
Abstract
Background:
Hospital-acquired infections constitute a significant source of morbidity and mortality for both patients and healthcare professionals. Nursing professionals constitute an integral component of any quality-related program in a hospital, given their oversight and provision of nearly all healthcare services. Nurses’ knowledge and attitudes play a significant role in healthcare delivery. Within Saudi Arabia, the prevalence of hospital-acquired infections in hospital settings has prompted a growing emphasis on evaluating nursing knowledge and adherence to practice standards aimed at hospital-acquired infection prevention.
Methods:
This single-center cross-sectional study was conducted at the emergency department of King Faisal Medical Complex, Taif, between October and December 2022, involving 168 nurses. The study utilized a pre-validated structured online questionnaire comprising three sections: demographics, knowledge assessment, and practice evaluation. Knowledge and practice levels were categorized as good, moderate, and poor using quartiles.
Results:
The study encompassed 168 nurses employed in the emergency department of the hospital, revealing their proficiency in standard practices for preventing hospital-acquired infections. Notably, 63.8% of participants demonstrated a commendable “Good” level of knowledge, while 10.6% exhibited a “Moderate” level and 25.5% manifested a “Poor” level in terms of knowledge. Similarly, concerning practice levels, 56.4% showcased a commendable “Good” practice level, 22.3% maintained a “Moderate” practice level, and 21.3% presented a “Poor” practice level. Chi-square analysis unveiled a significant association between age and knowledge levels (p = 0.000). In addition, age (p = 0.000) and years of clinical experience (p = 0.000) were significantly linked to nurses’ practice levels The nurses aged 40–50 years (82%) and those with 10–15 years of clinical experience (83.3%) showed good levels of knowledge and practice, respectively. Overall, most of the nurses demonstrated effective knowledge and compliance with infection prevention practices.
Conclusion:
Sociodemographic factors such as age and clinical experience exert a notable impact on nurses’ knowledge and practices regarding hospital-acquired infections.
Keywords
Introduction
Globally, the burden of morbidity and mortality of infectious diseases remains high, and deaths attributable to nosocomial infections continue to be a major concern in healthcare settings. These infections, commonly referred to as healthcare-associated infections (HAIs), arise among patients admitted to hospitals for various reasons. HAIs persist as one of the major contributors to morbidity and mortality for both patients and healthcare workers, who experience continuous exposure to diverse diseases through patient interactions, contaminated surfaces, and blood and body fluids. These factors substantially elevate the risk of HAIs.1,2
Nursing procedures can both prevent and contribute to hospital infections. The role of nurses in preventing hospital infections is pivotal. 3 Nursing professionals constitute an integral component of any quality-related program in a hospital, given their oversight and provision of nearly all healthcare services. Consequently, nurses’ knowledge and attitudes play a significant role in healthcare delivery. Studies have shown that continuing education has improved nurses’ professional conduct and knowledge of patient care. Nurses employed across various hospital departments can effectively prevent HAIs. 4 In the prevention of HAIs, nurses require adequate knowledge, skills, and appropriate attitudes. Furthermore, their knowledge is influenced by diverse factors, encompassing their personal and educational backgrounds, training courses, and motivational and managerial elements. Enhanced knowledge, advanced education, and training, along with efficient disinfection and sterilization practices, stand as the most effective approaches to combat and reduce the incidence of HAIs. 5
Despite progress made in healthcare systems, HAIs persist as a substantial threat. The ramifications extend beyond heightened healthcare expenditures to encompass loss of life. While education and knowledge of nurses can effectively curtail the spread of HAIs in emergency departments, other factors can contribute to infection transmission. These factors encompass inadequate supervision and equipment, a taxing workload leading to staff fatigue, poor performance, and insufficient education. Education and knowledge play essential roles in formulating an infection control program aimed at reducing the incidence of HAIs.6,7 This study aims to evaluate the knowledge and practices of nurses regarding HAI prevention in the emergency department of King Faisal Medical Complex in Taif.
