
Abstract
Background:
Organizational effectiveness is vital in public hospitals, especially in low- and middle-income countries, including Ghana, where healthcare delivery faces resource constraints and high disease burdens. This study evaluates the organizational effectiveness of public hospitals in Ghana from the perspective of frontline healthcare workers.
Methods:
A cross-sectional study was conducted in four public hospitals using a validated World Health Organization questionnaire. A total of 477 frontline healthcare workers participated, assessing the perceived gap between current effectiveness (“as-is”) and ideal expectations (“should-be”) across 15 items. Data were analyzed using descriptive statistics and paired Student’s t-tests.
Results:
Significant gaps were identified between current organizational effectiveness and ideal expectations. The mean score for current effectiveness was 2.75 ± 0.63, while the ideal state scored 5.20 ± 0.43, yielding a significant mean difference of 2.45 ± 0.58 (p = 0.001). Major gaps were noted in conflict management, support for continuous learning, and valuing individual contributions. Only 8.4% rated their organizations as “extremely effective,” with 31% indicating a need for significant improvement.
Conclusion:
The findings reveal substantial gaps between current effectiveness and expectations, emphasizing the need for urgent reforms in conflict resolution, staff development, and fostering a learning-oriented culture to enhance hospital effectiveness and healthcare delivery in Ghana.
Keywords
Introduction
Organizational effectiveness in healthcare institutions—defined as the ability to achieve institutional goals through strong leadership, efficient systems, engaged staff, and a supportive environment that fosters high-quality, patient-centered care—is essential to ensuring that healthcare delivery meets the needs of patients, staff, and the wider community. 1 Hospitals that demonstrate high organizational effectiveness are better positioned to manage their workforce, adapt to changes in healthcare demands, and achieve national and international health objectives, including the United Nations’ Sustainable Development Goal 3, which aims to ensure healthy lives and promote well-being for all at all ages.2,3
In low- and middle-income countries (LMICs) such as Ghana, organizational effectiveness is especially important due to resource constraints, workforce shortages, and the rising burden of communicable and noncommunicable diseases.4,5 The performance of public hospitals, which serve the majority of the population, significantly influences public health outcomes, particularly for vulnerable groups.4,6 However, these hospitals often face considerable barriers, including poor infrastructure, inadequate supplies, and limited training opportunities for healthcare staff, all of which can hinder the delivery of optimal care. 6
Research on performance improvement in Ghanaian public hospitals has highlighted several areas of concern. Studies have shown that many hospitals suffer from poor communication between management and staff, inadequate staff development programs, and a lack of clear strategic goals.7–10 These issues contribute to inefficiencies in healthcare delivery, reduced employee morale, and, ultimately, poorer patient outcomes.7,8
Although substantial research has been conducted on organizational efficiency in healthcare settings,11–13 there is limited knowledge regarding the organizational effectiveness of public healthcare organizations in Ghana. While both organizational efficiency and organizational effectiveness are important in healthcare management, they focus on different aspects of performance. Organizational effectiveness emphasizes a hospital’s ability to achieve its goals—such as delivering timely, high-quality care, maintaining employee satisfaction, and optimizing resource use. 14 Effective organizations tend to have well-structured systems that promote collaboration, foster innovation, and support continuous improvement in healthcare delivery. 15 In contrast, organizational efficiency measures how well a hospital uses its resources to meet its objectives, focusing on the relationship between inputs (such as staff hours, equipment, and finances) and outputs (such as patient treatments and services delivered). Common metrics include cost per patient treated, bed occupancy rates, and turnover ratios. 16
While efficiency is necessary, healthcare managers should balance it with effectiveness to respond to environmental demands and improve overall performance.14,16 Understanding these concepts is crucial for evaluating and improving hospital performance in the evolving healthcare landscape. This study, therefore, aims to provide a frontline perspective on the organizational effectiveness of public hospitals in Ghana. Frontline healthcare workers—including medical doctors, nurses, pharmacists, and allied health professionals—play a central role in the daily operations of healthcare organizations. Their direct interactions with patients and their involvement in managing complex operational challenges make their insights invaluable in assessing hospital performance and identifying areas for improvement. This study is particularly relevant in the context of Ghana’s healthcare system, where public hospitals serve as the primary healthcare providers, especially for low-income populations.
