
Abstract
Objective:
This study aimed to evaluate the prevalence, location, and morphometric characteristics of the alveolar antral artery in an Iranian population using cone-beam computed tomography.
Materials and methods:
A retrospective analysis was conducted on cone-beam computed tomography images of 322 patients acquired at Shiraz University of Medical Sciences between January 2015 and December 2022. The alveolar antral artery canal presence, mediolateral position (intrasinus, intraosseous, superficial), mediolateral coarse, and morphometry (distances to sinus floor and alveolar crest at the premolar and molar site, and diameter) were assessed. Statistical analysis was performed to identify significant differences based on age, gender, dental status, and side (p < 0.05).
Results:
The overall prevalence of the alveolar antral artery was 92.2%, most commonly in an intrasinus position (51.3%). The most frequent course was the “in” type (32.4%). Median distances to the sinus floor ranged from 5.09 mm (first premolar) to 7.30 mm (second molar), while distances to the alveolar crest from 16.70 mm (second molar) to 24.65 mm (first premolar). Significant variations in alveolar antral artery canal dimensions and distances were observed based on tooth location, gender, age, and dental status.
Conclusion:
This study demonstrates a high prevalence and significant anatomical variability of the alveolar antral artery canal in the Iranian population, and underscores the importance of preoperative cone-beam computed tomography imaging to minimize the risk of iatrogenic injury during posterior maxillary surgeries.
Introduction
The posterior region of the maxilla presents a complex anatomical structure, including various vessels forming a plexiform network responsible for blood supply to the posterior muscles, teeth, and bones of the upper jaw. The alveolar antral artery (AAA) represents a critical anastomosis between the posterior superior alveolar artery (PSAA) and the infraorbital artery. It is located at the anterolateral wall of the maxillary sinus which supplies blood to the Schneiderian membrane, sinus wall, and periosteum.1,2 The AAA is the intraosseous branch or anastomosis of the PSAA and infraorbital artery, which appears on cone-beam computed tomography (CBCT) images as a bony canal in the lateral wall of the maxillary sinus. The clinical importance of the AAA stems from the potential complications associated with its iatrogenic injury during various dental and maxillofacial procedures. Surgical interventions such as sinus lift operations, Lefort I osteotomies, and dental implant placements in the posterior maxilla can lead to inadvertent damage to the AAA canal, resulting in significant hemorrhage that compromises visibility during the procedure and potentially leads to postoperative complications. 1 This risk highlights the necessity for thorough pre-surgical planning with appropriate imaging techniques to identify and avoid this important vascular structure.3–5
CBCT has emerged as the gold standard for evaluating maxillofacial structures, particularly the maxillary sinuses. The technology’s high spatial resolution, absence of superimposition effects, and ability to generate three-dimensional models for volumetric analysis make it exceptionally suitable for assessing small vascular structures like the AAA canal. 6 Previous research has established that CBCT provides superior visualization of the AAA canal compared to other imaging modalities, enabling precise measurement of its location, and diameter along with assessment of the height and width of the alveolar ridge.7–9
While several studies have investigated the anatomical properties of the AAA across various populations,10–15 a comprehensive analysis of its features stratified by demographic factors remained lacking. A recent scoping review highlighted the growing demand for anatomically precise, image-based investigations that directly inform clinical decision-making. 16 This research gap prompted the current investigation, which aimed to comprehensively analyze the presence, location, and morphometric features of the AAA stratified by sex, side, age, and dental status. The study provides valuable measurements of the distances from the AAA canal to the maxillary sinus floor and alveolar crest across all the maxillary premolar and molar locations, contributing essential insights for surgical planning involving the posterior maxillary region.
Materials and methods
This descriptive, retrospective, observational cross-sectional study was conducted at the Oral and Maxillofacial Radiology department of Shiraz University of Medical Sciences in Iran. For a CBCT-based study evaluating the AAA, a sample size of 200–400 patients were considered appropriate by the existing literature and statistical calculation. The CBCT studies of 322 patients were assessed based on a retrospective review of all the eligible CBCT scans obtained at Shiraz University of Medical Sciences between January 2015 and December 2022. The study protocol was approved by the Institutional Review Board of Shiraz University of Medical Sciences (IR.SUMS.DENTAL.REC.1401.047) and complied with the ethical standards of the Declaration of Helsinki, and relevant informed consent forms were signed by patients or legally authorized representatives.
