
Abstract
Background:
Laboratory testing plays a critical role in healthcare decision-making; however, concerns regarding overutilization and inappropriate testing persist. Minimum retesting intervals serve as a tool to optimize testing practices and resource allocation. This study aimed to assess adherence to minimum retesting interval guidelines and estimate associated costs for commonly prescribed tests, namely HbA1c, 25 hydroxyvitamin D (Vitamin D), and thyrotropin, in a university hospital setting in Nepal.
Methods:
This observational study utilized secondary data from medical records covering 1 year. Adherence to minimum retesting interval guidelines was evaluated based on established recommendations, and the economic burden of inappropriate testing was estimated using cost data provided by the Health Insurance Board of Nepal.
Results:
Patients who underwent TSH, HbA1c, and Vitamin D testing during the study period were 27,960, 8558, and 5416 with the total number of tests being 38,718 TSH, 13,859 HbA1c, and 5977 Vitamin D, respectively. There were notable proportions of patients with minimum retesting interval breach, that is, n = 1317 for thyroid stimulating hormone (4.71%), n = 1159 for HbA1c (13.54%) and n = 232 for Vitamin D (4.28%). Minimum retesting interval breaches were identified across all parameters, with associated costs of $12,817 which could be saved if there were no minimum retesting interval breaches. Variations in minimum retesting interval adherence were observed between insured and noninsured patients and among tests falling within and outside reference ranges.
Conclusion:
The findings highlight the prevalence of minimum retesting interval breaches and inappropriate testing practices, emphasizing the need for interventions to optimize laboratory testing utilization. Addressing these challenges through context-specific strategies can enhance resource allocation and patient care while mitigating financial burdens.
Keywords
Background
Laboratory testing is a vital aspect of modern diagnostics and disease management, with healthcare decisions relying heavily on the results of these tests. 1 According to recent estimates, as much as 70% of healthcare decisions are based on laboratory test results. 2 However, the increasing use of laboratory tests has raised concerns about cost control and appropriate resource allocation in healthcare. 3 The high number of diagnostic tests being prescribed worldwide suggests that the issue is not solely due to an increasing population morbidity rate but also the inappropriate use of these tests. Studies have revealed that a substantial portion of laboratory tests, ranging from 23% to 67%, are deemed inappropriate. 2
To address the issue of laboratory overutilization, laboratory professionals have explored interventions aimed at optimizing the use of laboratory testing. 4 Educational strategies and administrative approaches have been employed to reduce inappropriate testing. One such intervention proposed is the implementation of minimum retesting intervals (MRIs) within the laboratory order entry system. This approach aims to manage inappropriate retesting and contributes to sustainable demand management. 5 MRI serve as an effective tool for managing laboratory test utilization. MRI refers to the minimum time required before a test should be retested based on the test’s properties and the clinical situation. 6 The Association for Clinical Biochemistry and Laboratory Medicine (ACB) and the Royal College of Pathologists have provided recommendations for MRI implementation, defining optimal MRIs for various laboratory tests based on evidence-based guidelines and best practices. 7
Glycated hemoglobin (HbA1c) assay is a commonly performed standard laboratory test for long-term glycemic control assessment and correlates with long-term diabetes complications. 8 There has been undeniable evidence that HbA1c is being inappropriately retested in clinical practice. HbA1c concentrations of 5.7%–6.4% indicate individuals at high risk of developing type 2 diabetes mellitus. Repeat HbA1c testing is not required for persons with results in this range. 9 Clinical laboratory professionals will have a vital role in implementing ordering procedures in conjunction with clinicians. 10 Studies related to retesting for HbA1c have shown variable results. An Australian study highlights that better adherence to guideline-recommended HbA1c testing frequency was associated with better glycemic control and lower risk of Chronic Kidney Disease (CKD) with a finding suggesting an overall adherence of only 50%, with the median testing frequency of 1.6 tests per year, which was less than the recommended frequency (i.e., at least 2 tests yearly). 