Materials and methods
Study design and setting
A facility-based cross-sectional study was conducted among frontline healthcare workers in four public hospitals in Ghana from May 17 to July 16, 2024. The four hospitals that participated in the study were Kumasi South Hospital, Tamale Teaching Hospital, Efutu Municipal Hospital, and Winneba Traum and Specialist Hospital.
Study population
The study population comprised all frontline healthcare workers providing health and related services in public healthcare organizations in Ghana. However, only those who met the following criteria were included frontline healthcare workers in the participating hospitals who were over 18 years of age, had worked for at least a year, were available at the time of data collection, were willing to participate, and were of sound mind. Exclusion criteria included healthcare workers with managerial responsibilities, those not directly involved in patient care such as administrative and support staff, those on leave during the data collection period, and individuals with <1 year of work experience.
Sample size estimation and sampling procedure
With an estimated Ghanaian public sector healthcare workforce of 122,183, 17 the sample size for the study was determined using the Taro Yamane’s formula 18 :

where n = the expected sample size, N = finite population out of which the sample size is drawn, and e = level of precision (e = 0.05).
Substituting the above figures:

Nonresponse rate of 20% was added to give a total sample size of 479.
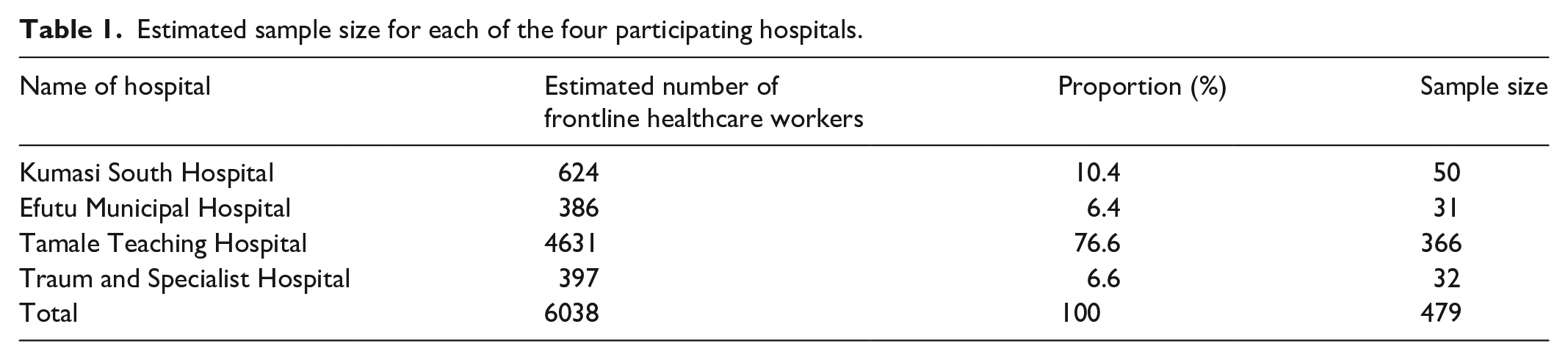
The study sample was selected using a multistage sampling approach. First, Ghana was divided into three clusters based on its ecological zones: coastal, middle belt, and northern. From these clusters, four hospitals were conveniently selected: two (Efutu Municipal Hospital, and Winneba Traum and Specialist Hospital) from the coastal belt, one (Kumasi South Hospital) from the middle belt, and one (Tamale Teaching Hospital) from the northern belt. This convenience sampling was chosen to minimize costs and logistical challenges by focusing on easily accessible hospitals. Next, we employed a proportional sampling method to draw 479 frontline healthcare workers from the four hospitals (Table 1) to participate in the study. Each hospital’s total number of frontline healthcare workers was treated as an independent subpopulation. The sample size for each hospital was determined by calculating the proportion of frontline healthcare workers at that hospital relative to the total number across all four hospitals and then multiplying this proportion by the total sample size. Finally, a consecutive sampling technique was used to select the required study participants. In this process, every eligible healthcare worker meeting the inclusion criteria was selected until the desired sample size for each hospital was reached.