The CBCT images were obtained, using a flat panel detector scanner (NewTom VGi; QR s.r.l., Verona, Italy). All the images were acquired within a total exposure time of 1.8 s at 110 kVp, using a field of view of at least 15 × 12 cm2; the electrical current (mA) was adjusted automatically for each patient. All the CBCT images were obtained in a standardized head posture (the Frankfurt plane parallel to the floor). The CBCT images were reviewed in NNT viewer version 8.0. Voxel size was maintained at 0.3 mm, with corresponding slice and inter-slice thicknesses to optimize resolution for detecting small anatomical structures such as the AAA canal. CBCT images were viewed and reported in a dimly lit, quiet room, using a medical grade diagnostic display device (Barco monitor, Model: MDRS-2122; Belgium). CBCT images were reconstructed and analyzed in the coronal plane.
Subject selection focused on patients with permanent dentition who had received CBCT imaging of the posterior maxillary region from the first premolar to the second molar for various dental treatment purposes. Demographic data including age and gender were collected for all the subjects. The age range of subjects was from 15 to 70 years. An important inclusion criterion was the availability of bilateral maxillary scans suitable for comprehensive investigation.
To maintain the integrity of the analysis, several exclusion criteria were established. These included any conditions that could compromise visualization of the maxillary sinus wall in either side of the posterior maxillary region, such as pathologic conditions (cysts or tumors, sinusitis), previous trauma or surgery, and severe pneumatization in edentulous areas. Additionally, individuals with congenital anomalies associated with the maxillary bone that might interfere with image interpretation were excluded from the study.
The assessment of CBCT scans was conducted by two independent examiners—a senior dental student and an oral and maxillofacial radiologist—to identify the AAA canal. Both examiners were calibrated through a pre-assessment of 30 random scans. Interobserver agreement was measured using Cohen’s kappa (κ = 0.88), indicating high reliability. Discrepancies greater than 0.5 mm were re-evaluated, and consensus was achieved through joint discussion. The measurements were performed on coronal sections and included two primary distance measurements: the perpendicular distance from the inferior border of the AAA canal to the maxillary sinus floor (Distance a), and the perpendicular distance from the inferior border of the AAA canal to the alveolar crest (Distance b; Figure 1). 1

(a) Distance from the AAA to the maxillary sinus floor, (b) distance from the AAA canal to the alveolar crest, and (c) AAA diameter.
For edentulous areas, adjacent or contralateral teeth served as anatomical landmarks to identify the corresponding tooth location. The researchers utilized the same distance from the midline to identify corresponding locations on the opposite side. Measurements were taken from slices intersecting the center of each tooth. For age-related analyses, patients were categorized into four distinct groups: under 20 years, 20–39 years, 40–59 years, and 60 years or older. The mediolateral position of the AAA canal according to the location to each tooth was classified as intrasinus (beneath the sinus membrane at the lateral sinus wall), intraosseous (within the lateral sinus wall), or superficial (beneath the outset layer of the bone at the lateral sinus wall; Figure 2).

(a) AAA is located at the inner sinus wall, (b) AAA is located within the sinus wall, and (c) AAA is located at the outer sinus wall.
The mediolateral course of the AAA canal, at the level of the second molar to the first premolar, was categorized into six types: in (canal located at the inner sinus wall at all the tooth locations); middle (canal located within the sinus wall at all the tooth locations); out (canal located at the outer sinus wall at all the tooth locations); through (canal crossing the sinus wall during its course); in or out to middle (canal at the inner or outer wall at the second molar, gradually transitioning to within the sinus wall); and middle to in or out (canal within the sinus wall at the second molar, gradually transitioning to the inner or outer wall; Figure 3).
