
Abstract
Immune checkpoint inhibitors therapy in cancer patients may induce immune-related diabetes mellitus through islet β-cell destruction, necessitating systematic glycemic management. This scoping review aims to identify and synthesize evidence on glycemic management strategies for immune-related diabetes mellitus. Guided by Arksey and O’Malley’s five-stage scoping review framework, we strictly adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist. A systematic search was conducted across guideline repositories, academic databases, and professional oncology/endocrinology association websites. The search period spanned from database inception to June 30, 2024. Of 5085 initially identified records, 9 studies met inclusion criteria. Evidence was synthesized into five key domains: (1) risk assessment and early detection, (2) therapeutic interventions and monitoring, (3) patient education, (4) glycemic target optimization, and (5) multidisciplinary care coordination. This review consolidates evidence-based best practices for immune-related diabetes mellitus management derived from rigorous methodology. Clinicians should tailor these strategies to individual patient profiles to optimize outcomes while mitigating treatment disruptions.
Introduction
With the increasing of global cancer burden,1,2 cancer treatment methods and pharmacological interventions are rapidly evolving. Immune checkpoint inhibitors (ICIs), as one of the typical representative, have demonstrated significant efficacy in tumor control. ICIs exert their antitumor effects by blocking interactions between tumor cells and immune checkpoints expressed on immune cells, thereby disrupting the immunosuppressive signaling pathways exploited by malignancies. 3 These agents are now explicitly recommended as first-line therapies for numerous advanced cancers in clinical guidelines.4,5
With the widespread clinical application of ICIs, associated toxicities, particularly endocrine-related adverse events, have become increasingly recognized. Immune-related diabetes mellitus (IR-DM) is a documented endocrine complication following PD-1/PD-L1 inhibitor therapy. 3 Although the pathogenesis of IR-DM remains incompletely understood, ICIs treatment may trigger CD4+ Th1 cell proliferation and CD8+ T-cell infiltration into pancreatic tissue, resulting in islet β-cell destruction. 6 IR-DM affects approximately 1%–2% of cancer patients receiving ICIs regimens,3,7–10 but its reported incidence is rising due to expanding clinical indications,11–13 and 70% of these patients may rapidly progress to life-threatening hyperosmolar hyperglycemic state (HHS) or diabetic ketoacidosis (DKA), 10 posing significant challenges for clinical management.
The association between IR-DM and oncological outcomes, including tumor response rates and overall survival, remains incompletely confirmed. Although existing studies on IR-DM are limited by small sample sizes, some reports suggest that 70%–80% of these patients achieve partial or complete tumor remission.14–16 Paradoxically, diabetes mellitus has been established as an independent predictor of poor tumor prognosis.17,18 Glycemic distress and hyperglycemia are established risk factors for cardiovascular disease and immunosuppression, which may further elevate patients’ risks of infection and heart failure.19–21 Thus, further research is warranted to clarify the correlation between IR-DM and survival or clinical outcomes in cancer patients. Notably, IR-DM often manifests rapidly, resulting in accelerated deterioration of pancreatic β-cell function. In many cases, DKA is the initial presenting symptom.9,14,22–24 Furthermore, the pancreatic damage caused by IR-DM is largely irreversible, underscoring the critical need for vigilant clinical management in these patients.7,8
The reported incidence of IR-DM is low across regions, and direct evidence supporting its management remains limited. Furthermore, due to the prioritization of cancer diagnosis, treatment, and clinical care, healthcare professionals and patients may overlook blood glucose monitoring.8,25,26 However, IR-DM may lead to severe clinical complications in cancer patients. Therefore, urgent research is needed to explore effective management strategies for this condition.
This scoping review aims to identify and evaluate evidence-based approaches for managing IR-DM guided by Arksey and O’Malley’s five-step method, 27 with the goal of optimizing standardized and effective glycemic management in this patient population.