Methods
Study design and settings
A web-based single-center cross-sectional study was conducted at the emergency department of King Faisal Medical Complex, Taif from October to December 2022. The study population comprised nurses working in the emergency department, with a total of 168 nurses recruited for participation.
Inclusion and exclusion criteria
Registered nurses actively employed in the emergency department of King Faisal Medical Complex, Taif, were included in the study. Nurses with diverse levels of clinical experience were considered to capture a range of expertise within the department. Participation was voluntary, contingent upon providing electronic consent (e-consent), ensuring participants’ comprehension of research objectives and willingness to partake. Exclusion criteria encompassed nurses from departments other than the emergency department, as the study focused on insights specific to this healthcare setting. In addition, individuals disinclined to participate or on leave during data collection were excluded. Nurses with limited clinical experience, which might affect their contribution to infection prevention insights, were also excluded.
Sample size and sampling procedure
A formal sample size calculation and power assessment were not conducted for this study. Instead, a convenient sampling method was employed, aiming to include all eligible participants from the emergency department of King Faisal Medical Complex, Taif. The study population consisted of registered nurses actively employed in the emergency department, with a total of 168 nurses recruited for participation.
Data collection tool and variable measurements
Participants received an online self-administered questionnaire comprising three main sections. The questionnaire initiation involved gathering sociodemographic characteristics of the study population, followed by knowledge and practice assessment. Response data were treated with utmost confidentiality and managed solely by the principal investigator.
The questionnaire, adapted from Geberemariyam et al.’s study, 8 encompassed three sections. Beginning with sociodemographic characteristics, it proceeded to knowledge assessment, followed by practice evaluation (Supplemental Material). Response data were securely managed by the principal investigator. Geberemariyam et al. 8 reported acceptable internal consistency (reliability) using Cronbach’s alpha test, with values of 0.812 and 0.751 for the knowledge and practice sections, respectively. This tool by Geberemariyam et al. 8 was developed after extensive pertinent literature searches and adopting content from related studies.9–13
Knowledge assessment
In all, 10 binary questions were posed to gauge nurses’ grasp of infection prevention, eliciting “yes” or “no” responses. Furthermore, for analytical purposes, the dependent variables were split into binary outcome variables, where knowledge of infection prevention was coded as “knowledgeable = 1” and “not knowledgeable = 0.” Cumulative knowledge scores, ranging from 0 to 10, were classified into proficiency categories using quartiles: “Poor Knowledge” (lowest 25% of scores), “Moderate Knowledge” (middle 50% of scores), and “Good Knowledge” (upper 50% of scores).
Practice evaluation
Participants responded to five items that assessed their adherence to infection prevention practices using a binary “yes” or “no” format. A standardized scoring approach was employed, assigning a score of “1” for correct practices and “0” for non-compliance. The cumulative scores, ranging from 0 to 5, were then categorized into different practice levels based on quartiles: “Poor Practice” (lowest 25% of scores), “Moderate Practice” (middle 50% of scores), and “Good Practice” (upper 50% of scores).
Statistical analysis
Data were entered into Microsoft Excel and exported to IBM SPSS Statistics version 26, Chicago, IL for analysis. Descriptive statistics were used to calculate the frequency and percentages, while inferential statistics, such as chi-square and regression analysis, were performed to determine the association and impact of the variables of interest. All tests were two-tailed and p-value <0.05 was used as a cutoff point for all statistically significant tests.
Results
There were 55.95% female and 44.05% male respondents. In terms of age, 44.64% were between 25 and 40, 26.79% were between 18 and 25, 20.24% were between 40 and 50, and 8.33% were over 50. In terms of education, 46.43% had a second degree or higher, 17.86% had more than 15 years of experience, 19.05% had 10–15 years of experience, 29.76% had 5–10 years of experience, and 33.33% had less than 5 years of experience (Table 1). In the knowledge assessment, 72.02% of the nurses had heard of infection principles, and 75.59% agreed that gloves cannot completely protect against infection transmission. Almost 64.88% were aware that alcohol-based antiseptic is as effective as soap and water for hand hygiene when hands are not visibly dirty. In addition, 78.57% knew that tuberculosis is carried in airborne particles. Knowledge about the seal and closure of the safety box when it was three-quarters full was observed in 80.95% of the participants, while 67.26% knew about the preparation of 0.5% chlorine solution. These results indicate that the selected nursing participants have good knowledge regarding various criteria for the prevention of healthcare-associated infections (Table 2).