Estimated sample size for each of the four participating hospitals.
Measuring organizational effectiveness
To assess the effectiveness of the participating hospitals, we utilized a validated questionnaire developed by the World Health Organization (WHO). 19 This tool is designed to evaluate an organization’s effectiveness in creating an environment conducive to change and improving performance. The questionnaire includes 15 closed-ended questions that compare the current state of the organization (the “as-is” condition) with an ideal state (the “should-be” condition). Respondents are asked to rate their organization’s current performance on a scale from 1 (very poor performance) to 6 (excellent performance) by marking an “×” in the appropriate box. After completing this step, they repeat the exercise, this time using a “√” to represent what they consider to be the ideal level of effectiveness for their organization. The final item asks respondents to rate the overall effectiveness of their organization, with options ranging from “One of the best, extremely effective” to “Marginally effective, needs revamping.” The difference between the ratings of “My organization as-is” and “My ideal organization” offers insight into how far employees perceive their organization from reaching optimal effectiveness.
In addition to evaluating the overall effectiveness of the public hospitals, we categorized the questionnaire items to compare the “hard” (technical) and “soft” (social) organizational elements of the hospitals, using the McKinsey 7-S Framework. According to the McKinsey 7-S Framework, hard organizational elements include structure, which defines organizational hierarchies, roles, and responsibilities; systems, which manage processes such as HR for recruitment and promotion; and strategy, which focuses on activities aimed at achieving goals, such as improving public health. 20 Soft elements consist of skills, representing employees’ capabilities; staff, referring to the workforce’s diverse knowledge and experience; style, which governs the allocation of rights and responsibilities; and shared values, which reflect the beliefs and attitudes that shape the organization’s culture and mission. 20 We categorized the questionnaire items around this framework, covering shared values (two items—the organization has a set of guiding beliefs, general objectives, and values are set forth), strategy (one item—the organization operates in a purposeful mode), structure (one item—structures are designed based on work requirements), systems (three items—decision are made based on location of information, collaboration is rewarded, the organization is seen as an open system), style (six items—managers assume individuals want more responsibility, rewards are balanced, communication is open, conflict is managed, individuals are valued, management respects people), staff development (one item—an effort is made to inspire people), and skills (one item—there is a “learning” mode of management).
To ensure the appropriateness and clarity of the instrument for the local context, the questionnaire was pilot-tested among 48 frontline healthcare workers, representing ~10% of the total study sample, at Komfo Anokye Teaching Hospital in Kumasi, located in the Ashanti Region of Ghana. The pilot test aimed to assess whether the items were clear, understandable, and interpreted as intended by the target population.
Data collection
Data were collected from the frontline healthcare workers using a structured questionnaire, which included sections on background information, the WHO’s 15-item organizational effectiveness assessment, and one item assessing the overall effectiveness of the public hospitals (see Supplementary File). An institutional-based data collection approach was employed, ensuring that data collection was conducted within the public hospitals. Four trained field assistants were engaged in the process to help administer the questionnaire and ensure consistency across respondents. These assistants received comprehensive training to standardize the data collection and minimize potential bias. Verbal informed consent was obtained from all participants prior to data collection, in accordance with the approved ethical guidelines.