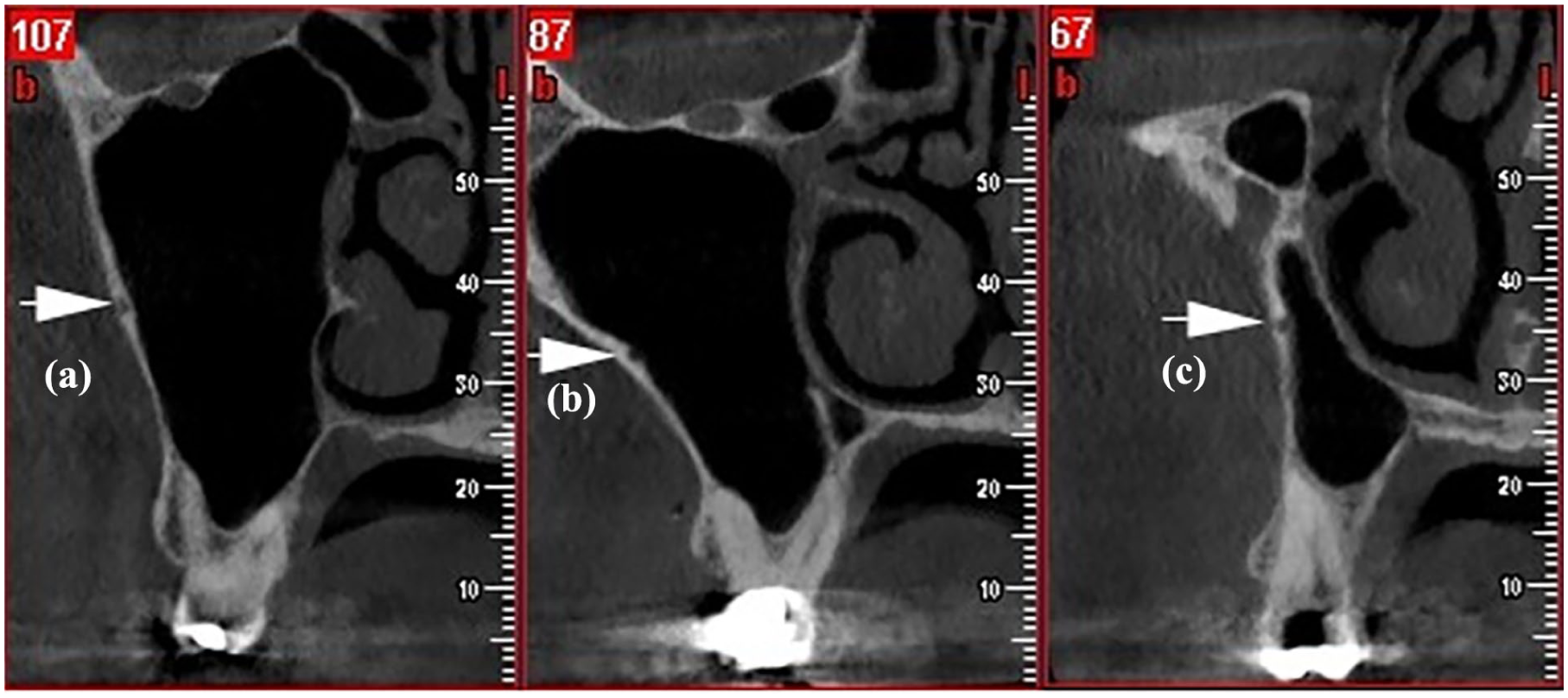
The mediolateral trajectory of the AAA canal from the second molar (a) to the first molar (b) and then to the second premolar (c) gradually shifts from the middle sinus wall toward the inner sinus wall and back toward the middle wall.
The primary outcome parameters were the distances between the AAA canal and the maxillary sinus floor and alveolar crest. Secondary outcomes included the prevalence, diameter, mediolateral position, and course of the AAA canal, and their respective comparisons across age groups, sides, and genders.
