimicrobial resistance (AMR).5,6 The United Nations’ General Assembly High-Level Meeting held in September 2024 declared AMR as a serious world health threat, demanding immediate action to safeguard the world’s ability to treat infectious diseases. 7
Misuse of antibiotics includes use of antibiotics for non-bacterial infections, inadequate dosage of antibiotics, excessive use of antibiotics, use of wrong antibiotics for bacterial infections, and medication error.5,8,9 It is a well-established key driver for AMR 10 and associated with ecological disturbance, economic problems, and re-hospitalization.11,12 Unfortunately, there has been negligible innovation in antibiotics in the last decades 6 as the pharmaceutical companies have divested from antibiotics research to other drugs having higher commercial return. 13 The establishment of antimicrobial stewardship program (ASP) is, therefore, crucial to reduce overuse of the existing antibiotics. 3 Besides, antibiotics should be prescribed by authorized persons with written medico-legal documents to minimize medication errors. 14
Studies indicated that AMR causes hundreds of thousands of deaths every year worldwide. 13 According to recent study, there were about 4.95 million deaths associated with AMR in 2019 worldwide, including 1.27 million deaths directly attributable to AMR. 12 Besides, the Review on AMR estimated that the global burden of deaths from AMR will reach 10 million per year in 2050 unless urgently acted. 13 The World Bank estimated that globally, AMR will result in US$ 1 trillion healthcare costs per year by 2050. 7 Developing countries are disproportionately affected by AMR, 15 which faced substantial increase from 2000 to 2015. 16 Inappropriate use of antimicrobials, poor diagnostics protocols, and high burden of infectious diseases contribute to AMR in developing countries.16,17
Concerned with inappropriate use of medicines, the WHO in collaboration with the International Network for Rational Use of Drugs (WHO/INRUD) developed drug use indicators in 1993. 18 The WHO also introduced the “AWaRe” classification of antibiotics (Access, Watch, and Reserve) in 2017, revised in 2019, 2021, and 2023.19,20 The “AWaRe” classification considers the importance of optimal use of antibiotics and their potential for AMR. 21 The “Access” group includes antibiotics that should be available for common infections. 22 The “Watch” group consists of antibiotics with broader-spectrum activity intended for severe infections, while the “Reserve” antibiotics should only be prescribed as last-resort options.5,22 Despite the prevalent inappropriate use of antibiotics and rapid emergences of AMR, studies on the topic are limited in Tigrai, Ethiopia. Determining the antibiotics utilizing pattern is considered by the WHO as the major indicator for surveillance. The objective of this study was to evaluate antibiotic prescribing patterns using WHO/INRUD prescribing indicators and its determinants at primary public hospitals in Eastern Tigrai, Ethiopia.
Methods
Study setting
Tigrai is a regional state in Ethiopia, with its capital city of Mekelle. The region has seven administrative zones: Eastern zone, Southern zone, Central zone, Western zone, Southeastern zone, Northwest zone, and Mekelle zone. The Ethiopian healthcare system is organized in a three-tier system as primary, secondary, and tertiary levels of care. The primary level of care includes primary hospitals, health centers, and health posts. 23 This study was conducted at three primary public hospitals in Eastern zone of Tigrai, namely Doctor Tsegay Primary Hospital, Freweyni Primary Hospital, and Fre-Semaetat Primary Hospital (FSPH), which are found in Gulomekeda, Tsada Emba, and Hawzien districts, respectively. Unpublished data from the hospitals showed that these hospitals provide different healthcare services collectively for over 418,000 populations. Data were collected from prescription in the central pharmacies of these hospitals. These pharmacies provide both inpatient and outpatient services.
Study design and period
A retrospective multicenter cross-sectional study was conducted from 1 December 2024 to 31 January 2025.
Eligibility criteria
All prescription encounters prescribed for the patients attending at the selected hospitals whose prescriptions were kept in the central pharmacies from 1 December 2023 to 30 November 2024. Prescriptions containing only medical supplies or lacking clear medication names were excluded.
Sampling procedures
The WHO recommends that at least 600 encounters should be included in a cross-sectional study to determine core prescribing indicators in health facility or group of health facilities, with greater number being encouraged. 18 The WHO also recommends reviewing at least 100 prescriptions per health facility to describe or compare drug use by individual facilities and at least 600 prescriptions to describe the overall prescribing practice in group of facilities. 24 Accordingly, in this study, 600 prescription encounters were taken from each hospital from annually written prescriptions. After the prescriptions dispensed in each month were sorted chronologically, a systematic random sampling technique was employed. Then, 50 prescriptions from each month and each hospital were selected to minimize bias due to disease spread and variation in drug availabilities across the year. So, a total of 1800 prescriptions were selected from the three hospitals, from which 1183 prescriptions having antibiotics were included in all analysis.