Data analysis
Descriptive statistics (frequencies and percentages) were used to summarize the demographic characteristics of the healthcare workers. To assess the organizational effectiveness, we first calculated the mean scores for each of the 15 items comparing the current state of the organization (“My organization as is”) to an ideal state (“My ideal organization”). From these, we computed overall mean scores for both the “as-is” and “ideal” states. Next, composite mean scores were calculated for the hard (five items) and soft (10 items) organizational elements, which were combined to form overall mean scores for these elements. The degree of change needed in the public hospitals’ performance was evaluated by comparing the differences between the “as-is” and “should-be” scores. To determine the significance of these differences, a paired Student’s t-test was conducted, with a significance level set at 0.05. All analyses were performed using SPSS software version 20 (IBM© Corporation, Armonk, NY, USA).
Ethical statement and approvals
Ethical clearance for the study was obtained from the Institutional Review Board of the Tamale Teaching Hospital (reference no. TTH/R&D/SR/24/103). In addition, permission was obtained from the authorities of the participating hospitals before the commencement of the study. The purpose of the study was clearly explained to all participants, including the objectives, procedures, potential risks and benefits, and their rights as participants. They were informed that participation was voluntary, that they could withdraw at any time without consequence, and that all information provided would be treated with strict confidentiality and used solely for research purposes. Once participants confirmed their understanding of the information and had no further questions, verbal consent was obtained, and the research team proceeded with data collection This procedure for obtaining oral informed consent was reviewed and approved by the Institutional Review Board of the Tamale Teaching Hospital.
Results
Out of the 479 administered questionnaires, 477 were returned, resulting in a response rate of 99.6%. The average age of the healthcare workers was 33.9 ± 6.8 years. The majority were aged 31–40 (48.4%), female (57.2%), and married (50.3%). Most identified as Christian (65.6%) and worked primarily as nurses (30.8%). In terms of work experience, the largest group had worked for 4–6 years (42.6%; Table 2).
