
Abstract
Background:
Heavy menstrual bleeding is a common gynecological issue that often requires prompt treatment. Our study aimed to assess thermal balloon endometrial ablation with Foley’s catheter as a viable, cost-effective, and minimally invasive procedure alternative to hysterectomy.
Methods:
An experimental study was carried out on 114 married women experiencing heavy menstrual bleeding who did not wish to have further children and had either failed standard treatments or were not suitable for medical treatment. These women had a uterine size of 12 cm or less and an endometrial thickness of less than 18 mm. A 3-min balloon inflation–deflation procedure was performed. After 3 months, the effectiveness of the treatment was assessed by examining overall heavy menstrual bleeding outcomes, posttreatment transvaginal ultrasound results, number of bleeding days and pain per cycle, and scores from the Menorrhagia Outcome Questionnaire.
Results:
The mean patient’s age was 44.46 ± 4.184 years and a disease duration of 2.84 ± 1.53 years. Most patients were multiparous (86.0%) or grand multiparous (14.0%). Significant improvements were observed in endometrial thickness, Menorrhagia Outcome Questionnaire scores, pain levels, and the number of bleeding days postprocedure (p-value < 0.05). The majority of patients experienced a reduction in the pattern of irregular menstrual cycles. The procedure showed a success rate of 88.6%, with 11.4% of patients not responding. Some further interventions such as hysterectomy or repeated thermal balloon ablation were required due to complications like infection or balloon deflation.
Conclusion:
The thermal balloon endometrial ablation using Foley’s catheter is an effective treatment for heavy menstrual bleeding.
Keywords
Brief summary
A study assessing thermal balloon endometrial ablation with Foley’s catheter as a cost-effective, minimally invasive alternative to hysterectomy was conducted on women with heavy menstrual bleeding. The procedure found a success rate of 88.6%. Further interventions may be necessary due to complications like infection or balloon deflation.
Introduction
Excessive menstrual bleeding is a common concern in gynecology, characterized by the loss of more than 80 mL of blood per menstrual cycle. This occurs when the body sheds the functional layer of the endometrium due to the withdrawal of progesterone in the absence of pregnancy. 1 From menarche to menopause, menstruation plays a crucial role in women’s overall health, impacting their physical, mental, and social well-being. 2 Normal menstruation is described as cyclical bleeding from the uterine body during this period, evaluated based on frequency, regularity, duration, and volume. 3 This condition affects between 10% and 30% of women of reproductive age and up to 50% of premenopausal women. 4 Excessive menstrual bleeding accounts for approximately 12% of gynecological referrals, imposing a significant burden on healthcare services. While many women manage their irregular bleeding with medication, surgery is often considered for those who do not respond to medical treatment. 5 Treating excessive menstrual bleeding requires a significant commitment of healthcare resources. A hysterectomy is usually performed when medical treatments prove ineffective. 6 However, less-invasive surgical procedures have been developed to reduce patient morbidity and healthcare costs. 7
Endometrial ablation (EA) techniques have emerged as a viable alternative to hysterectomy for women with menorrhagia. 8 Since the 1990s, second-generation EA techniques have been developed as simpler, faster, and more effective alternatives to first-generation methods and hysterectomy for treating menorrhagia. Unlike earlier methods, these rely on device design rather than operator skill for safety and efficacy. Though initially raising concerns about increased surgical rates, this minimally invasive approach offers an efficient solution for menorrhagia.9,10 Resection and ablation procedures have lower complication rates and more advantages compared to hysterectomy. Most EAs can be completed in less than 30 min and can be performed with local anaesthesia. Patients who meet the appropriate criteria should be offered this less-invasive alternative for the treatment of their symptoms. 11
However, recent data indicates a decrease in the annual number of hysterectomies and overall surgical procedures in England, alongside an increase in endoscopic procedures. 12 EA using thermal balloons or microwave energy, similar to traditional transcervical endometrial resection or rollerball ablation, is typically performed under general anesthesia as an inpatient procedure. 13
Nevertheless, it is feasible to conduct the procedure on an outpatient basis with the patient awake. The feasibility of this approach is attributed to the simplicity of the technique, its minimally invasive nature, and the shorter postoperative recovery time. Transitioning traditionally inpatient procedures to outpatient settings provides convenience, and potential cost savings, and enhances healthcare capacity. 14 Furthermore, resection and ablation surgeries offer a lower complication rate and are more advantages compared to hysterectomy. Most EAs can be completed in 30 min, in contrast to the typical 1.5 h required for a hysterectomy. 15 Thermal balloon endometrial ablation (TBEA) is commonly carried out under local anesthesia—paracervical block and IV sedation. Patients undergoing EA can typically resume their normal activities the following day. Those eligible for EA should be presented with this less-invasive treatment option for their symptoms. 16 For patients with failed medical treatment for heavy menstrual bleeding (HMB), various nonhysteroscopic endometrial balloon ablation methods exist, but they are effective yet expensive and not readily accessible. This study aims to assess the viability of using a Foley catheter for TBEA as a cost-effective, less-invasive alternative for managing HMB, aligning with our clinical practices and local guidelines. Introducing this approach has the potential to enhance the treatment of HMB.