Operational definitions and outcome measures
The following five WHO/INRUD prescribing indicators were evaluated in this study. 25
Data collection
Data were collected from prescription encounters and prescription registration books. Data abstraction tool adopted from WHO/INRUD prescribing indicators and by reviewing relevant literature was used.26 –29 It was designed to gather information on sociodemographic and patients’ clinical variables (such as sex, age, and the diagnosis) and prescribing indicators such as the number of drugs per encounter, number of drugs prescribed generic name, number of drugs prescribed from EML, presence of antibiotics in encounter, and presence of injection in encounter. The tool also included checklists addressing prescription completeness. It was pretested on 5% of the sample size at Dohan primary hospital (Erob district). Patients’ registration books and medical charts were used to collect missed data from prescriptions (Supplemental material: File 1). The principal investigator gave training to three pharmacists’ data collectors on the objectives of the study and how to collect data. The Ethiopian EML 6th edition was used in measuring medicines prescribed from EML and by generic names. 30 Moreover, the International Classification of Diseases version 10 (ICD-10), 31 and the Anatomical and Therapeutic Chemical classification (ATC) 32 were used to categorize medical conditions and drugs, respectively, for the sake of standardization.
Data entry, analysis, and presentation
Data were entered and analyzed using IBM SPSS version 21. Descriptive statistics were used to summarize sociodemographic characteristics, disease conditions, and prescribing indicators, and are presented as frequencies, percentages, means and standard deviations (SDs), or medians and The Interquartile ranges as appropriate. Associations between independent variables and antibiotic prescribing were assessed using binary logistic regression. Variables with p < 0.25 in the univariable analysis were included in the multivariable model; p < 0.05 was considered statistically significant. Independent variables evaluated included sex, age, number of medicines per encounter, number of diseases per encounter, and ICD-10 disease categories (including the nine most prevalent groups). Results are presented in tables, bar charts, and pie charts.
Results
Sociodemographic and clinical characteristics
In this study, 1800 prescription encounters (600 per hospital) were analyzed. Of these, 51.5% were for female patients. About 54.0% of the prescriptions were for the patients between 18 and 64 years old, with a mean age of 29 (SD 23.51). Moreover, 30.6% of the patients were given ⩾3 drugs, which could be antibiotics and other drug classes (Table 1).
Sociodemographic and clinical characteristics of participants at public hospitals in Tigrai, Ethiopia (n = 1800).

SD: Standard deviation; IQR: Interquartile range.
Infectious and parasitic diseases, diseases of the respiratory system, and diseases of the digestive system were the top three (Table 2). Moreover, out of the 2124 diseases, antibiotics were prescribed for 1196 infectious diseases. Lower respiratory tract infections, gastrointestinal infections, and upper respiratory tract infections together accounted for around half of the total infectious diseases (Figure 1).
Overall prevalence of diseases among participants at public hospitals in Tigrai, Ethiopia (n = 2124).

ICD-10: International Classification of Diseases version 10.
Others*: Diseases of the ear and mastoid process (H60-H95), certain conditions originating in perinatal period (P00–P96).

Infectious diseases for which antibiotics were prescribed among encounters at public hospitals in Tigrai, Ethiopia (n = 1196).
Completeness of prescriptions
Of the prescriptions with antibiotics, overall, patient’s weight (11.0%), address (34.2%), and date of prescription (77.9%) were the least frequently recorded patient-related information. However, diagnosis and patient’s name appeared on 100%. Regarding drug-regimen information, dosage form was the least (11.5%) commonly filled on prescriptions followed by strength of drug (61.8%) and duration of treatment (87.3%). Besides, dispenser’s qualification, prescriber’s qualification, and dispenser’s name was written on 46.3%, 67.3%, and 72.4% of prescriptions, respectively, while prescriber’s signature appeared almost on all (99.2%) prescriptions (Table 3).
Overall prescription completeness among encounters at public hospitals in Tigrai, Ethiopia (n = 1183).

Prescribing indicators
The results of WHO/INRUD prescribing indicators showed that of the 1800 patient encounters, 1465 antibiotics were prescribed in 1183 encounter
WHO/INRUD core prescribing indicators among encounters at public hospitals in Tigrai, Ethiopia (n = 1183).