Characteristics of the study respondents.

Organizational effectiveness
The healthcare professionals reported a significant disparity between their current and ideal organizational environments. On average, participants rated their current organizations notably lower (mean = 2.75 ± 0.63) than their ideal (mean = 5.20 ± 0.43), indicating widespread dissatisfaction with key organizational dimensions. This perceived gap was reflected across all fifteen items assessed (see Table 3), suggesting a systemic challenge rather than isolated issue.
Comparison of organizational characteristics between current state and ideal state.
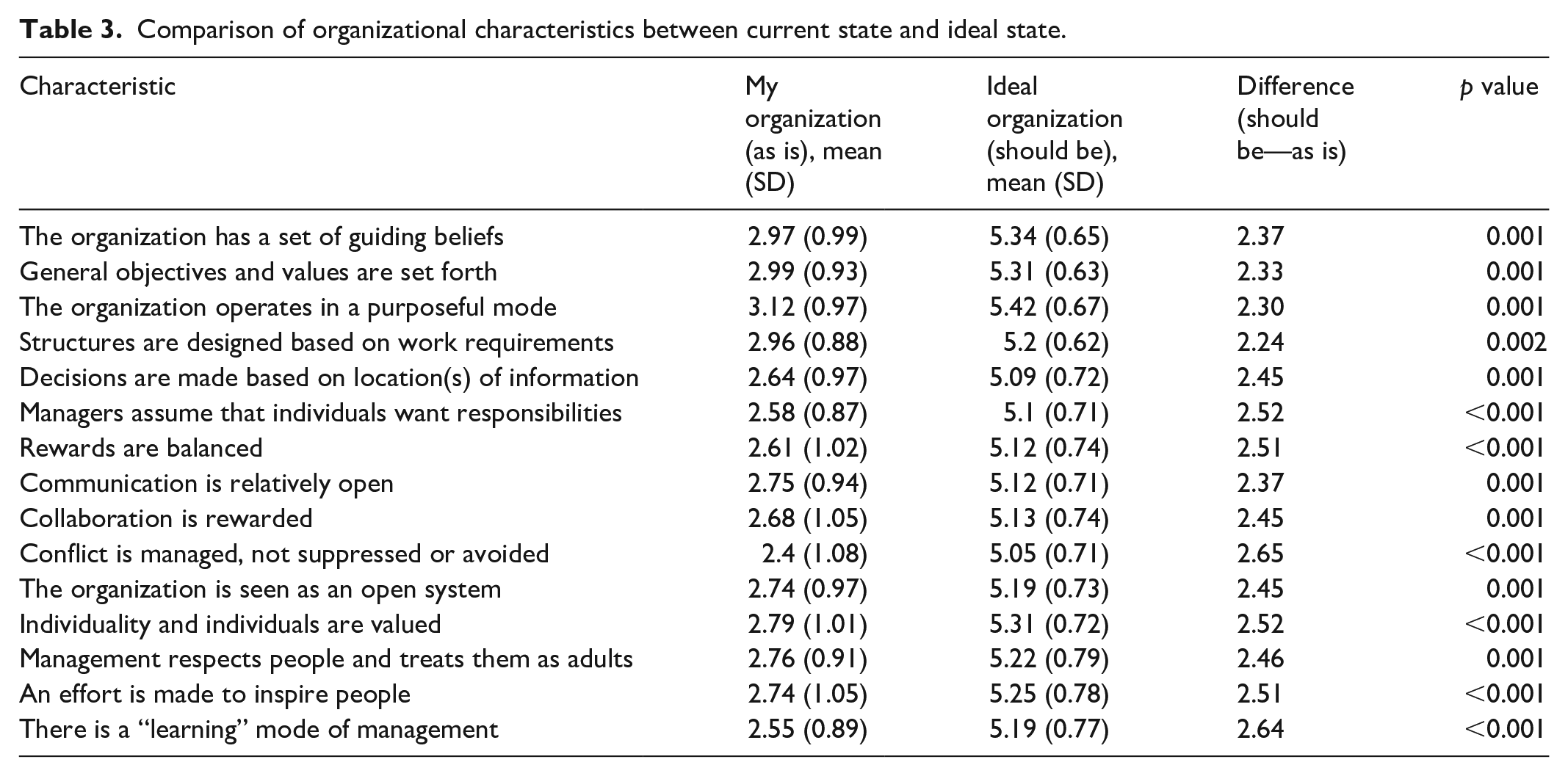
When comparing specific organizational characteristics, the characteristics with the highest differences were “Conflict is managed, not suppressed or avoided,” “There is a learning mode of management,” “Managers assume that individuals want responsibilities,” and “Individuality and individuals are valued.” Conversely, the characteristics with the lowest differences were “Structures are designed based on work requirements,” “The organization operates in a purposeful mode,” “General objectives and values are set forth,” and “Communication is relatively open” (see Table 3 and Figure 1).

Difference in mean scores between the “as is” and the “should be” modes of organizational effectiveness.
A comparison between the hard and soft elements revealed that participants rated the hard elements slightly more favorably, with an average score of 2.83 compared to 2.71 for the soft elements. Although the difference in mean scores was relatively small (0.012), it was statistically significant (t(476) = 5.681, p = 0.013).
Finally, the overall perception of organizational effectiveness was notably low. Fewer than one in ten respondents (8.4%) considered their hospital to be “one of the best, extremely effective.” The majority, however, offered more reserved or critical assessments. Approximately 31% felt that their organization was effective in certain areas but required significant improvements in others, while nearly 10% viewed their hospital as only “marginally effective” (see Figure 2).