Statistical analysis
Descriptive statistics were initially calculated. Homogeneity of variance was assessed using Levene’s test. NCSS version 15.0 (SPSS Inc., Chicago, IL, USA) was used for all the statistical analyses. Continuous variables were compared using one-way ANOVA. The Mann–Whitney U and Kruskal–Wallis tests were employed for other variables. Independent t-tests were used to determine statistically significant differences (p < 0.05) in median and interquartile range (IQR) AAA canal distances from the alveolar crest and sinus floor, categorized by tooth location, age, gender, side, and dental status.
Results
The comprehensive analysis of 322 CBCT images revealed significant findings regarding the prevalence and anatomical characteristics of the AAA in the Iranian population. The overall detection rate of the AAA canal using CBCT imaging was notably high at 92.2%, demonstrating the ubiquitous nature of this vascular structure in the study population. A slight gender difference was observed, with males showing a marginally higher prevalence (94.7%, mean age 34.5 years) compared to females (91.9%, mean age 39.7 years).
Due to the non-normal distribution of data as determined by Levene’s test, the study appropriately utilized median and IQR values for distance measurements rather than means and standard deviations.
The median distance from the AAA canal to the sinus floor, designated as distance A, demonstrated a progressive increase from anterior to posterior regions. At the first premolar, this distance measured 5.09 mm (IQR: 2.49), increasing to 5.82 mm (IQR: 2.04) at the second premolar, 6.67 mm (IQR: 2.15) at the first molar, and reaching 7.30 mm (IQR: 2.39) at the second molar. Statistical analysis confirmed significant differences between the premolar and molar regions in this measurement (Table 1). Conversely, the measurements of distance B, representing the perpendicular distance from the inferior border of the AAA canal to the alveolar crest, exhibited an opposite trend. The median values decreased progressively from anterior to posterior: 24.65 mm (IQR: 6.13) at the first premolar, 20.38 mm (IQR: 3.39) at the second premolar, 17.62 mm (IQR: 2.80) at the first molar, and 16.70 mm (IQR: 3.10) at the second molar. Again, significant variations were observed between premolar and molar regions.
Comparison of the parameters by gender and side.

AAA: alveolar antral artery.
Distance A: distances from the AAA canal to the maxillary sinus floor (mm); Distance B: distances from the AAA canal to the alveolar crest (mm).
The diameter of the AAA canal represents another important morphometric parameter. The study found a mean diameter of 1.20 mm with a standard deviation of 0.42 mm, and a range from 0.3 to 3.00 mm. Analysis of diameter frequency distribution revealed that the majority of canals (71.8%) measured between less than 1 mm and less than 1.5 mm, with 34.6% measuring less than 1 mm and 37.2% between 1 and less than 1.5 mm. Larger diameters were less common, with 24.1% measuring between 1.5 and less than 2 mm, and only 4% measuring 2 mm or greater. 1 These findings indicate that while most AAA canals are of moderate size, a significant proportion are larger than 1.5 mm in diameter.
Gender-based differences were observed across multiple parameters of the AAA canal. Significant variations between males and females were found in the distance from the canal to the sinus floor at the first molar (p = 0.001) and second molar (p = 0.016), as well as in the distance to the alveolar crest at the first molar (p = 0.047). Additionally, the AAA canal diameter showed a statistically significant gender difference (p = 0.008), with males having larger mean diameters (1.24 mm, SD: 0.40) compared to females (1.16 mm, SD: 0.42; Table 1).
Age-related variations were another significant factor influencing AAA canal characteristics. The study categorized patients into four age groups (<20, 20–39, 40–59, and ⩾60 years) and identified notable differences across these cohorts. Specifically, differences in the distance to the sinus floor were observed at the second premolar and molar regions, particularly between the 20–39 and ⩾60 age groups (p < 0.001). Similar age-related variations were evident in the distance to the alveolar crest at the first molar between these same age groups (p = 0.042). The AAA canal diameter also demonstrated significant differences across age groups (p = 0.002), with particular distinctions between the 40 and 59 age groups and both the <20 (p = 0.002) and 20–39 (p = 0.017) age groups (Table 2).