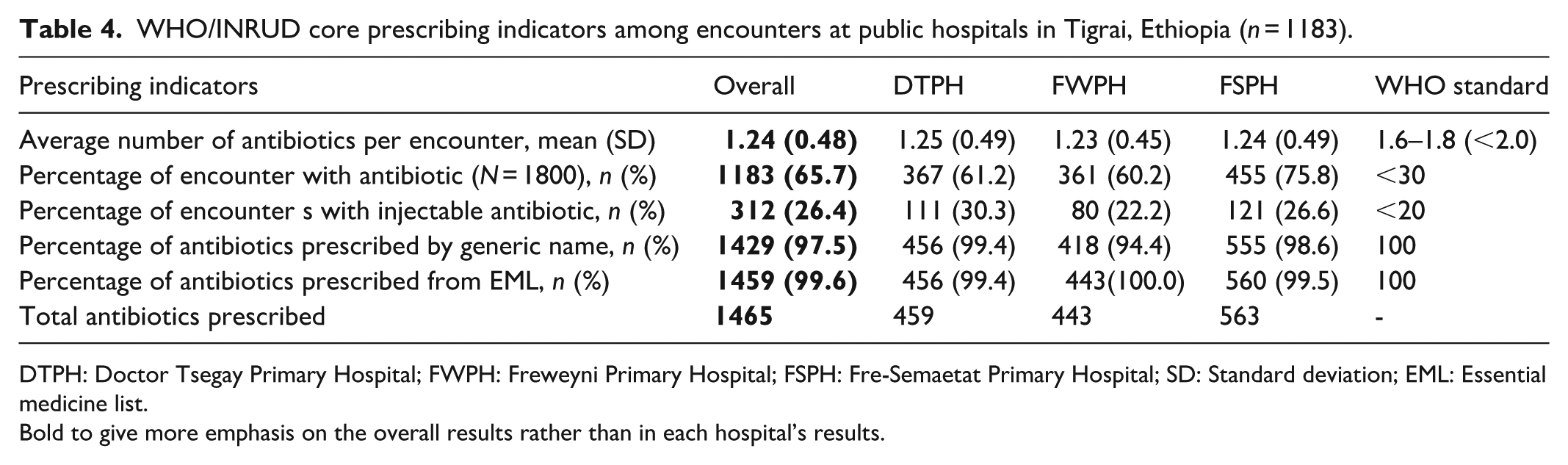
DTPH: Doctor Tsegay Primary Hospital; FWPH: Freweyni Primary Hospital; FSPH: Fre-Semaetat Primary Hospital; SD: Standard deviation; EML: Essential medicine list.
Bold to give more emphasis on the overall results rather than in each hospital’s results.
Patterns of antibiotic prescribing
The distribution of prescribed antibiotics was described using the ATC classification. Accordingly, penicillins (J01C) (42.0%), cephalosporins (J01F) (14.1%), and fluoroquinolones (J01M) (11.4%) were the most frequently prescribed antibiotics classes, collectively accounting for more than two-third (67.5%) of the total antibiotics (Figure 2). Amoxicillin (29.2%), ceftriaxone (11.9%), ciprofloxacin (11.0%), metronidazole (8.8%), and azithromycin (8.7%) were the most frequently prescribed antibiotics at individual drug level. Based on the WHO “AWaRe” classification, 67.0% and 33.0% of the antibiotics fell