Methods
In this scoping review, the five-step method of scope review proposed by Arksey and O’Malley was taken as the theoretical framework. 27 The list of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews was strictly followed. 28
The first step: Identifying the research questions
The final literature search strategy guided by the PICO framework. Two researchers with expertise in evidence synthesis independently validated the search strategy to minimize bias.
P (Population): Patients with IR-DM.
I (Intervention): Glycemic control strategies.
C (Control): Not applicable (noncomparative design).
O (Outcome): Glycemic management level and clinical outcomes.
The identification of IR-DM management measures was guided by our primary research question: What evidence-based strategies effectively manage hyperglycemia in patients with IR-DM?
The second step: Identifying relevant studies
A comprehensive literature search was conducted across the following databases and resources:
International databases
BMJ best clinical practice, Up To Date, PubMed, Web of Science, CINAHL, Embase, EBSCO, Cochrane Library, Guidelines International Network, National Institute for Health and Care Excellence, Scottish Intercollegiate Guidelines Network, National Comprehensive Cancer Network, Registered Nurses’ Association of Ontario, National Guideline Clearinghouse, American Society of Clinical Oncology, and Joanna Briggs Institute, and endocrinology association websites.
Chinese databases
Wanfang Data, China National Knowledge Infrastructure, CQVIP, China Biomedical Literature Database, and Chinese Medical Association.
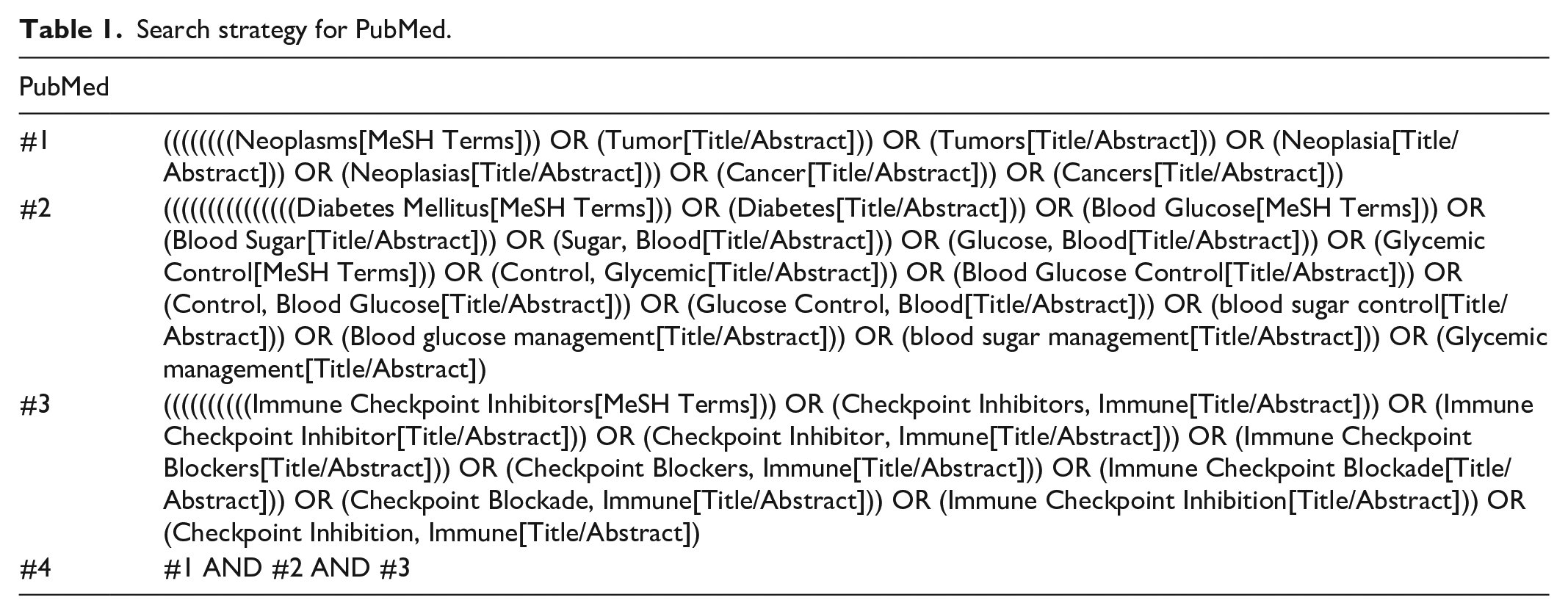
The search strategy for PubMed is presented in Table 1. All retrieved studies were managed using EndNote X9 reference management software.