Sociodemographic characteristics of the nursing participants.

Percentages of the correct responses regarding the knowledge of nurses of HAI prevention.

The distribution of healthcare workers across different knowledge and practice levels was analyzed to understand the variations in infection prevention behaviors. In terms of knowledge levels, 63.8% of participants demonstrated a “Good” level of knowledge, 10.6% had a “Moderate” level, and 25.5% had a “Poor” level. Moving to practice levels, among the participants, 56.4% exhibited a “Good” practice level, 22.3% showed a “Moderate” practice level, and 21.3% displayed a “Poor” practice level (Figure 1).
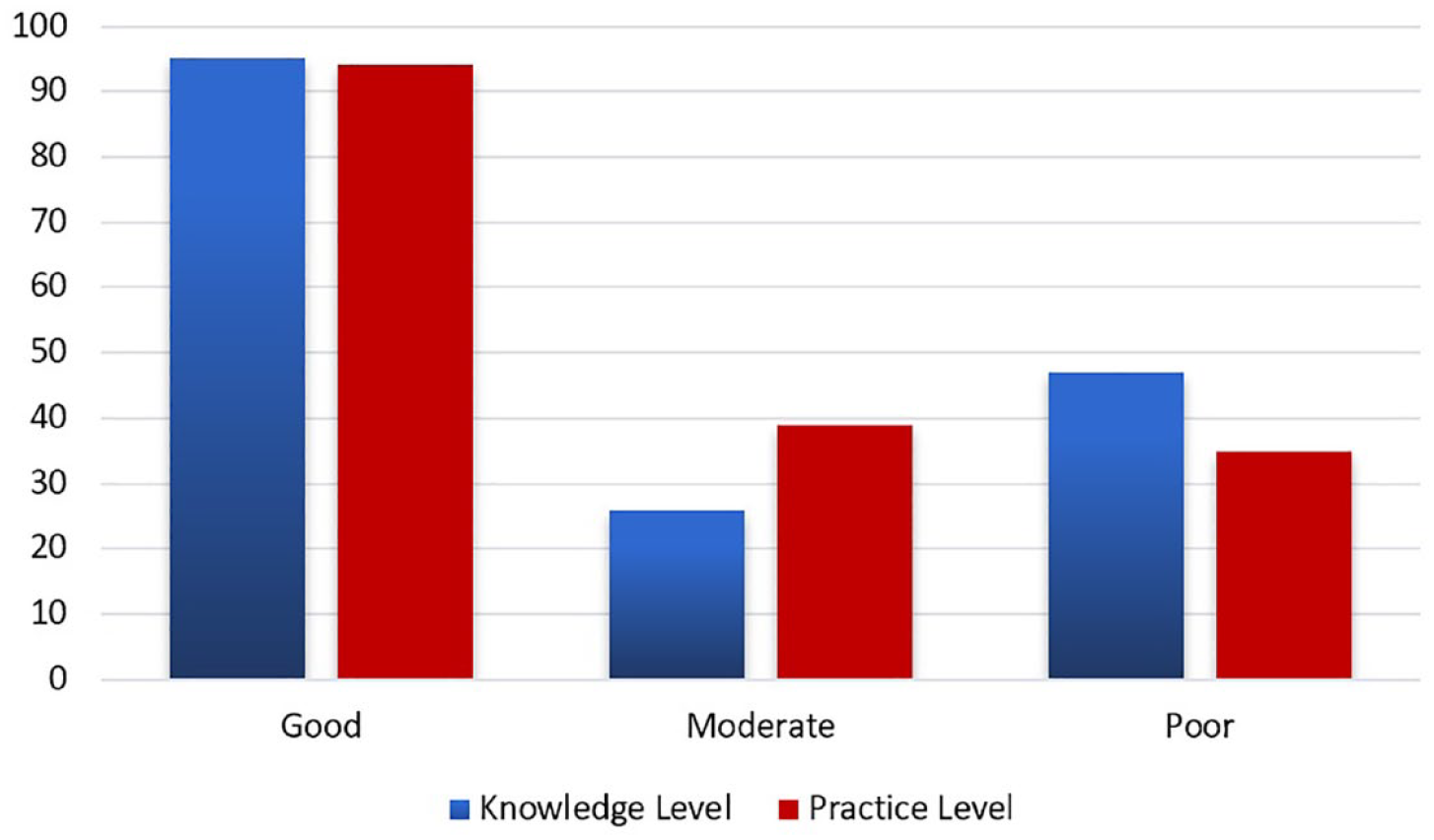
Distribution of knowledge and practice levels of participants.