Comparison of the parameters by age and dental status.
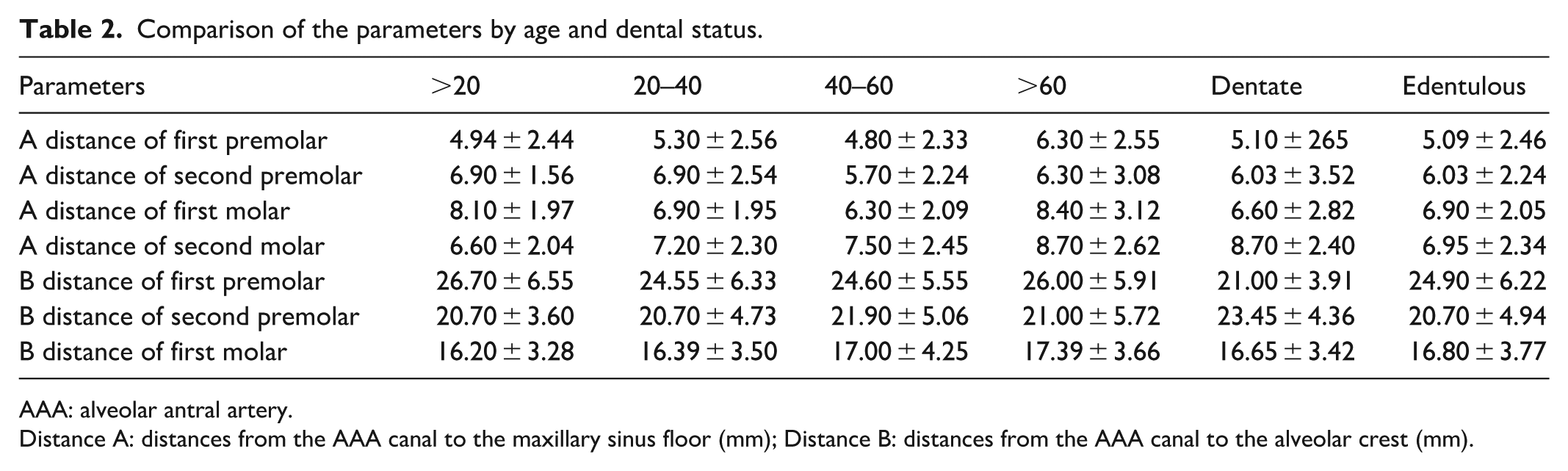
AAA: alveolar antral artery.
Distance A: distances from the AAA canal to the maxillary sinus floor (mm); Distance B: distances from the AAA canal to the alveolar crest (mm).
Regarding laterality, the study found minimal differences between right and left sides, with the only statistically significant variation observed in the distance from the AAA canal to the alveolar crest at the first premolar (p = 0.021), where the right side exhibited a longer distance (Table 1).
Dental status emerged as another influential factor affecting AAA canal measurements. The study revealed a significant difference in the distance to the sinus floor at the second molar between dentate and edentulous patients (Table 2).
The positional characteristics of the AAA canal demonstrated considerable variability, with the most common mediolateral position being intrasinus, accounting for 51.3% of cases. This designation refers to the canal’s location beneath the sinus membrane at the lateral sinus wall. The second most prevalent position was intraosseous (42.5%), where the canal courses within the lateral sinus wall itself, followed by superficial position (6.2%), in which the canal lies beneath the outset layer of bone at the lateral sinus wall. These findings indicate that in more than half of the cases, the AAA travels directly beneath the Schneiderian membrane.
When examining the mediolateral course of the AAA canal from the second molar to the premolar region, the study revealed six distinct patterns, with the “in” type being the most frequent (32.4%). This pattern indicates that the canal maintains its position at the inner sinus wall throughout all the tooth locations. Other significant patterns included “middle to in” (19%), where the canal transitions from within the sinus wall to the inner aspect, and “middle” (19%), where the canal remains within the sinus wall throughout its course. The “through” pattern, where the canal crosses the sinus wall during its course, was observed in 17% of cases, while both “in/out to middle” and “out” patterns each accounted for 6% of the sample.