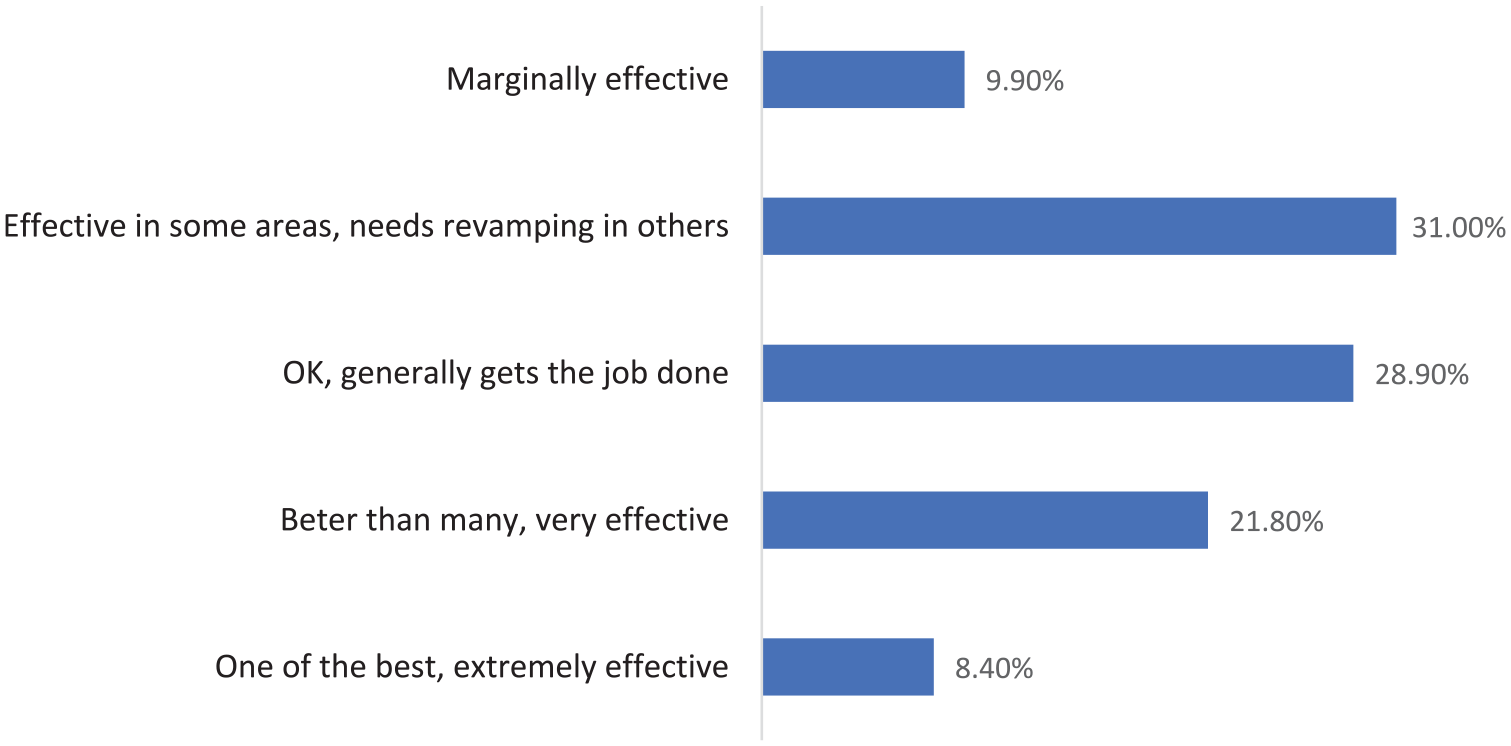
Overall rating of organizational effectiveness.
Overall mean score for ideal organization = 5.20 ± 0.43; current organization (my organization as is) mean score = 2.75 ± 0.63; difference between ideal and current mean score = 2.45 ± 0.58. This difference was statistically significant, t(476) = 91.640, p = 0.001; 95% CI: 2.40–2.50.
Discussion
The findings from this study highlight the disparity between the current state of the assessed organizations and the workers’ ideal expectations. The overall perception of organizational effectiveness was low, with a substantial gap identified between the healthcare workers’ ratings of their current organization and their ideal organization. Importantly, this gap was consistently observed across all 15 organizational items assessed, reinforcing the need for urgent reforms in hospital management and operational practices.