11 Although studies examining HbA1c testing frequency in line with clinical guidelines in patients with type 2 diabetes are limited, low adherence rates and low testing frequency in the population have been suggested by some studies.11,12 In contrast to this, a UK study showed that >50% of all tests are requested outside recommended monitoring intervals (21% too soon; 30% too late). 13 This strappingly raises questions as to the implications of inadequate, excessive, or inappropriate monitoring, on both clinical and economic endpoints. 14
A new dawn in nutritional clinical biochemistry has been the utilization of vitamin D tests in numerous clinical conditions, but majorly for the maintenance of musculoskeletal health. 15 Similarly, significant associations of vitamin D have also been made with increased risks for hypertension, type II diabetes, cardiac diseases, respiratory disorders, and different cancers. 16 Hence, it has been a widespread practice as both workups for certain medical conditions and symptoms and as part of routine health maintenance for testing and treating optimum vitamin D levels. Data from the Third National Health and Nutrition Examination Survey has revealed that the prevalence of vitamin D deficiency and insufficiency is >50% among children and young, middle-aged, and older adults. 17 The minimum retesting interval for vitamin D is 3 months as per the guidelines. Retesting vitamin D <1 month after initiating treatment may give a false picture of under or over-repletion. 15
For thyroid-related disorders, medical history, physical examination, and thyroid imaging, laboratory tests are fundamental segments for screening, diagnosis, and management of thyroid disorders. 18 One common test for the screening of thyroid disorder is thyroid-stimulating hormone (TSH). TSH has a MRI of 4 weeks. 19 A Dutch study reported that 14.2% of the requests for TSH could be saved if the MRI protocol was meticulously followed.19,20 In addition, large cohort studies from Canada and Italy reported comparable rates of inappropriate utilization for TSH being 7%–8%.21,22
Since the introduction of the National Health Insurance program, the overall number of biochemical tests conducted at Dhulikhel Hospital has noticeably risen. Our study aimed to investigate this scenario of minimum retesting intervals by concentrating on three commonly prescribed tests: HbA1c, vitamin D, and thyrotropin (TSH). Specifically, the study aims to assess adherence to MRI guidelines, identify any breaches in retesting intervals, and estimate the associated costs. These tests were chosen because they are frequently prescribed and have experienced a significant increase in usage over the past few years, particularly in nonacute settings.
Methodology
This is an observational, hospital-based secondary data analysis (Audit) focusing on compliance with MRIs and the economic burden of the tests. This study utilized medical records extracted from the Hospital Information Management Software (Midas) of Dhulikhel Hospital, one of the largest tertiary care centers of Central Nepal for a period of 1 year from October 2022 to September 2023. We have obtained the ethical clearance from the Institutional Health Research Ethics Review Committee Kathmandu University School of Medical Sciences (KUSMS) with the reference number: IHRERC/3688/22 KUSMS.
Inclusion criteria
The inclusion criteria encompassed patients who underwent HbA1c and/or vitamin D and/or TSH tests within the specified time frame.
Exclusion criteria
Data that were not present in the medical record were excluded.
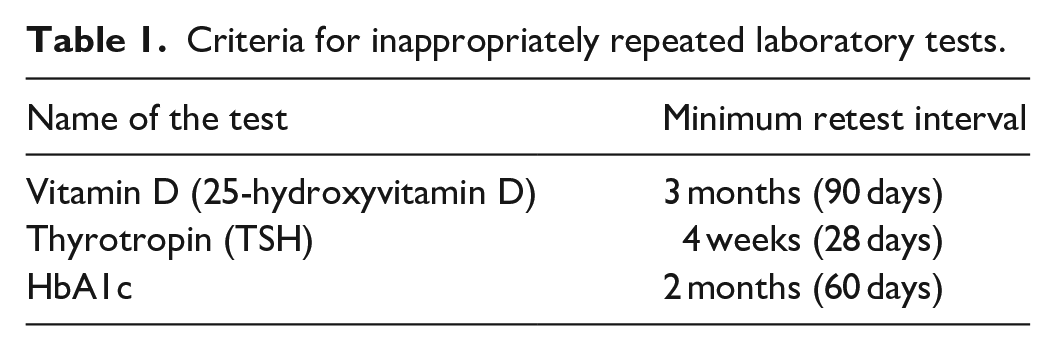
TSH and vitamin D was estimated by chemiluminescence immunoassay using ARCHITECT i1000SR from Abbott Laboratories (Abbott Park, IL)/DiaSorin LIAISON®XL (DiaSorin S.p.A., Saluggia, Italy) and HbA1c by high performance liquid chromatography using D-10 hemoglobin testing system by BIO-RAD. We strictly adhered to the standard recommendations for MRIs in Clinical Biochemistry, which was developed by the Association for Clinical Biochemistry and Laboratory Medicine and are supported by the Royal College of Pathologists, 7 as provided in Table 1. To calculate the economic burden, we utilized the cost of the tests as provided by the Health Insurance Board of the Nepal government (Table 2).