under the “Access” and “Watch” groups, respectively, but no antibiotic was prescribed from the “Reserve” group. Overall, more than two-third (67.9%) of antibiotics in the “Access” group was covered by amoxicillin, metronidazole, and cloxacillin, while ceftriaxone, ciprofloxacin, and azithromycin accounted for 95.9% of the antibiotics in the “Watch” group. Besides, ceftriaxone alone consisted of 36.0% of the “Watch” group (Table 5).
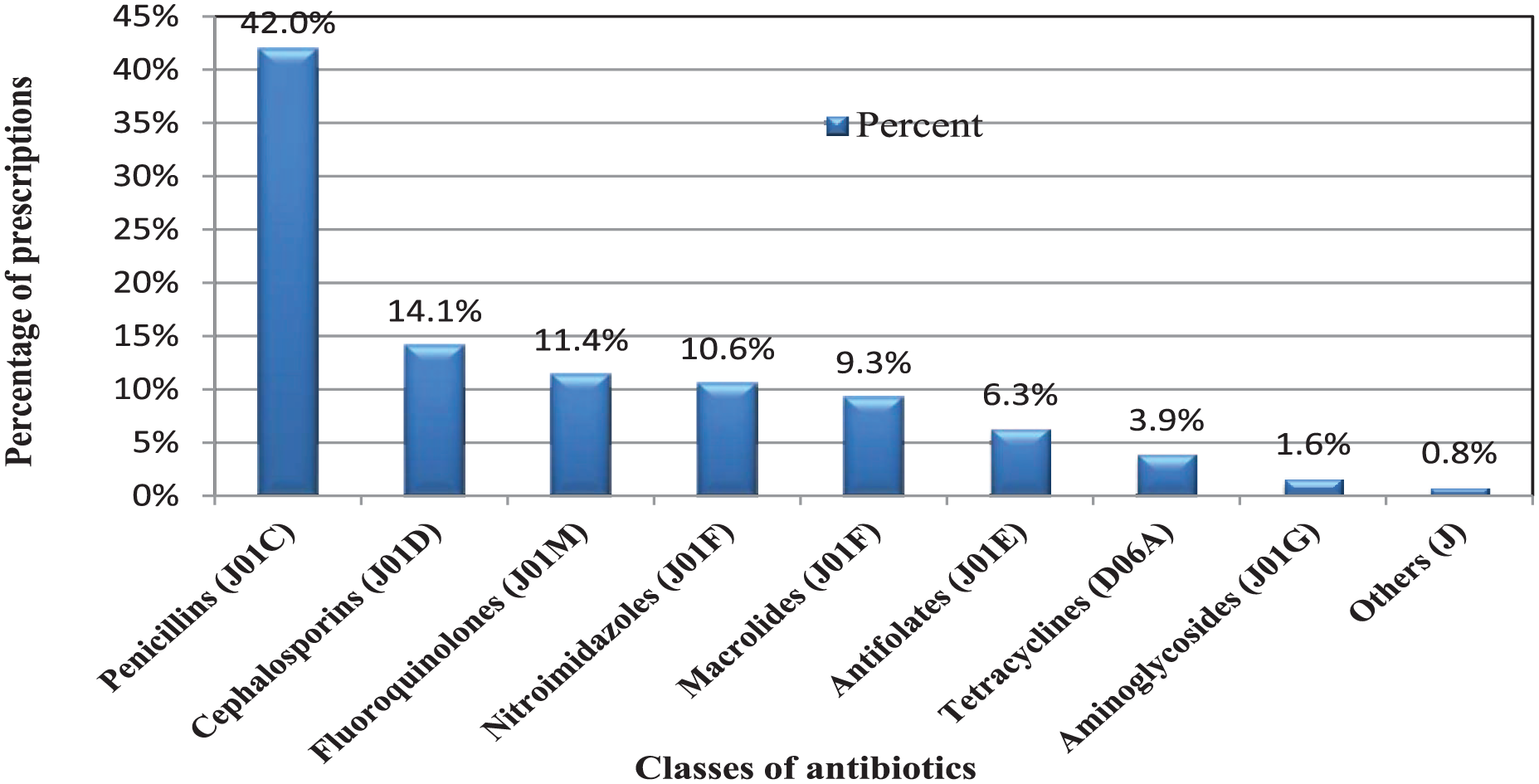
Classes of antibiotics prescribed among encounters at public hospitals in Tigrai, Ethiopia (n = 1465 antibiotics).
Distribution of prescribed antibiotics using the “AWaRe” classification among encounters at public hospitals in Tigrai, Ethiopia (n = 1465).
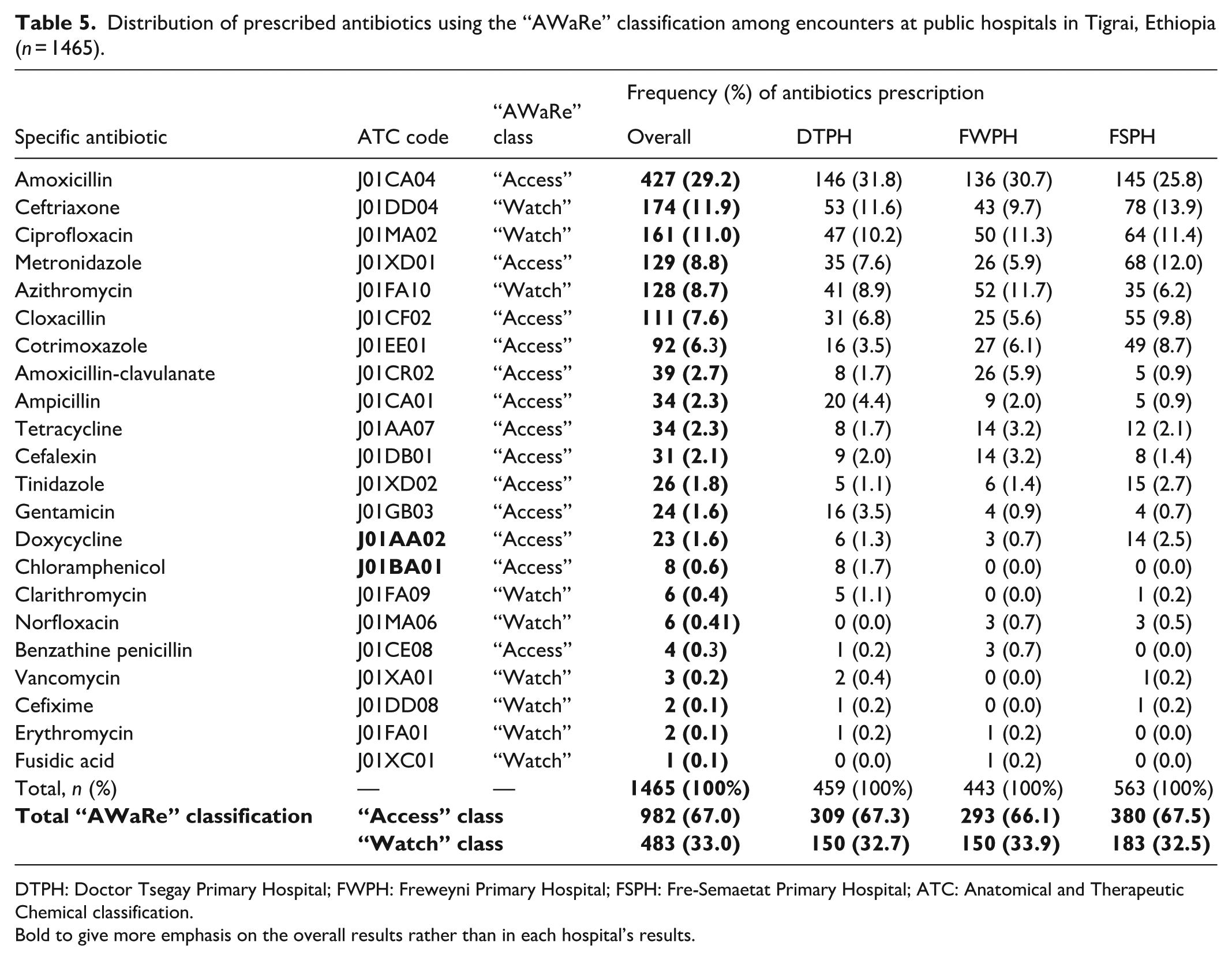
DTPH: Doctor Tsegay Primary Hospital; FWPH: Freweyni Primary Hospital; FSPH: Fre-Semaetat Primary Hospital; ATC: Anatomical and Therapeutic Chemical classification.