Among the specific organizational characteristics evaluated, the highest perceived gaps were related to conflict management, managerial responsibilities, and valuing individuality. These characteristics are integral to fostering a positive organizational culture that promotes teamwork, personal growth, and efficient conflict resolution. For instance, the largest gap (2.65) was found in the item “Conflict is managed, not suppressed or avoided.” This suggests that workers perceive a lack of effective conflict resolution mechanisms, which may lead to unresolved tensions, decreased morale, and lower overall effectiveness. Similarly, a gap of 2.64 was identified for “There is a learning mode of management,” indicating dissatisfaction with management’s support for continuous learning and professional development. Earlier studies8,21 have identified inadequate staff development programs as a major concern in Ghanaian public hospitals, emphasizing the need for improving training and learning initiatives in these healthcare organizations.
In contrast, characteristics with the lowest differences, such as “Structures are designed based on work requirements” (gap = 2.24) and “The organization operates in a purposeful mode” (gap = 2.30), suggest that while there are still significant gaps, certain structural aspects of the organization may be relatively better aligned with workers’ expectations. However, these smaller differences should not detract from the overall message that substantial improvements are needed across all organizational dimensions.
The finding that hard elements received a slightly higher mean score than soft elements, despite a small but statistically significant difference, aligns with a similar study conducted in Poland. 22 In that study, soft aspects had significantly lower scores (p < 0.05), with a mean of 2.58 (95% CI: 2.43–2.73), compared to the hard aspects, which had a mean score of 2.80 (95% CI: 2.66–2.94). These observations suggest that healthcare workers perceive the structural and operational frameworks within their organizations to be relatively better than the intangible, interpersonal aspects. This implies that the foundational systems—such as policies, procedures, and technological resources—are more developed or functional compared to the softer aspects such as leadership and communication. It must be noted however that in this study, both hard and soft elements still received low scores, reflecting an overall perception of inadequacy in both areas.
The results of this study have significant implications for healthcare policy and practice in Ghana, particularly regarding workforce management and hospital operations. Policymakers and healthcare managers must prioritize strategies that address the substantial gaps between current organizational conditions and the expectations of healthcare workers. A critical area of focus should be the development and implementation of policies that enhance conflict resolution mechanisms within hospitals, as conflicts—whether relational, task-related, or process-related—are inherent in the healthcare environment.23,24 The effectiveness of organizations largely depends on how these conflicts are managed.25,26 It may, therefore, be beneficial for policymakers to promote training programs and systems that empower staff and management to address conflicts proactively and constructively.
For healthcare managers, the findings underscore the need to actively address conflicts in a transparent and fair manner. Suppressing or avoiding conflicts, as perceived by the workers, can have detrimental effects on team cohesion and morale. Managers should foster open communication channels that allow for constructive dialogue and mediation when conflicts arise. Additionally, policy interventions should aim to foster a culture of continuous learning and professional development within healthcare organizations. The gap in the perception of a “learning mode of management” suggests that workers feel unsupported in their professional growth, which can lead to disengagement and reduced job satisfaction. Policymakers should advocate for resources and programs that encourage lifelong learning, skills enhancement, and leadership development for healthcare professionals.
The gap in valuing individuality and assuming individuals want responsibilities suggests that hospitals need to empower their staff by providing more opportunities for autonomy and professional growth. Managers should strive to recognize and reward individual contributions, as well as delegate meaningful responsibilities that align with workers’ skills and interests. This would not only improve job satisfaction but also enhance organizational effectiveness by capitalizing on the diverse talents and motivations of the workforce. 27 The findings also point to a need for policies that better align the structure of healthcare organizations with their operational goals. While the gaps in structural elements were smaller than in other areas, they indicate that healthcare workers feel that the current organizational designs do not fully meet their needs or the demands of the job. By ensuring that hospital structures are adaptable and responsive to frontline workers’ feedback, policymakers can contribute to more effective and efficient healthcare delivery.