Search strategy for PubMed.
The third step: Study selection
Two researchers independently screened the studies, with discrepancies resolved through consultation with a third investigator to reach consensus. The search period spanned from database inception to June 2024.
Inclusion criteria of literatures: Studies of any design; English or Chinese language; Focused on glycemic management strategies for cancer patients with IR-DM. Exclusion Criteria of literatures: Duplicate publications or studies with unavailable full texts. Superseded versions of updated guidelines or consensus statements. The literature selection step is detailed in Figure 1.

Flowchart of the study screening process.
The fourth step: Charting the data
Following the exclusion of duplicate publications, two researchers independently screened the remaining studies. Titles and abstracts were reviewed to exclude studies and conference abstracts irrelevant to the research theme or target population. Ultimately, nine studies were retained after excluding those that (1) lacked alignment with the research objectives; (2) had unavailable full texts; (3) were published in languages other than English or Chinese. Discrepancies between the two researchers during screening were resolved through discussion with a third investigator to achieve consensus.
The fifth step: Collating and reporting the results
Data extraction and synthesis were performed independently by two researchers, following a protocol consistent with the literature screening process. Key variables, including author, publication year, study region, data source, and thematic focus were systematically extracted. Discrepancies were resolved through consensus discussions involving a third investigator. The synthesized findings from the included studies are summarized in Table 2.
The characteristics of included literatures (n = 9).

UK: The United Kingdom of Great Britain and Northern Ireland; ESMO: European society of endocrinology; ASCO: American society of clinical oncology; SITC: society for immunotherapy of cancer.
Results
A total of 5058 studies were initially identified using the predefined search strategy. 2032 studies remained after removing duplicates. Sixty-two studies were obtained after title and abstract screening. Nine studies were following full-text assessment, nine studies met the inclusion criteria: seven clinical guidelines,7,8,29–33 one expert consensus statement, 34 and one clinical policy document. 35
Among the included studies, assessment and early identification was addressed in eight articles.7,8,30–35 Treatment and monitoring strategies were proposed in seven studies.8,30–35 Glycemic control goals targets were specified in three studies.7,8,29 Health education recommendations were provided in eight studies.7,8,29,31–35 Multidisciplinary team management for glycemic control was emphasized in four studies (Table 2 and Figure 2).8,29,30,33

Distribution of the management skills included in the studies.
Discussion
Since the first ICI was approved by the U.S. Food and Drug Administration (FDA) in 2011. 36 These agents have revolutionized oncology practice, emerging as a landmark therapeutic approach that offers new hope for durable cancer remission. Nevertheless, optimal strategies for the prevention, early detection, and effectively management of treatment-related adverse events remain underexplored. Currently, no validated predictors of IR-DM have been established. Consequently, prompt identification and evidence-based intervention for IR-DM are critical for optimizing patient safety outcomes. This study synthesizes evidence-based management approaches for IR-DM, summarized in Table 3.
The management skills of patients with IR-DM.