Bold to give more emphasis on the overall results rather than in each hospital’s results.
Predictors of antibiotic prescribing
Multicollinearity among predictor variables was assessed using the variance inflation factor (VIF). Values >10 were considered indicative of multicollinearity. All predictor variables presented VIF <10 (mean = 1.26), indicating absence of multicollinearity. A model fitness test was performed to confirm its suitability using the Hosmer–Lemeshow goodness-of-fit. The model was able to distinguish the encounters which had been prescribed antibiotics and those which had not (X2 = 5.79 (df) = 8, p = 0.67]. The p-value > 0.05 indicates the model’s fitness. The model accurately identified 80% of those subjects with antibiotics prescribed and explained between 33.0% (Cox and Snell R squared) and 45.6% (Nagelkerke R squared) of the variance in prescribing antibiotics. The model’s sensitivity test showed that the percentage of encounters with antibiotics, the model had accurately recognized, was 89.3%. Similarly, specificity of the model was 62.2% (Supplemental material: File 2).
On the univariable logistic regression, age, sex, number of diseases per encounter, number of drugs per encounter, diseases of the respiratory system (J00–J99), and diseases of the genitourinary system (N00–N99) were significantly associated with antibiotic prescribing. On the other hand, the presence of infectious and parasitic diseases (A00–B99), diseases of the digestive system (K00–K93), and diseases of the musculoskeletal system (M00–M99) significantly reduced antibiotic prescribing (Table 6).
Predictors of antibiotic prescribing among encounters at public hospitals in Tigrai (n = 1800).

AOR: Adjusted Odds ratio; COR: Crude Odds ratio; Bold values show statistically significant associations; CI: Confidence interval.
In multivariable logistic regression, individuals prescribed with ⩾3 drugs had almost 8 times higher chance to get antibiotics prescription compared to those prescribed with one drug adjusted odds ratio. Similarly, individuals under 18 years old had 2.6 times higher odds of being prescribed antibiotics than those ⩾65 years old. Moreover, having diseases of the genitourinary system and diseases of respiratory system had almost nine and five times likelihood of being prescribed antibiotics, respectively, compared to those without these diseases. The odds of antibiotic prescribing also increased with the number of diseases. However, some of the ICD-10 disease classifications protected antibiotic prescribing. Patients without diseases of musculoskeletal system were about 14 times more likely to have antibiotic compared to patients with this disease. Besides, no diagnosis of endocrine, nutritional and metabolic diseases, and diseases of the circulatory system increased odds of antibiotic prescribing (Table 6).
Discussion
In this study, prescribing patterns of antibiotics was evaluated using WHO/INRUD prescribing indicators. The current findings showed that except diagnosis and patient’s name, completeness of prescription did not meet the standard (100%). 33 More than one-third (35.8%) of the participants in this study were pediatrics. Although patient’s weight and age are crucial in pediatrics to calculate doses, 34 patient’s weight was written on only 11.0% of the prescriptions, which is lower than previous finding (14.3%), 35 but higher than others’ studies (0.9%–2.3%).24,29,35 However, patient’s age was written almost on all (98.1%) prescriptions. Prescription date was written on 77.9% prescriptions, which is lower than the study of Gondar (100%). 33 Dosage form, strength, duration of treatment, and dose were written on 11.5%, 61.8%, 87.3%, and 89.1% of prescriptions, respectively. Unlike our result, all prescriptions had strength, duration, and dosage form of drugs in other study. 36 Moreover, dose was written on 94.2% of prescriptions in other study in Gondar, 33 while other studies reported lower results (27.4%, 30.3%).35,37 Besides, 67.3% of prescriptions had prescriber’s qualification, which is higher than earlier finding (33.0%). 35 The WHO defines the rational use of medicines as “providing patients the right drug; at the right dose; by the right route; for the right duration and at the right cost.” 6 Prescribing medicines against this definition may adversely affect treatment outcomes.