Discussion
The comprehensive findings of this CBCT-based study provide important anatomical and clinical insights into the AAA with direct implications for surgical procedures in the posterior maxillary region. Understanding these implications is crucial for minimizing complications and optimizing treatment outcomes in dental and maxillofacial interventions.
The anatomical characteristics observed in this study both align with and differ from previous research findings, while previous studies have reported a wide range of AAA prevalence (32.5%–100%),1,4,11,12,17 only cadaveric studies have consistently reported 100% prevalence.18–22 The current study’s detection rate of AAA was 92.2%.
CBCT has proven superior to other imaging modalities for AAA detection due to the vessel’s variable and often small diameter (typically < 1.5 mm). Studies using CBCT have demonstrated a prevalence range of 52.8%–94.6%, significantly higher than CT scans (32.5%–64%).11,12,23 Our study detected the AAA in 92.2% of patients using CBCT, slightly lower than the 94.6% reported by Laovoravit et al. 11 This difference may be attributed to variations in imaging protocols, specifically the voxel size used, which affects resolution and radiation exposure.
Regarding AAA canal location, the most common mediolateral position in this study was intrasinus (51.3%), followed by intraosseous (42.5%), and superficial (6.2%). These findings contrast with Valente 17 and Danesh et al., 24 who reported intraosseous as the most frequent, but align with Soundarajan et al., 2 Laovoravit et al., 11 and Kim et al. 13 The positional variations of the AAA canal have direct implications for specific surgical procedures. The predominance of intrasinus positioning (51.3%) indicates that in more than half of cases, the artery runs beneath the Schneiderian membrane. The high frequency of intrasinus positioning implies increased risk during sinus membrane elevation, while intraosseous and superficial canals are more prone to injury during lateral window osteotomy.
The diameter of the AAA canal represents a critical factor in assessing hemorrhage risk. While the mean diameter in this study was 1.20 mm, approximately 28% of canals measured 1.5 mm or larger. Previous literature suggests that arteries exceeding 2 mm in diameter pose significant bleeding risks if injured, while those between 1 and 2 mm may cause moderate hemorrhage.7,25 In this study, 4% of canals exceeded 2 mm in diameter, representing a high-risk category for severe bleeding complications. This finding emphasizes the importance of preoperative diameter assessment to identify patients at elevated risk for hemorrhagic complications. The mean AAA canal diameter in this study is consistent with previous reports.25–27 However, unlike some studies, we observed significant diameter variations based on age (p = 0.002) and gender (p = 0.008).12,14,28
The morphometric measurements of this study provide valuable quantitative guidance for surgical safety margins. We also investigated the distance of AAA to the sinus floor and alveolar crest. Our finding measurements revealed shorter distances to the sinus floor compared to Ciftci et al., 14 Yang and Kye, 26 and Laovoravit et al. 11 Distances to the alveolar crest showed mixed agreement consistent with Yang and Kye 26 and Watanabe et al., 27 while our values were higher than those reported by Ciftci et al. 14 The median distances from the AAA canal to the sinus floor ranged from 5.09 mm at the first premolar to 7.30 mm at the second molar. These measurements suggest that osteotomies for lateral window sinus lifts should ideally be positioned at least 7–8 mm superior to the sinus floor in the molar region to minimize the risk of arterial injury. Similarly, the distances to the alveolar crest, ranging from 16.70 mm at the second molar to 24.65 mm at the first premolar, provide reference points for vertical measurements during implant placement and ridge augmentation procedures.
Consistent with Ciftci et al., 14 we found that AAA dimensions (distance and diameter) were generally greater in males. Significant gender differences were observed in distances to the sinus floor (first and second molars) and the alveolar crest (first molar), while Laovoravit et al. 11 reported differences in the premolar and second molar regions for sinus floor distance. Generally, males exhibited larger measurements than females, suggesting anatomical differences that may be attributed to overall skeletal size variations between genders. These values provide average safety thresholds for sinus lift and osteotomy procedures in each gender.