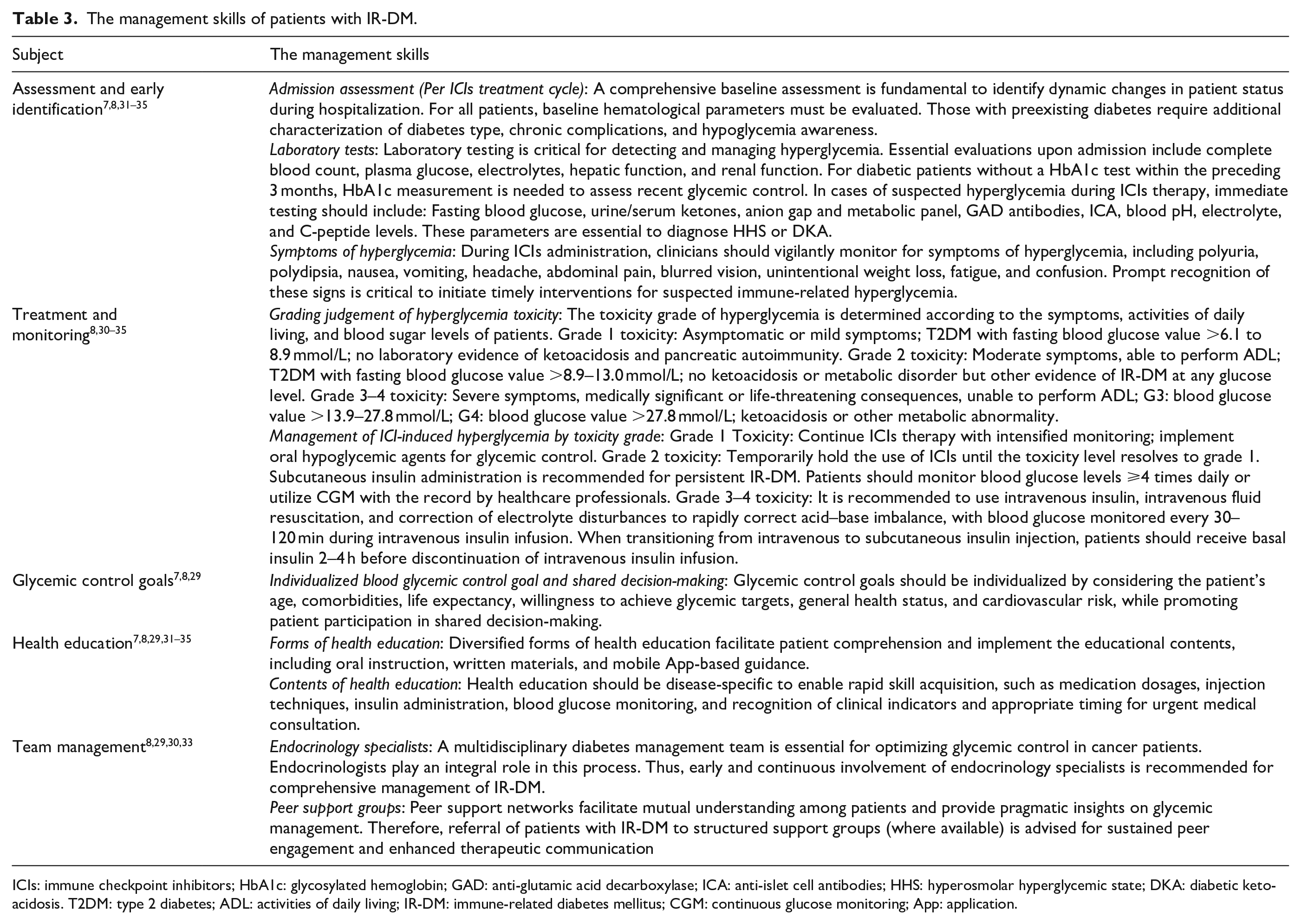
ICIs: immune checkpoint inhibitors; HbA1c: glycosylated hemoglobin; GAD: anti-glutamic acid decarboxylase; ICA: anti-islet cell antibodies; HHS: hyperosmolar hyperglycemic state; DKA: diabetic ketoacidosis. T2DM: type 2 diabetes; ADL: activities of daily living; IR-DM: immune-related diabetes mellitus; CGM: continuous glucose monitoring; App: application.