Materials and methods
The study was conducted in the Obstetrics and Gynecology Department at the University of Lahore Teaching Hospital, Lahore, Pakistan, over 1 year from 2022 to 2023 and approved by the Human Research Ethics Committee at the University of Lahore, Pakistan (IRB/SPRM/2022-3). Written informed consent to participate in this study was provided by the participants. The sample size was determined based on the effectiveness of thermal balloon ablation in patients with HMB as 92% and a margin of error set at 5%, using a 95% confidence level. After taking the written informed consent and explaining the procedure, the patients were enrolled in the study. The participants were aged between 40 and 52 years, married with no desire for further fertility, who had previously failed medical treatment or were contraindicated for it, with no pelvic pathology or underlying medical conditions contributing to the increased bleeding. They also had a uterine size of 12 cm or less and an endometrial thickness of less than 18 mm. Women with a normal endometrium (<5 mm) and no intracavitary lesions on hysteroscopy were included in the study, while those with organic uterine pathology or malignancy, anatomical uterine pathology, active genital/pelvic infection, or abnormal pap-smear results were excluded. After obtaining approval from the hospital’s ethical board, 114 eligible patients were enrolled from the outpatient department. Informed consent was obtained, and demographic data, including name, age, duration of symptoms, parity, hemoglobin (Hb) levels, and HMB score, were recorded.
Thermal balloon ablation procedure
Patients who met the inclusion criteria were admitted to the ward 1 day before the procedure. Before the procedure, general anesthesia was administered, and the patient was placed in a lithotomy. Position—a vaginal examination was conducted to evaluate uterine size and direction, followed by disinfection using povidone-iodine. The cervix was held with a tenaculum and dilated with Hegar’s dilator up to 6 mm. An 18-gauge silicone Foley catheter balloon (30 mL capacity) was used, with the tip trimmed to fit the uterine cavity. The catheter balloon was filled with 30 mL of boiling water at 100°C to ensure its integrity before insertion into the uterine cavity. Gauze pieces were placed between the speculum and vaginal walls to prevent burns. The balloon was inflated with 30 mL of preheated water at 100°C for 3 min, repeated two more times at 1-min intervals.
Procedure follow-up plan
Following the procedure, patients were monitored for short-term complications in the gynecology ward for 6 h and discharged if no active complaints were reported. The posttreatment follow-up plan is designed to track patients’ progress and well-being at specific intervals: 2 weeks and the 12th-week postprocedure. Initially, at the second-week follow-up, patients were checked for any complications, particularly pain and vaginal bleeding, to ensure early detection and intervention if needed. Subsequently, patients returned for a comprehensive evaluation of postoperative adverse effects and complications, such as pain, vaginal bleeding, and changes in menstrual cycle patterns such as amenorrhea, hypomenorrhea, and eumenorrhea. Postoperatively, patients received standard antibiotic prophylaxis, with analgesics administered as needed. Discharge typically occurred on the same day or the following day. Adverse events were documented for each patient intraoperatively, throughout their hospital stay, and at follow-up visits. The effectiveness of the treatment approach was assessed after 12 weeks, which include evaluating total heavy menstrual bleed outcomes, posttreatment transvaginal ultrasound results showing endometrial thickness below 5 mm, reduction in bleeding days per cycle, and pain reduction along with MOQ scores.