The results of the chi-square analysis indicate a significant relationship between nursing knowledge and age (p = 0.000). Furthermore, age and years of service are significantly associated with nursing practice levels (p = 0.000) (Table 3). The regression analysis results suggest that nursing knowledge and practice explain 13.9% of the variation in prevention prevalence in the emergency department (Table 4). A high regression coefficient (0.412) and a low p-value (0.000) indicate a positive impact of nursing knowledge on prevention prevalence, while the t-value for knowledge is 4.205 and the standard error value is 0.098. Similarly, the regression coefficient for nursing practice is 0.207 with a p-value of 0.012, indicating a positive impact on prevention and prevalence (Table 5).
The association or impact of the sociodemographic characteristic on the nursing knowledge and practices in the prevention of HAIs.
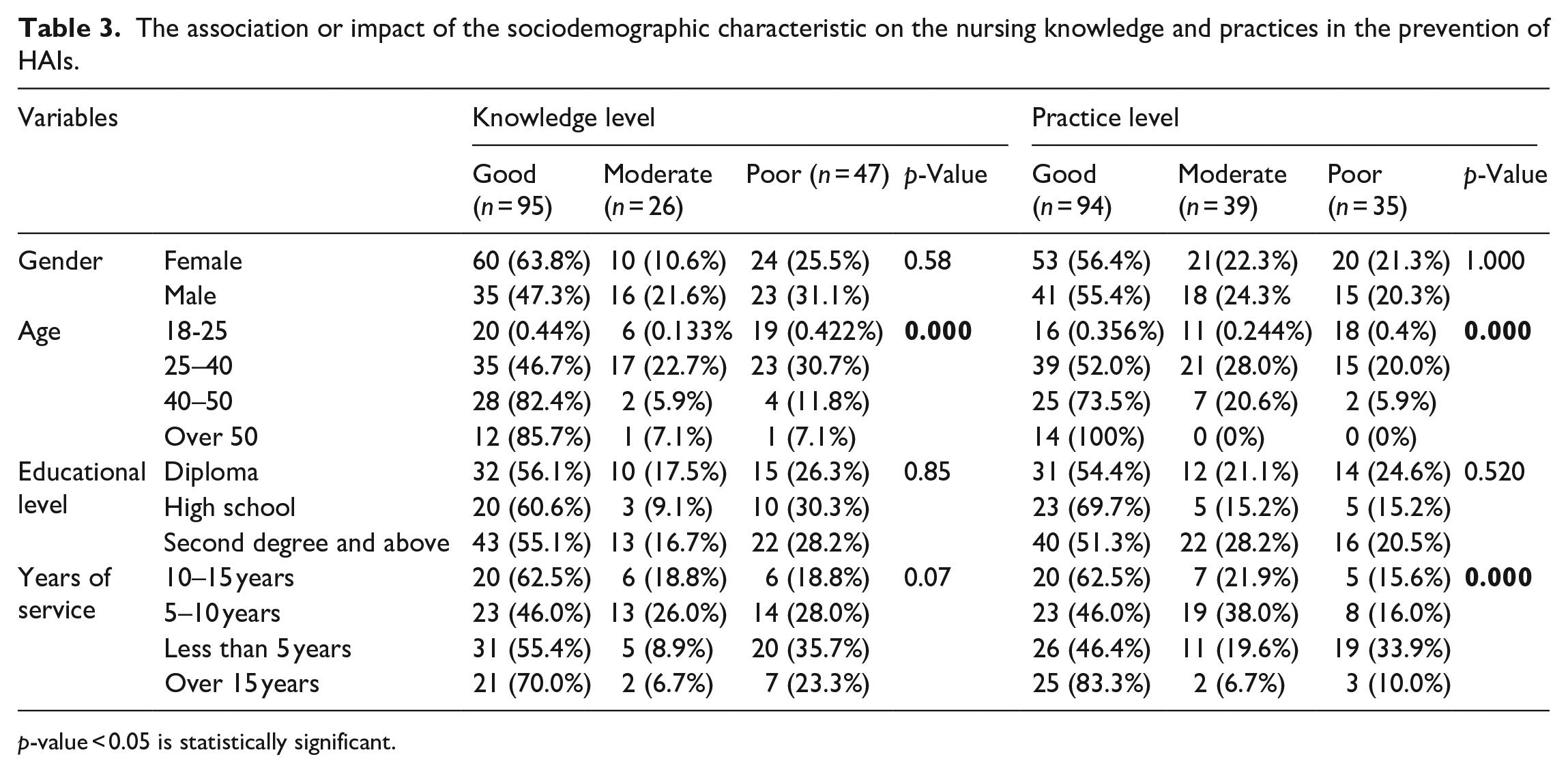
p-value < 0.05 is statistically significant.
Model summary.

Regression coefficient result.

Discussion
The current study aimed to assess the knowledge and practice of nurses in preventing HAIs within the emergency department of King Faisal Medical Complex in Taif, Saudi Arabia. The findings revealed several important insights that can contribute to the understanding of infection prevention efforts among nursing staff.
Globally, more than 2.5 million cases of HAIs occur each year in both developing and developed countries. In high-income countries, HAIs affect 5%–15% of hospitalized patients and 9%–37% of individuals in intensive care units. The prevention of HAIs is achieved through a set of protocols that healthcare workers must adhere to significantly reduce the occurrence and severity of infections. However, adherence to these protocols can be influenced by factors such as a lack of awareness, personal, logistical, or organizational barriers. 