Criteria for inappropriately repeated laboratory tests.
Cost of the tests as per the Health Insurance Board of the Nepal government.

Statistical analysis
Data were entered in Microsoft Office Excel 2013 XLL and analyzed with Statistical Package for Social Sciences version 21.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics was utilized to summarize the data and provide an overview of key variables. Data were expressed in terms of percentages and frequency distributions.
Results
During 1 year, 27,960, 8558, and 5416 patients underwent TSH, HbA1c, and vitamin D with a total number of tests, that is, 38,718 for TSH, 13,859 for HbA1c, and 5977 for vitamin D, respectively. Out of these, the number of patients who repeated the tests was 6335 (TSH), 2995 (HbA1c), and 486 (vitamin D), while the number of patients with MRI breach were 1317 (TSH), 1159 (HbA1c), and 232 (vitamin D), respectively, as shown in Table 3. Over 1 year, the highest TSH retesting occurred in two patients with 13 retests. Similarly, one patient had a maximum of 19 HbA1c retests, while two patients underwent a maximum of five vitamin D retests each. The number of retested parameters for each patient, along with the total number of patients is presented in Table 4.
Total number of patients tested and number of patients with MRI breach.

Repetition of TSH, HbA1c, and vitamin D.

Analysis of appropriate testing practices revealed that the majority of TSH (91.1%), HbA1c (80.4%), and vitamin D (73.4 %) tests were deemed appropriate. Taking account of the retested parameters, 3430 (13%) were inappropriate based on MRI guidelines. The total number of inappropriate tests among the repeated tests amounted to 3430 out of 26,436, representing 12.97% of the total. Among the total repeated tests, the median value of TSH and 25-OH vitamin D were 2.92 (1.62, 4.76) and 22.7 (15, 32.8), respectively. Similarly, the mean value of HbA1c was 7.22 ± 1.68. The difference between MRI breach and appropriate testing of TSH, HbA1c, and vitamin D has been shown in Table 5.
Descriptive analysis of the laboratory parameters among inappropriate retesting and appropriate testing among the laboratory parameters.

Among the tests that breached the MRI, 8.7% of TSH, 19.3% of HbA1c, and 21.3% of vitamin D showed results outside the reference range. However, a greater proportion of the test results (9% TSH, 23.4% HbA1c, and 38.5% Vitamin D) that fell within the reference range was also found to breach the MRI guidelines which was statistically significant (Table 6). Comparison of the test parameters within and out of the reference range with and without MRI breach, we found that there was a significant difference in the MRI breach in HbA1c and vitamin D (p ⩽ 0.05) as depicted in Table 6.
Difference in MRI breach among the test parameters within and out of reference range.

Regarding the insurance status, an MRI breach was observed in insured and noninsured patients. A total of 8.5% of insured patients and 9.7% of noninsured patients showed MRI breaches in TSH tests, whereas 19.4% of insured and 20% of noninsured patients exhibited MRI breaches in HbA1c tests. Similarly, an MRI breach was observed in 25.6% of the insured and 30.3% of the noninsured patients in the vitamin D tests (Table 4). Out of the total repeated tests, 18,340 out of 26,436 (69.37%) were covered by insurance. In total, among those tests covered by insurance, 2340 out of 18,340 (12.75%) were considered inappropriate. Comparing the MRI breach among the insured and noninsured test parameters showed that there was a significant difference (p <0.01) between TSH (insured vs noninsured) as shown in Table 7.
MRI breach among insured and noninsured test parameters.

p value < 0.05 is considered to be statistically significant.