Early identification of hyperglycemic toxicity necessitates comprehensive evaluation of hematological indices and disease-specific parameters, including blood glucose levels, hepatic and renal function profiles, complete blood count, HbA1c, diabetes classification, glycemic control status, and diabetes management literacy.7,8,30–35 Notably, positive islet autoantibodies demonstrate association with accelerated IR-DM onset. 37 However, given their unestablished predictive value, baseline routine screening is not currently recommended. Pretherapy autoantibody testing should be individualized based on clinical judgment and patient-specific comorbidities. Clinicians must maintain heightened awareness of hyperglycemia and hypoglycemia-related symptoms during ICIs administration, with vigilant monitoring for their emergence.8,30–35 IR-DM encompasses a spectrum of ICI-induced hyperglycemic disorders wherein Type 1 diabetes (T1DM) predominates, while T2DM manifests less frequently.37–39 Immune-related pancreatitis and acquired generalized lipodystrophy represent rare entities within this continuum.40–42 This etiological heterogeneity complicates phenotypic differentiation, posing significant diagnostic challenges. Upon clinical suspicion of hyperglycemia, immediate laboratory assessment must include blood glucose, serum/urine ketone, blood PH, C-peptide levels, islet autoantibodies.8,30–32,34,35 Islet autoantibodies and C-peptide level serve as pivotal biomarkers for confirming immune-related T1DM (IR-T1DM), warranting prioritized evaluation during acute presentations.
Regular blood glucose monitoring and systematic laboratory assessment are essential for evaluating therapeutic efficacy in IR-DM and determining eligibility for ICIs rechallenge. 24 Under rigorous clinical supervision, Grade 1 toxicity may be managed without ICI interruption. When toxicity progresses to Grade 2 or higher, ICIs therapy must be suspended until resolution to Grade 1. Evidence indicates that rechallenge with ICIs may be feasible in patients experiencing Grade 2 or higher toxicity. 43 Insulin therapy (subcutaneous or intravenous) constitutes the cornerstone of hyperglycemia management. Regimen formulation requires shared decision-making between clinicians and patients, with dosing individualized according to age, prognosis, functional status, and glycemic patterns.30–32 During intravenous insulin administration for HHS or DKA, frequent glucose monitoring (every 30–120 min) is critical to prevent hypoglycemia. 8 Critically, transitioning from intravenous to subcutaneous insulin necessitates basal insulin administration 2–4 h before discontinuing intravenous infusion. 8 This protocol is frequently overlooked by nonendocrinology clinicians, underscoring the need for standardized management algorithms and multidisciplinary education initiatives. Future quality improvement initiatives should prioritize integrating this insulin transition protocol into electronic medical record alert systems for nonspecialist clinicians in primary care settings.
Structured health education delivers significant clinical benefits for patients with IR-DM. Most cases of IR-DM manifest within the initial 3 months of ICIs initiation, although delayed onset up to 12 months has been documented.32,33 Nearly all patients with IR-DM require lifelong insulin therapy. 44 Consequently, optimizing both delivery modalities (e.g., verbal instruction, written materials, and mobile applications) and evidence-based educational content, including medication dosing, injection techniques, insulin protocols, blood glucose monitoring methodologies, and recognition of indications for urgent medical consultation, is critical to enhance patient self-management capabilities.7,29,31,35
Glycemic targets for patients with IR-DM require personalization. Currently, no unified goals exist for cancer patients. The guiding principle is that target benefits must outweigh associated risks.7,8,29 The standards of medical care in diabetes recommend HbA1c goal <7% for most cancer patients. 45 However, IR-DM often presents with rapid hyperglycemia despite normal HbA1c due to abrupt β-cell destruction, making glucose-centric targets more clinically relevant. A UK guideline for ambulatory cancer patients proposes a broad glucose target range of 6.0–12.0 mmol/L (108–216.0 mg/dL) without specifying target ranges for different measurement times. 7 China’s guideline suggests moderately relaxed targets for immunotherapy recipients: Fasting blood glucose: 6.1–7.8 mmol/L (109.8–140.4 mg/dL), postprandial/random blood glucose: 7.8–10.0 mmol/L (140.4–180 mg/dL), and HbA1c/% is 7.0–8.0 mmol/L. 8 Tailored adjustments should be instituted based on the patient’s functional status, psychological resilience, and self-management engagement. This individualized approach optimizes the risk benefit profile of therapy, addresses unique patient needs, and enhances involvement in shared decision-making participation of patients for co-management of two diseases.