In this study, the overall percentage of encounters with at least one antibiotic was 65.7%. This percentage is more than two times the WHO standard (<30%) and higher than the WHO African regional value, 46%. 25 Moreover, our result was higher than studies done across Ethiopia; Injibara 21.7%, 38 Dire Dawa 27.62%, 39 Gondar 37.5%, 33 Mekelle 32%, 40 and Dessie 44%. 37 Similarly, the present finding was higher than the reports from different parts of the world; 32.9% in Europe, 41 36.6% in India, 42 41.5% in Senegal, 43 and 52.4% in Pakistan. 44 Methodological aspects, such as sample size, number of centers, study design, data collection period, and sample type, could contribute for the differences in antibiotic prescribing. Unlike our study, most of the aforementioned studies included one health facility,18,37 –40,44 with sample size of 344–620. The discrepancy might also be attributed to differences in level of awareness among prescribers, national prescribing guidelines, antibiotic availability, infection control policies, prevalence of infectious diseases, and laboratory setups.
Conversely, our result in the percentage of encounters with at least one antibiotic matched with previous findings reported from India (66%), 45 southern Ethiopia (66.5%), 46 and eastern Ethiopia (66.9%), 39 which could be due to their similarity in terms of multicenter (these studies were conducted in two, three, or four hospitals) and large sample size (these studies used 1440, 2400, or 20,303 patients). However, our finding in antibiotic prescribing was lower than the 89% reported in Ethiopia, 47 88% in Tanzania, 48 83.5% in Nigeria, 49 and 79.1% in Egypt. 50 The relatively low figure in our study compared to these studies may be attributed to study design, sample size, and study setting. The study from Egypt 50 used point prevalence survey approach on 379 inpatients. Moreover, the Ethiopian 47 report was from dentistry, while the Nigerian 49 study was conducted in orthopedics hospital where antibiotics are often used for prophylaxis.
The overuse of antibiotics observed in our study may be attributed to different factors. Diagnostic tests to confirm infectious diseases in developing countries (including Sub-Saharan Africa) are scarce, and the available tests are expensive.13,51 This is true in our context as there are lack of antimicrobial susceptibility tests, microbiological laboratory tests, antibiotics guidelines, and ASPs, which could, in part, be due to long-lasting effects of war crisis in Tigrai, Ethiopia. 52 So, all antibiotics were prescribed empirically based merely on patient’s symptoms, contributing overuse of antibiotics. The overuse of antibiotics may also be accounted for the high burden of infectious diseases . Recent studies showed that infectious diseases remain prevalent in Ethiopia.53,54 Other reasons for the overuse of antibiotics could be the use of antibiotics for viral diseases, 22 cultural beliefs, and view of prescribers on antibiotics. 55 However, the overuse of antibiotics underscores for the responsible use of the existing antibiotics to retard the spread of AMR.
According to the antimicrobial sensitivity studies in Tigrai, Ethiopia, AMR rate is high.56 –59 For instance, antimicrobial susceptibility study indicated that of the total bacterial isolates, 78.6% developed multidrug resistance, and 100% gram-positive and 75% of gram-negative bacterial isolates were found to be multidrug resistant. 59 Besides, similar study conducted among acute diarrheal outpatients in Mekelle hospital, Tigrai showed that Shigella isolates were resistant to ampicillin (100%), amoxicillin (86.7%), and cotrimoxazole (66.6%), while low resistance was observed to ciprofloxacin (6.7%), norfloxacin (6.7%), and gentamicin (13.3%). Overall, 80% of the isolates showed multidrug resistance. 56 All these findings call for clinicians for the critical use of antibiotics in our setups to safeguard the existing antibiotics. Adherence to national and WHO standard treatment guidelines may also be paramount to prevent the overuse of antibiotics and retard further spread of AMR.
Penicillins (42.0%), cephalosporins (14.1%), and fluoroquinolones (11.4%) were the most frequently prescribed antibiotics classes. Prescribed alone, 69.6% was covered by five antibiotics: amoxicillin (29.2%), ceftriaxone (11.9%), ciprofloxacin (11.0%), metronidazole (8.8%), and azithromycin (8.7%). This is consistent with findings of European countries 41 where penicillins, cephalosporins, and fluoroquinolones were the most common antibiotics used. Likewise, penicillins were most prescribed antibiotics in Ethiopia (32.69–51.9%)24,60,61 and other settings (34.1%–43.3%).27,50 Inconsistent with our findings, cephalosporins ranked the first in earlier study. 44 Amoxicillin was the most commonly prescribed antibiotic in Ethiopian studies,37,39,61,62 which agrees with our study. However, ceftriaxone,2,44 metronidazole, 48 and ciprofloxacin 60 ranked first most prescribed antibiotics in some studies. The higher ceftriaxone usage could be explained by the fact that these studies assessed inpatients only where injectable antibiotics are common, while we included outpatients and inpatients. The overuse of few types of antibiotics observed in our study may worsen the emergence of AMR to these antibiotics.