Statistical analysis
Data were analyzed using SPSS version 25 (New York, NY, USA). Quantitative variables were presented in mean, and qualitative variables were presented in frequency and percentages. Paired sample t-tests were applied to compare the mean scores of pain, Trans vaginal sonography (TVS) findings of endometrial thickness and MOQ score. The p-value < 0.05 was considered statistically significant.
Results
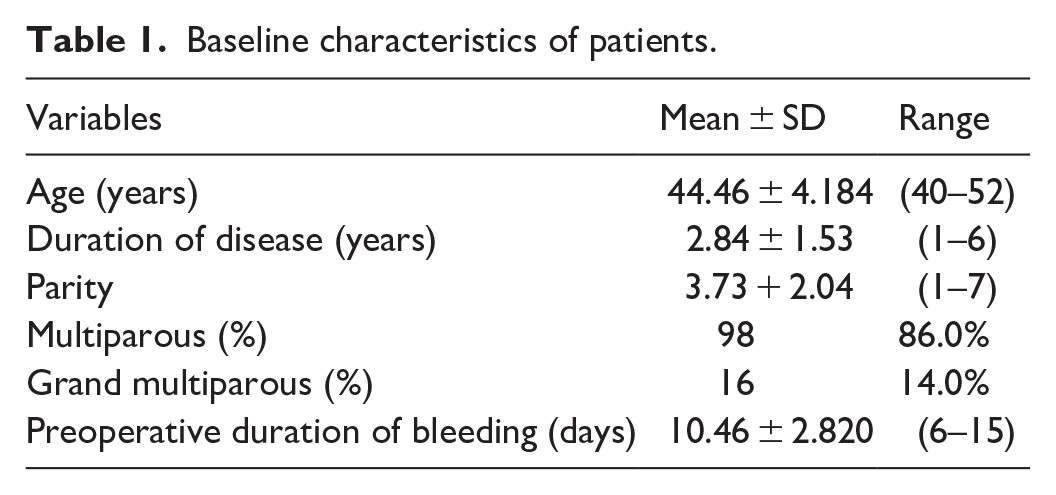
The mean patients’ age was 44.46 ± 4.184 years with the duration of disease as 2.84 ± 1.53 years. Regarding parity, 98 (86.0%) females were multiparous, and 16 (14.0%) were grand multiparous (Table 1).
Baseline characteristics of patients.
The mean Hb levels of patients before endometrial balloon ablation were 9.21 ± 1.80 g/dL, and after the procedure, it increased slightly to 9.48 ± 1.55 g/dL, though this change was not statistically significant (p-value > 0.05). The endometrial thickness showed a significant reduction after a 3-month follow-up, decreasing from 9.24 ± 2.27 mm to 4.41 ± 1.90 mm (p-value < 0.05). Additionally, the MOQ score indicated a significant improvement, with scores decreasing from 91.88 ± 20.03 preprocedure to 50.08 ± 16.99 postprocedure (p-value < 0.05). Patients also reported a significant reduction in pain levels, with scores dropping from 7.46 ± 1.07 to 4.44 ± 1.19 (p-value < 0.05). The number of bleeding days was significantly reduced from 10.46 ± 2.82 days to 5.58 ± 1.07 days (p-value < 0.05). Before the procedure, 71 patients (62.3%) had experienced irregular menstrual cycles, which decreased to 34 (29.8%) females after the procedure (Table 2).
Comparison of pre- and postprocedure outcome variable.

Hb: haemoglobin; MOQ: Menorrhagia Outcome Questionnaire.
Paired sample t-test.