Among the insured patients, 11,712 (68.5%) TSH, 5809 (70%) HbA1c, and 819 (78.2%) of Vitamin D were retested. In contrast, among noninsured patients, frequency of retesting was much lower as shown in Figure 1.

Frequency of insured and noninsured tests among MRI breaches in laboratory parameters.
The financial consequences of inappropriate testing were considerable. The overall expense related to MRI breaches amounted to $12,817, with TSH tests accounting for $3536, HbA1c tests costing $6128, and vitamin D tests costing $3153. The total cost incurred for MRI was 6.13%. The individual costs incurred from MRI for TSH was 3.95%, HbA1c was 11.79%, and vitamin D was 4.68% as shown in Table 8. Additionally, the financial burden was not evenly distributed between insured and uninsured patients across all tested parameters (Figure 2).
Total cost per test in 1 year and cost of MRI breach for the test parameters.


Cost (in US$) associated with inappropriate testing among insured and noninsured patients.
Discussion
Laboratory testing plays a pivotal role in healthcare decision-making, yet concerns surrounding overutilization and inappropriate testing persist leading to rising healthcare costs and resource allocation challenges. 23 MRIs continue to be a successful demand management tool to assist in identifying and reducing inappropriate testing. Our study delineated that 12.97% of the repeated tests were inappropriate according to MRI guidelines. This finding is similar to the study reported from a Croatian University hospital in which 14.8% of the requests contravened the MRI rule. 2 While the proportion is lower than the study reported from Turkey (16.2% vs 12.97%). 7
Similarly, a report by Lang 23 constituting the studies done from 2011 to 2020 showed that 11.8% of the tests failed the defined MRI recommendations. 23 The review concluded their findings as MRI being a popular and established demand management solution for identifying and reducing overutilized tests and aligned with our study. In the same hospital settings, all of them are tertiary, and university hospitals could be the cause. Most of the tests were ordered by junior physicians and interns, who are constantly switching places. Moreover, inappropriate testing can result when several doctors in different departments order the same test because there is no information system to verify if another doctor has ordered it. 23
Out of all the tests that were analyzed, 46.55% were within the reference range, and among the tests within the reference range, 1284/12,308 (10.43%) were inappropriate. A total of 69.37% of the total number of repeated tests had insurance coverage. A total of 12.75% of those tests were deemed inappropriate. Since there is a lack of any national guideline for test repetition in Nepal, the physicians would request tests whenever it seem suitable. The insurance coverage removed the financial burden from patients along with financial accountability while testing. This has resulted in repeated testing that violated MRI. Inappropriate testing had significant cost repercussions. The total cost associated with MRI breaches was approximated to be Nepalese Rupees (NPR) 1,708,389.47 ($12,817) for 1 year.
Our research findings are similar to those reported by Hueth et al. 24 from the University of Utah, which reported that 44% of repeated tests were potentially unnecessary repeat testing (PURT). They estimated that the annual cost of this PURT was $37,376/year. They found that 26% of providers ordered PURT, but most (69%) of PURT was due to relatively few (10%) providers. 24 Irrational use of laboratory services including overutilization of tests can exert detrimental effects that can directly raise the costs beyond the direct cost of the test. 24
Also, unwarranted investigative work-ups increase patient safety risks and do not pose any diagnostic certainty. 25 Gratuitous testing leading to negative clinical outcomes is commonly seen in Iatrogenic anemia, 26 increased length of stay and unplanned readmission, 27 patient discomfort 28 (i.e., frequent phlebotomies and sleep interruptions), and patient dissatisfaction. 29 These negative effects are contrary to the aims of US health care systems, and limiting them presents a greater value than solely that of direct cost savings. 25
We have analyzed the MRI for three commonly done analytes in our setting, that is, TSH, HbA1c, and vitamin D. Our findings depict that an MRI breach for TSH was found in 8.9% of total tests done. This was in line with the study reported from Canada 30 which has highlighted the ordering of TSH was deemed inappropriate in most of the requisitions. They reported that almost 91% of the primary care physicians who ordered one or more TSH tests ordered at least one inappropriately, and around 6% of all TSH tests ordered by primary care physicians were inappropriate. 30 Similarly, Morgen and Naugler 31 have reported that the percentage repeated inappropriately (95% CI) for TSH was 7.2 (7.0–7.3) with the recoverable internal cost of each test for the study laboratory Canadian Dollars (CAD) being $1.00–$5.00 and the annualized cost of inappropriate repeats at the study laboratory (millions) was $0.04–$0.19, respectively. 21 We report an interesting finding that 9% of the patients who violated the MRI had the TSH within the reference range similar to the one that was outside the reference range (8.7%). There might be various factors influencing this scenario. A few of the reasons could be pediatric patients, patients who are pregnant, and those with overt hyperthyroidism, people in perimenopause or menopause, or those taking hormone therapy (e.g., people who are transgender). 32