Regarding laterality, the study found minimal differences between right and left sides, with the only statistically significant variation observed in the distance from the AAA canal to the alveolar crest at the first premolar (p = 0.021), where the right side exhibited a longer distance. The general bilateral symmetry in most measurements suggests that in most patients, the AAA canal maintains relatively consistent positioning on both sides of the maxilla, which may simplify surgical planning for bilateral procedures in the maxillary posterior region. 8
Dental status emerged as another influential factor affecting AAA canal measurements. The study revealed a significant difference in the distance to the sinus floor at the second molar between dentate and edentulous patients, a parameter not previously investigated in the literature. Additionally, differences were observed in the distance to the alveolar crest in the premolar regions based on dental status, contrasting with findings from previous studies. The longer distance at the second premolar in edentulous patients may be attributed to maxillary sinus pneumatization following tooth loss. Conversely, the shorter distances to the alveolar crest in both molar and premolar regions underscore the increased susceptibility to complications in these areas during surgical interventions.8,11,29
The interaction among age, dental status, and AAA canal measurements deserves particular attention. The study identified differences between the 20–39 and ⩾60 age groups, which contrasts with some previous studies.3,11 These variations may be partially explained by the influence of dental status. Older age groups typically have a higher prevalence of tooth loss, which triggers alveolar bone resorption and maxillary sinus pneumatization, thereby altering the spatial relationships between the AAA canal and reference points such as the sinus floor and alveolar crest. This complex interplay of factors underscores the need for comprehensive preoperative assessment that considers multiple patient-specific variables.
In this study, like others, the inferior border of the alveolar ridge as a reference point is used, thus alveolar bone resorption, which varies among individuals, must be considered.8,28 Although key variables such as gender, age, and dental status were examined, other potentially influential anatomical and physiological factors, such as skeletal classification, bone density, and the degree of maxillary sinus pneumatization, were not evaluated. These variables could affect the spatial relationship and dimensions of the AAA canal. Additional studies examining the correlation between the degree of ridge resorption or sinus pneumatization and changes in AAA canal position could provide valuable insights into the dynamic nature of maxillary anatomy following tooth loss. Additionally, minor variations in voxel size and CBCT scanning parameters, despite standardization efforts, may have influenced the detection and measurement accuracy of the AAA canal, particularly for smaller, or less calcified structures. Furthermore, prospective studies evaluating the clinical outcomes of surgical procedures guided by preoperative CBCT assessment of the AAA could quantify the benefit of this imaging approach in reducing complication rates during maxillary surgical interventions.
Conclusion
The study demonstrated a high prevalence of the AAA canal (92.2%), affirming the widespread presence of this vascular structure in the posterior maxillary region. The detailed anatomical characterization revealed considerable variability in the position, course, and dimensions of the AAA canal, influenced by factors such as tooth location, gender, age, and dental status.
The predominance of intrasinus positioning (51.3%) followed by intraosseous (42.5%) and superficial (6.2%) locations reflects the complex three-dimensional relationship between the AAA and the lateral wall of the maxillary sinus. Similarly, the variable mediolateral course from posterior to anterior regions, with six distinct patterns identified, underscores the dynamic nature of this vascular structure. These findings emphasize that surgeons cannot rely on assumptions about the AAA’s position but must instead evaluate each patient individually through appropriate imaging.
Footnotes
Acknowledgements
The authors would like to acknowledge the Shiraz University of Medical Sciences, for supporting the research (Grant#25043). The authors thank Dr. N. Asmarian from the Dental Research Development Center, for the statistical analysis. This article is based on the thesis of Dr. Zahra Mohammadi Jaberi.
Ethical considerations
This study was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.DENTAL.REC.1401.047).
Consent to participate
Written informed consent was obtained from all the participants or Legally Authorized Representatives.
Consent for publication
Not applicable.
Author contributions
MH and MP contributed to the study design and data interpretation. ZMJ and FH collected the data and assisted in article drafting. MH and FH critically revised the article. All the authors read and approved the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset generated and analyzed during the current study is available from the corresponding author on reasonable request.