14 To establish a safe and hygienic healthcare environment, it is crucial to provide on-the-job training, address skill gaps through training and knowledge sharing among healthcare providers and conduct timely assessments. According to evidence-based studies from the World Health Organization, providing training to healthcare providers significantly prevents HAIs, improves their perception and behavior regarding infection prevention and control, and enhances their implementation of current guidelines.15,16
The present study reveals a commendable level of knowledge among nurses, with a substantial proportion of participants displaying an accurate understanding of control and prevention measures for HAIs. Notably, nurses demonstrated sound knowledge regarding hand hygiene, alcohol-based antiseptics, personal protective equipment usage, and the transmission of infections like tuberculosis. In addition, the pandemic context prompted nurses to adhere to infection control protocols and standardized practices, underscoring the influential role of knowledge dissemination in promoting compliance with HAI control measures among Saudi Arabian nurses. 17 These findings align with Sodhi et al. 18 and Ayed et al., 19 both indicating high infection prevention knowledge levels among nursing professionals. Furthermore, Alhumaid et al.’s 20 systematic review identified satisfactory knowledge levels encompassing standard precautions, hand hygiene, and disease-specific infection prevention and control measures. The demonstrated knowledge underscores the effectiveness of training programs provided to nurses in the emergency department, which is consistent with Farotimi et al., 21 highlighting the positive impact of continuous education on nurses’ adherence to infection prevention protocols.