Close collaboration between endocrinologists and oncologists is essential for prompt diagnosis, treatment, and monitoring of IR-DM. 24 Hyperglycemia not only necessitates treatment interruption but also rapidly progresses to life-threatening HHS or DKA. Studies demonstrate that endocrinology teams significantly improve glycemic control and clinical outcomes in affected patients. 46 Since sustained hyperglycemia induces irreversible islet β-cell damage and profound insulin deficiency, autoimmune diabetes in this context is typically irreversible.8,44 Thus, endocrinology teams should initiate and maintain involvement in blood glucose management for IR-DM patients at the earliest clinical indication.8,29,30 While health education provided by clinicians has inherent limitations, peer support substantially enhances self-management competencies and disease knowledge among patients. 47 Patients with IR-DM should therefore be actively connected to disease specific support groups (where available) to access peer-driven management strategies. 29
Limitations
This study employed a rigorous literature screening process guided by Arksey and O’Malley’s five-stage scoping framework to synthesize comprehensive glycemic management strategies for patients with IR-DM. The absence of original randomized controlled trials on IR-DM management and reliance on a few extrapolated guidelines from general diabetes care underscores the urgent need for condition specific clinical trials. Furthermore, international discrepancies in glycemic target setting reveal the absence of a global standard. These limitations compromise the robustness of evidence-based management strategies and emphasize the necessity for further research to address these gaps. Restricting inclusion to English and Chinese sources, while excluding diverse clinical perspectives, risks omitting relevant evidence. Future studies should incorporate multilingual literature to ensure comprehensive evidence synthesis.
Moreover, although hypoglycemia management represents a critical safety priority for patients IR-DM, this scoping review focuses primarily on hyperglycemia control. Consequently, hypoglycemia protocols receive limited coverage. In clinical practice, effective glycemic management demands a dual approach encompassing both hypoglycemia prevention and rapid therapeutic correction to mitigate treatment-associated risks.
Conclusion
Due to the rarity of IR-DM and the unclear correlation with oncologic outcomes, current understanding remains incomplete and may limit the comprehensiveness of evidence-based management strategies. Although IR-DM incidence is low, its propensity to induce severe complications necessitates vigilant clinical management. The paucity of original research underscores the importance of leveraging existing guidelines and consensus statements for clinical guidance. The guidelines and consensus statements included in this study were evaluated against established quality criteria to ensure reliability and applicability. They provide a foundational framework for evidence-based management despite the lack of IR-DM specific original research. Current recommendations consistently emphasize core components: risk assessment and early identification, therapeutic monitoring, patient education, and multidisciplinary collaboration. Nevertheless, standardized glycemic targets for oncology patients remain undefined.
The results are based on a limited number of studies, predominantly guidelines and consensus statements, reflecting a scarcity of high-quality, original clinical studies on IR-DM management. Persistent knowledge gaps include unclear pathogenesis, absence of unified diagnostic criteria, and insufficient high-grade evidence. Establishing a global IR-DM registry could facilitate: elucidation of disease mechanisms, identification of predictive biomarkers, development of evidence-based diagnostic criteria, and formulation of standardized management protocols.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Not applicable.
Author contributions
Yuan Jiang, Xiaoyan Wang, Lihua Liu, and Gang Feng were involved in the design and concept of the review protocol. Yuan Jiang, Lei Lei, Danfeng Wu, Siqi Zhang, and Dairong Tang screened the data. Yuan Jiang, Lei Lei, Wen Zhou, Lingli Fan and Xiaojing Xue extracted the data. All authors reviewed and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study funded by the Wu Jieping Medical Foundation and the grant number was 320.6750.2023-05-81.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.