**Chi-square test.
Figure 1 shows the overall effectiveness of Thermal Balloon Ablation (TBA). The procedure was successful and effective in 88.6% of patients, while 11.4% of patients did not respond to the treatment. Figure 2 provides a detailed breakdown of the complications and subsequent interventions following TBA. Notably, 30.7% of patients experienced no complications, indicating a positive outcome for nearly a third of the cohort. However, 23% of patients who did not respond to the procedure ultimately underwent a hysterectomy, while another 23% required a repeated TBA. Additionally, 15.3% of patients reported an infection and needed further treatment, highlighting the importance of postprocedural care. Furthermore, 7.6% of patients encountered initial balloon deflation. These statistics underscore the procedure’s overall effectiveness while also shedding light on the potential complications and the necessary interventions for nonresponding patients.

Effectiveness of thermal balloon ablation.

Complications of procedure.
Discussion
The EA is a minimally invasive surgical procedure utilized to manage HMB. EA specifically targets the endometrial surface of the uterine cavity, effectively addressing HMB that does not respond to medical treatment. This procedure serves as a less-invasive alternative to hysterectomy, offering significant relief to individuals experiencing HMB while preserving the uterus. By either removing or destroying the endometrial lining, EA reduces menstrual flow and often eliminates it, ultimately enhancing the quality of life for patients. Therefore, the current study was undertaken to assess the effectiveness of endometrial thermal balloon ablation in treating HMB. 17
In the current study, the mean age of female patients was 44.46 ± 4.184, with an average disease duration of 2.84 ± 1.53 among those experiencing HMB. In terms of parity, 98 (86.0%) of the females were multiparous, while 16 (14.0%) were grand multiparous. Referrals related to menstrual disorders make up roughly 20% of all specialized gynecology consultations in theUnited Kingdom. 18 In the current study, it was observed that 23% of patients who did not respond to the procedure eventually underwent a hysterectomy. In the literature, a primary reason for the high rate of hysterectomy following EA in the current study was the technical limitations of the procedure, such as incomplete ablation and difficulty accessing all areas of the endometrium, which often led to persistent symptoms. In cases where patients remained unsatisfied, hysterectomy was often the next step, either due to procedural failure or patient preference to forgo other conservative options. 19 However, in the literature, it was reported that initially, EA was anticipated to serve as a replacement for hysterectomy in cases of dysfunctional uterine bleeding (DUB). However, Bridgman and Dunn’s analysis of UK hospital data from 1989–1990 to 1995–1996 revealed that EA did not lead to a significant reduction in hysterectomy rates. 20
These results align with previous research indicating that HMB accounts for approximately half of all hysterectomies performed. According to the Royal College of Obstetricians and Gynecologists of theUnited Kingdom, 42% of hysterectomies in the United Kingdom are carried out to address DUB. 21 Among the respondents, 23% had repeated TBA procedures. Furthermore, 15.3% of patients experienced infections requiring additional treatment, underscoring the significance of postprocedural care in the current study. Nonetheless, infections occur infrequently, and the use of antibiotic medication is a common practice to reduce the risk of endometritis. 22 Prophylactic antibiotics are essential for lowering infection risks during EA, as these procedures can introduce bacteria and induce problems such as endometritis. Proper aseptic procedures can reduce infection rates, but antibiotic prophylaxis is particularly important for high-risk patients. The selection and timing of antibiotics are critical factors affecting the success of prophylactic measures. 23
We also observed a significant decrease in bleeding days, from 10.46 ± 2.82 to 5.58 ± 1.07 days (p-value < 0.05). Furthermore, the percentage of patients with irregular menstrual cycles decreased from 62.3% (71 patients) to 29.8% (34 patients) postprocedure. Another study has reported a reduction in the interval between cycles and a sustained improvement in dysmenorrhea rates at follow-up periods of 12, 24, and 36 months. This method was consistently maintained to achieve highly satisfactory outcomes and effectiveness in reducing abnormal menstrual bleeding in a separate trial at a 3-year follow-up (89.1%). 24 Another study focused on the decrease in blood flow following modified thermal balloon ablation, revealing that 75% of participants experienced normalized menstrual flow after 1 month, which decreased to 36.36% at the 3-month follow-up. 25