The United Nations General Assembly recommends that the “Access” antibiotics should cover ⩾70% of all antibiotics uses. 7 The “Access” antibiotics have narrow spectrum of activity and lower potential for AMR.19,21 However, the “Watch” antibiotics have higher potential for AMR, and should be used in confirmed infections. 63 In the present study, 67.0% of antibiotics were prescribed from the “Access” group, which is lower than the standard, ⩾70%. Besides, the “Watch” group accounted for 33% of antibiotics, whereas no antibiotic was prescribed from the “Reserve” group. Amoxicillin, metronidazole, and cloxacillin covered 67.9% in the “Access” antibiotics, while ceftriaxone, ciprofloxacin, and azithromycin consisted of 95.9% in the “Watch” group. Unlike to our result, higher use of the “Access” antibiotics was reported in Ethiopia (79.4%) 24 and Eritrea (71.9%). 62 Conversely, some studies showed higher prescription of the “Watch” antibiotics (41.70–50.69%).50,60,61 Although the “Access” antibiotics use deviated from WHO standard (⩾70%) in our study, it should be encouraged. However, the overuse of ceftriaxone, ciprofloxacin, and azithromycin from the “Watch” group needs special attention. The “no” usage of the “Reserve” antibiotics in our study may be attributed to nonavailability due to their expensiveness.
In this study, the average number of antibiotics per patient was 1.24 (SD = 0.48), which fell within the WHO standard value of <2.0. 18 Nevertheless, drugs other than antibiotics were not analyzed as this was not the aim of this study, which needs careful interpretation. This finding was lower than that of similar studies from Tanzania, 48 northwest Ethiopia, 2 Egypt, 50 and north Ethiopia 26 (1.53–2.01). However, the current finding was higher than similar study conducted in Addis Ababa, which was 1.10. 24 The lower the number of drugs prescribed per patient, the more rational prescribing patterns being practiced. 2 Moreover, increasing number of drugs is associated with drug interactions and other adverse drug reactions, 26 and thus, prescribers should limit the number of drugs they prescribe.
The WHO gives special emphasis on the rational use of injections as they are important, but commonly overused and costly forms of drugs. 23 In the present study, overall, 26.4% of encounters were prescribed injectable antibiotic, a value higher than WHO’s standard (13.4–24.1%). In contrast, studies done in Ethiopia reported lower values28,38,41 (3.1–13.9%), while higher values were reported: 46% from South Africa, 27 84.8% Ethiopia 26 and 98.6% Egypt. 50 The studies with higher injection rates assessed only inpatients where injections are reasonably high, which may be one reason for the discrepancies. The overuse of injections increases the risk of transmission of hepatitis-B, human immunodeficiency virus, and other iatrogenic infections.39,61 Furthermore, injectable medicines are more expensive than the equivalent oral preparations, which cause wastage of resources. 29
Generic prescribing reduces chance of drug duplication as patients may use one drug prescribed in brand and generic names. 2 Besides, generic prescribing enables the substitution of therapeutic equivalents. Generic drugs are relatively accessible and less expensive compared to brand drugs.39,61,62 In this study, the percentage of antibiotics prescribed by generic name was 97.5%, which approached the WHO standard value of 100%. Lower percentages than our result were reported in some studies (19–83%).28,42 –44,46 The WHO recommends prescribers to follow the EML as medicines on this list have good quality, safety, and efficacy. In the present study, almost all (99.6%) the antibiotics were prescribed from the Ethiopian EML, which fell almost within WHO’s standard, 100%. 18 Almost consistent with this finding, previous studies from Ethiopia reported that all medicines were prescribed from the EML.2,41 The relatively higher antibiotic prescribing rates from the EML and by generic name in our study might be attributed to the centralized procurement policy of Ethiopia where the Pharmaceutical Supply Agency of the country provides drugs to public hospitals from EML by their generic name. This practice is, hence, quite promising which needs further enforcement.
This study showed strong association between antibiotic prescribing and patients’ age. Thus, subjects under 18 years old had about 2.6 times higher probability of receiving antibiotics than those ⩾65 years old. Agreeing with this, a study from Eritrea 62 showed that increasing age decreased the likelihood of prescribing antibiotics significantly. Conversely, sex did not show significant association with antibiotic prescribing in our study. However, age was not predictor of antibiotic prescribing in Poland, 4 while sex was predictor in other study, 64 all disagreeing with our finding. The higher antibiotics use in children in our study could rise (partly) from the high burden of respiratory tract infections in children in Tigrai. 54 Beyond AMR, children are susceptible for various medication errors, 65 and adverse drug reactions as developmental changes affect responses to drugs. 34 So, prescribers should be cautious when prescribing antibiotics to pediatrics. Besides, prescribing antibiotics was significantly associated with the number of drugs per prescription. Individuals prescribed with ⩾3 drugs had almost 8 times higher chance of being prescribed with antibiotics compared to those prescribed with one drug, which is in line with previous study. 34
In the current study, individuals having diseases of the genitourinary system and diseases of respiratory system had about nine and five times higher chance of being prescribed antibiotics, respectively, compared to those without these diseases. Consistent with this, studies done in Ghana 55 and Tigrai, Ethiopia 61 showed that subjects with respiratory tract infection had increased odds of antibiotic prescribing compared to those without this disease. In the current study, upper respiratory tract infection was the third most common disease for which antibiotics were prescribed. So, antibiotics might have been inappropriately prescribed for self-limiting conditions like acute otitis media, acute sinusitis, and bronchitis. 20 However; some of the disease protected antibiotic prescribing in our study. Accordingly, patients without diseases of musculoskeletal system were about 14 times more likely to be prescribed antibiotic compared to those having the disease. Besides, no diagnosis of endocrine, nutritional and metabolic diseases, and diseases of the circulatory system increased odds of antibiotic prescribing.