This study opens several avenues for further research. First, future studies should investigate the underlying factors contributing to the large gaps in specific organizational characteristics, such as conflict management and learning modes of management. In particular, qualitative research is recommended to explore the root causes of these gaps, as it would provide in-depth insights that complement the current quantitative findings. By understanding the contextual and systemic factors driving these issues, researchers can propose more targeted and contextually relevant interventions. Additionally, comparative research across different regions or healthcare systems could shed light on whether the gaps observed in this study are unique to Ghana or indicative of broader trends in healthcare organizations in LMICs. Such research would be invaluable for informing global health policy and improving organizational effectiveness in diverse healthcare settings. Furthermore, it would be valuable for future studies to explore how individual characteristics—such as sex, education, and years of experience—relate to overall effectiveness ratings. This line of inquiry could offer additional explanatory power and refine strategies for workforce development and organizational improvement.
Limitations
While this study provides valuable insights into healthcare organizational effectiveness from the perspectives of frontline healthcare workers, several limitations should be considered when interpreting the findings. The use of convenience sampling to select the four hospitals restricts the generalizability of the results, as the chosen hospitals may not fully represent the broader landscape of public hospitals in Ghana. Additionally, though the hospitals were selected from different ecological zones, the small sample size may not adequately capture the variation in organizational effectiveness across the country, especially in regions with differing healthcare challenges. Moreover, reliance on self-reported data could introduce response bias, as participants may rate their organizations more favorably or unfavorably based on personal experiences. Finally, the study’s cross-sectional design limits its ability to assess changes or trends in organizational effectiveness over time.
Conclusion
The evaluation of organizational effectiveness in public hospitals in Ghana, as perceived by frontline healthcare workers, revealed significant gaps between the current organizational environment and workers’ ideal expectation. These gaps were particularly pronounced in areas such as conflict management, managerial responsibilities, and valuing individuality. The findings have far-reaching implications for policy, practice, and research, underscoring the need for interventions that enhance conflict resolution, support continuous learning, and align organizational structures with operational goals. By addressing these issues, policymakers and healthcare managers can improve the effectiveness of public hospitals, ultimately leading to better healthcare outcomes for the population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251365757 – Supplemental material for Perceptions of organizational effectiveness in public hospitals: Insights from frontline healthcare workers in Ghana
Supplemental material, sj-docx-1-smo-10.1177_20503121251365757 for Perceptions of organizational effectiveness in public hospitals: Insights from frontline healthcare workers in Ghana by Emmanuel Kumah, Dorothy Serwaa Boakye, Richard Boateng, Michael Afari Baidoo, Emmanuel Osei Tutu, Osman Ibrahim, Sandra Abakah, Eric Kwabena Asante Osei and Maxwell Derrick Nyame in SAGE Open Medicine
Footnotes
Ethical considerations
Ethical clearance was obtained from the Institutional Review Board of the Tamale Teaching Hospital under reference no. TTH/R&D/SR/24/103. In addition, we obtained permission from the authorities of the participating hospitals before commencing the study.
Consent to participate
All participants provided oral informed consent prior to their involvement in the study.
Author contributions
Emmanuel Kumah: conceptualization, methodology, formal analysis, investigation, writing—original draft preparation, writing—review and editing, supervision. Dorothy Serwaa Boakye: methodology, formal analysis, writing—review and editing. Richard Boateng: methodology, formal analysis, writing—review and editing. Michael Afari Baidoo: methodology, formal analysis, writing—review and editing. Emmanuel Osei Tutu: conceptualization, investigation, writing—original draft preparation. Osman Ibrahim: conceptualization, investigation, writing—original draft preparation. Sandra Abakah: conceptualization, investigation, writing—original draft preparation. Eric Kwabena Asante Osei: investigation, writing—review and editing. Maxwell Derrick Nyame: investigation, writing—review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this analysis are available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.