By contrast, the study by Sisay et al. 22 reported that 45.5% of nurses displayed good knowledge (95%), with 64.8% demonstrating good practices in infection prevention. Our study, on the other hand, identified that 56.55% of healthcare workers possessed good knowledge, while 55.95% displayed good practices. In addition, the research conducted by Mozghan et al. 23 revealed that 41.1% had intermediate knowledge and 33.03% had high knowledge levels, which differed from our study’s categorization of 15.48% with moderate knowledge and 56.55% with good knowledge.
In the study conducted by Bayleyegn et al., 14 90% of participants exhibited both a positive attitude and good knowledge toward HAI prevention, while 57.2% demonstrated a positive attitude. However, when it came to practice, only 36% achieved good practice levels, which is lower than our observed good practice level. The contrast between the positive attitude levels (57%) reported by Bayleyegn et al. 14 and our study’s emphasis on addressing knowledge-attitude gaps might arise from variations in healthcare systems, training approaches, and awareness campaigns across different regions and healthcare settings. These comparisons underscore the necessity of tailoring interventions to consider contextual factors, thereby enhancing infection prevention practices among healthcare workers.
Our findings suggest that nurses with 10–15 years of experience possess significantly better knowledge of HAIs compared to those with less experience. This group of nurses accounted for the largest proportion of knowledgeable participants among our study participants. These results are consistent with another descriptive study of 50 nurses, which found that those with 15–20 years of experience exhibited excellent knowledge of HAI control and prevention. 24 Similarly, a survey-based study of 648 healthcare workers in 2018 indicated that those who had worked in the field for 10 years or more and in facilities with infection prevention committees were more likely to possess knowledge about infection prevention. The authors also noted that healthcare workers who received training and were acquainted with existing infection prevention guidelines were more inclined to report adhering to safe infection prevention practices. 8 However, a cross-sectional study of 271 nurses in 2015 found a negative correlation between years of experience and knowledge of HAIs. In this study, no significant knowledge score was found irrespective of years of experience. 25
Our study also identified age and years of experience as factors influencing the practice level of HAIs. Approximately 73.3% of nurses aged 50 and over and 83.3% of nurses with more than 15 years of experience exhibited good practice levels. These findings align with the results of Asfaw’s et al. 1 study, which demonstrated a positive correlation between work experience and nurses’ practice of HAIs. However, the present study has the potential to show good practices of nurses in relation to their age and years of experience since the practices were inadequate in the nurses studied by Asfaw et al. 1 study.
Positive predictors of compliance include nurse attitudes, a perceived safe environment, and clinical experience. Compliance rates are higher in the intensive care unit department. Ongoing education for nurses, especially in general wards, to improve their knowledge and attitudes should go hand in hand with institutional support for safe environments. 26 In our study, half of the nursing participants reported that infection control training is ongoing in the hospital and that they are aware of the effectiveness of this training program. They also stated that appropriate infection prevention guidelines regarding HAIs are available in the hospital’s emergency department, which indicates strong compliance and adherence to practices. However, a few participants responded negatively to the effectiveness of the training program and compliance with practices.
Our study highlights the importance of assessment of knowledge and practice of nurses in the prevention of HAIs. Also, it provides an elaborate understanding of the role nurses play in this regard which is the strength of our study; however, the present study has certain limitations. Specifically, the study is constrained by its reliance on self-reported data, which could potentially introduce biases like memory recall and social desirability biases that are well-recognized within the field. Additionally, it is worth noting that a sample size and power assessment were not conducted. The study employed a convenient sampling method and included all participants with complete responses. The study did not include a pilot study to refine the research instruments and the questionnaire used was adapted from two previous studies but was not formally validated for this specific context. Furthermore, the study’s design was cross-sectional in nature, thus limiting its ability to establish causal relationships. Moreover, the study was hindered by its relatively small sample size and narrow focus, which restricts its generalizability to a broader understanding of nurses’ knowledge and practices across the entirety of Saudi Arabia. It is important to emphasize that the study exclusively concentrated on nurses within a single healthcare center; in addition, the knowledge of nurses in other domains such as handling and processing of instruments and how this can contribute to HAI were also not assessed and targeted.