In our study, the success rate of TBA was 88.6% which is higher than the previously conducted study involving 121 women with DUB who underwent Endometrial Balloon Ablation reported a 68% response rate, with 82 women providing a good response. However, in the other study, the success rate reported for thermal balloon ablation ranged from 80% to 97% and 89.1% of their subjects were satisfied with the surgery as shown by a decrease in days of menstrual flow each cycle. 26 There was also a significant improvement in the MOQ score, clearly seen in our study, with scores decreasing from 91.88 ± 20.03 preprocedure to 50.08 ± 16.99 postprocedure (p-value < 0.05), indicating satisfaction with the procedure and improved quality of life. These results align with a 6-year retrospective study done by Vitale et al. 27 where 76% of the 152 women assessed were satisfied with the treatment, 14% experienced amenorrhea, and 54% had eumenorrhea. They concluded that women over 40 with heavy but regular menstrual cycles benefit the most from TBEA therapy due to its good long-term efficacy.28,29
The TBA is now successfully used to treat not only HMB due to DUB but also to reduce bleeding from fibroids. Recent studies have demonstrated the effectiveness of TBA in reducing symptoms associated with fibroids.27,30,31
The effectiveness of the treatment approach was assessed after 12 weeks, which include evaluating total heavy menstrual bleed outcomes, posttreatment transvaginal ultrasound results showing endometrial thickness below 5 mm, reduction in bleeding days per cycle, and pain reduction along with MOQ scores. TBEA is a minimally invasive procedure designed to help premenopausal women with HMB by reducing the thickness of the endometrial lining. This technique promotes thinning of the endometrium and reduces the duration of menstrual bleeding. Factors such as the patient’s age and uterus characteristics can influence the success rates of TBEA. The long-term effectiveness of TBEA is impressive, with some studies showing sustained positive results for over a decade. However, younger patients or those with severe dysmenorrhea may need additional interventions in the future, such as a hysterectomy, compared to older patients nearing menopause. This highlights the need for personalized treatment options for HMB.32,33
In this study, the balloon is inflated with 30 mL of preheated water at 100°C for 3 min, with two additional cycles of 1 min each, effectively reducing endometrial lining thickness for HMB. The study by Ibrahim et al. reported the use of 5% dextrose in water at 87°C for 8 min, highlighting a similar duration. 25 Generally, thermal balloon ablation is recommended for 8–10 min, depending on the technique and fluid temperature to ensure effective ablation of the endometrial lining.34 –36
The study on Foley catheter ablation includes limitations, such as potential bias from patient selection and the lack of a control group. The modest number of patients included may reflect thorough selection, but compliance is also important. The lack of evidence regarding long-term follow-up or a lack of a control group weakens the ability to directly attribute the outcomes to Foley’s catheter ablation rather than other factors. We believe that a bigger trial with more patients and longer follow-up periods will yield a more comprehensive outcome, including potential late problems. Also, recommend prolonging the follow-up time to ensure a thorough comprehension of the technique.
Conclusion
TBEA utilizing Foley’s catheter is a cost-efficient method for addressing abnormal uterine bleeding. This technique serves as a secure, economical, and efficient substitute for hysterectomy in managing HMB. Its simplicity makes it a valuable option, especially in environments with limited resources, given its cost-effectiveness. With a notable success rate and a favorable safety record, marked by the absence of significant complications, this procedure instils confidence and can be readily integrated into future medical practices. It is essential to conduct additional research with an extended follow-up period to derive more substantial conclusions regarding this procedure.
Footnotes
Author’s contribution
Khalid Khadawardi was involved in Project designing. Hisham Nasief participated in manuscript writing. Amber Hassan was involved in data collection and result analysis. Yasir A Katib was part of finalizing the results and data analysis. Nashwa Aldardeir participated in the manuscript preparation. Ahmad B Alwazzan was the leading person in proofreading and finalizing. All authors contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
The studies involving human participants were reviewed and approved by the Human Research Ethics Committee at the University of Lahore, Pakistan (IRB/SPRM/2022-3).
Informed consent
Written informed consent to participate in this study was provided by the participant’s. Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.