The current trends of the inappropriate use of antibiotics in the study setting is concerning. To address the problem associated with the misuse of antibiotics, the WHO “AWaRe” and the WHO/INRUD guidelines should be enforced tailored to local clinical needs. The government bodies and hospital administrators should promote the laboratory infrastructures and diagnostic protocols to perform microbiological test, microbial culture, and antimicrobial sensitivity test to confirm infectious diseases and to choose the right antibiotics. This turn will help to reduce empirical and overuse of antibiotics, and to contain the spread of AMR. Revitalization of the war-ruined healthcare system in Tigrai should be the primary interventions of the Regional and Federal governments of Ethiopia to promote rational prescribing practices of antibiotics.
Strengths and limitations of the study
This study has a number of strengths. This is the first study conducted to evaluate patterns of antibiotic prescribing and its determinants at public hospitals in Tigrai, Ethiopia. The study was a multicenter study with a large sample size, three times the minimum sample size recommended by the WHO. However, the study has some limitations. First, since data were gathered retrospectively, we might have missed unrecorded data. Second, this study assessed only prescribing indicators, leaving patient care and healthcare facility indicators untouched. Third, only antibiotic medications were analyzed. Nevertheless, the current study provided some insights into the patterns, prevalence, and predictors of antibiotic prescribing at public hospitals in Tigrai.
Conclusion
The present study revealed that antibiotic prescribing patterns deviated from the WHO recommendations. The percentage of encounters with antibiotic prescribed was more than twice the WHO standard value. Besides, antibiotic prescription from the “Access” group was lower than WHO optimal value. This overuse of antibiotics in general and antibiotics from the “Watch” group in particular may aggravate AMR against these antibiotics. Therefore, the observed high antibiotic prescribing rate is concerning and underscores the urgent targeted interventions to tackle the spread of AMR. Moreover, the clinicians working herein these hospitals should focus on evidence-based prescribing practice of antibiotics and follow the WHO and National Treatment Guidelines to achieve the WHO/INRUD recommendations on prescribing indicators. The public should be aware that antibiotics have to be used only when they are absolutely required by the medical conditions, and be aware of the deleterious effects of the inappropriate use of antibiotics.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261426850 – Supplemental material for Antibiotic prescribing patterns using World Health Organization/International Network for Rational Use of Drug prescribing indicators and its determinants in Eastern Tigrai, Ethiopia: A need for antimicrobial stewardship programs
Supplemental material, sj-docx-1-smo-10.1177_20503121261426850 for Antibiotic prescribing patterns using World Health Organization/International Network for Rational Use of Drug prescribing indicators and its determinants in Eastern Tigrai, Ethiopia: A need for antimicrobial stewardship programs by Gebretekle Gebremichael Hailesilase, Haylay Araya Gebrezgabiher, Brhane Gebrehiwot Welegebrial and Abrahaley Mulu Kidane in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121261426850 – Supplemental material for Antibiotic prescribing patterns using World Health Organization/International Network for Rational Use of Drug prescribing indicators and its determinants in Eastern Tigrai, Ethiopia: A need for antimicrobial stewardship programs
Supplemental material, sj-pdf-2-smo-10.1177_20503121261426850 for Antibiotic prescribing patterns using World Health Organization/International Network for Rational Use of Drug prescribing indicators and its determinants in Eastern Tigrai, Ethiopia: A need for antimicrobial stewardship programs by Gebretekle Gebremichael Hailesilase, Haylay Araya Gebrezgabiher, Brhane Gebrehiwot Welegebrial and Abrahaley Mulu Kidane in SAGE Open Medicine
Footnotes
Acknowledgements
The authors are thankful to the respective administrators and pharmacy staffs of Doctor Tsegay Primary Hospital, Freweyni Primary Hospital, and Fre-Semaetat Primary Hospital for their valuable contributions during data collection process.
Ethical considerations
Ethical clearance was obtained from the Research Ethics Committee of the Research and Community Service Office of Adigrat University College of Medicine and Health Sciences (reference number ADU.CMHS/RCS/027/17). Permission was then obtained from the respective hospital administrators of Doctor Tsegay Primary Hospital, Freweyni Primary Hospital, and Fre-Semaetat Primary Hospital before commencing the study.
Consent to participate
Informed consent was not obtained from patients since this is retrospective cross-sectional study where secondary data were gathered from drug prescription papers after the patients had been discharged. Nevertheless, written informed consent was waived by the Research Ethics Committee of Adigrat University. Thus, confidentiality of patients was secured accordingly where data were anonymously used.
Author contributions
G.G.H. conceptualized the study. H.A.G. and B.G.W. drafted and developed research methodology of the study. G.G.H., B.G.W. and H.A.G. collected the data. A.M.K., B.G.W. and H.A.G. performed the statistical analysis. G.G.H. prepared the manuscript. All authors read and approved final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used to support findings of this study are available from the corresponding author upon reasonable requests from concerned body.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.