To enhance awareness about HAI prevention and underscore the significant role of nurses in this context, comprehensive research studies are imperative. Furthermore, it is recommended that regular on-the-job training sessions be implemented for healthcare workers, with a specific emphasis on nurses. These training sessions should take place every quarter to provide continuous education and augment their proficiency in preventive skills and strategies for HAIs.
Conclusion
In conclusion, this study highlights the commendable levels of knowledge and practice demonstrated by nurses in the emergency department toward the prevention of HAIs. The findings emphasize the pivotal role of nurses in maintaining a safe healthcare environment. Sociodemographic factors such as age and clinical experience exert a notable impact on nurses’ knowledge and practices regarding HAIs. While improvements in both knowledge and practice levels are evident, ongoing efforts are essential to reinforce infection prevention measures. Further research is warranted to explore the effectiveness of interventions aimed at enhancing nurses’ knowledge and compliance, ultimately fostering safer healthcare practices and improved patient outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231222341 – Supplemental material for Assessment of nursing knowledge and practice toward prevention of acquired infections in the emergency department of King Faisal Medical Complex in Taif
Supplemental material, sj-docx-1-smo-10.1177_20503121231222341 for Assessment of nursing knowledge and practice toward prevention of acquired infections in the emergency department of King Faisal Medical Complex in Taif by Fahad Sulaiman Althiyabi, Fares Mabrok Khuded, Fawaz Mohammed Alzaidi, Abdulmjeed Saleh Greeb Alswat, Fahad Suwaylih B Alotaibi, Wael Suwaylih B Alotaibi, Khalid Ibrahim A Alotaibi, Faisal Abdullah H Alshehri, Atallah Mesfer A Almutairi and Jamaan Aali Ahmed Alnathli in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our gratitude to all the participants who willingly contributed their time and insights to this study. Their cooperation was invaluable in gathering the necessary data for our research. We also extend our appreciation to the Directorate of Health Affairs at King Faisal Medical Complex in Taif, Saudi Arabia, for granting ethical approval for this study. Their support in ensuring ethical standards were upheld is greatly appreciated.
Authors contribution
Fahad Sulaiman Althiyabi led the conceptualization, methodology, software, formal analysis, investigation, resources, data curation, writing of the original draft, review and editing, visualization, supervision, project administration, and funding acquisition. Fares Mabrok Khuded contributed to the methodology, validation, formal analysis, investigation, data curation, and writing of both the original draft and review and editing. Fawaz Mohammed Alzaidi worked on software, validation, data curation, and writing review and editing. Abdulmjeed Saleh Greeb Alswat was involved in the methodology, investigation, resources, data curation, and writing review and editing. Fahad Suwaylih B Alotaibi contributed to the conceptualization, resources, writing review and editing, and supervision. Wael Suwaylih B Alotaibi focused on investigation, resources, data curation, and writing review and editing. Khalid Ibrahim A Alotaibi assisted with validation, investigation, data curation, and writing review and editing. Faisal Abdullah H Alshehri contributed to methodology, software, data curation, and writing review and editing. Atallah Mesfer A Almutairi was involved in validation, resources, data curation, and writing review and editing. Jamaan Aali Ahmed Alnathli aided in conceptualization, methodology, writing review and editing, supervision, and project administration. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethical approval for this study was taken from the Directorate of Health Affairs at King Faisal Medical Complex in Taif, Saudi Arabia. The approval number is: 2022-A-04 with registration number: H-02-T-123. The study’s ethical considerations encompassed e-consent, voluntary participation, participant anonymity, data privacy, confidentiality, and adherence to established ethical standards.
Informed consent
The goals and procedures of the study were outlined in a Google form, and all participants provided e-consent before data collection. Participants were informed about the study’s purpose, procedures, potential risks and benefits, and their right to withdraw at any time without consequence. Confidentiality of participant information was assured.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.