We found that 19.6% of HbA1c tests were inappropriate based on MRI guidelines. This was in accordance with the study reported by Chami et al. 21 (17.75%). Veterans’ administration health system in the United States found that 30% of patients being followed for diabetes had repeat HbA1cs done within 90 days of a previous test. 33 Our study findings show that the MRI breach (<90 days) for vitamin D was found to be 26.6%. This was slightly lower than a study reported by Dar and Ibrahim from Saudi Arabia which reported that retesting of MRI within 3 months was 20.3%. 15 One study 15 has provided a strategic analysis where the cost of the tests was displayed in real time when the general practitioners (GPs) were ordering the tests, and it achieved insignificant results. 15 The strategic analysis has shown variable results. Some studies have reported that displaying the cost of the tests led to a decrease in the ordering of tests,34–36 while another author concluded the contrary. 37 Displaying costs on the GPs requisition form is still sparsely investigated, but GPs tend to use more common and cheaper tests compared to hospitals, which tend to request the majority of special and expensive tests. It is therefore likely that this intervention might have only a minor effect on the requesting patterns of GPs. 15
If the test sets were increased in number, more savings would probably be possible. A study done in a tertiary care hospital in Turkey showed that the statistics can be extrapolated to the national level, resulting in an estimated yearly waste of US$3 million on unnecessary repeat testing. 7 Research conducted in Italy revealed that retesting of potentially inappropriate samples was carried out for tests where there was a minimum of 8.1% (1,25-dihydroxy vitamin D) and a maximum of 37.1% (total cholesterol). The estimated loss of money during the 3 years was €500,000. According to our analysis, there is no indication of a declining trend and economically unreasonable rates of incorrect retesting. 23 Not only may improper utilization of laboratory tests cause harm to patients, but it can incur needless extra expenses.
Our investigation used a comparatively small number of tests conducted at a single university hospital. As a result, our results might not be generalized to other settings. Since our practice still uses a traditional requisition sheet, we were unable to identify the test requestor for the improper tests. The majority of the requisition forms did not have details regarding the prescriber’s name, title, or department. This has limited the intervention implications significantly as it is highly challenging to determine the requisition pattern associated with the specific group of clinicians.
The next logical step would be to create MRIs that are universally acknowledged and made public. It may be helpful to establish a Laboratory Stewardship Committee to reduce the inappropriateness of laboratory requests by examining the causes and working together with laboratory experts and doctors. Interventions to decrease needless laboratory testing have been implemented and studied in various clinical settings across numerous nations. These interventions include educational sessions or posters, pop-up reminders upon test ordering through an electronic ordering system, modification of paper order forms, and giving clinicians insight into their ordering patterns.
Few studies have determined the effect of implementing MRIs on the amount of laboratory testing and direct financial savings. A study reported by Boerman et al. 38 from a Dutch Hospital delineated that MRI alerts offer a continuous reminder for physicians to use diagnostics appropriately and can be used to create awareness. They have highlighted that the use of MRIs should be considered to improve the appropriate use of laboratory tests, but the potential impact of these alerts in each hospital strongly depends on the overuse of laboratory testing before implementation, the position of the laboratory in the hospital, and the clinical care setting. 38 A South African study reported by Smit et al. 39 has highlighted the use of electronic gatekeeping (eGK) implementation in the laboratory has a beneficial effect on patient care. They have shown that eGK is an effective method of reducing unnecessary test requests and effectively managing demand.
Limitations
This study has a few limitations. This was a hospital-based study conducted over 1 year; hence, we did not have any provision for definite sample size calculation. The study relies on administrative data from the software medical record. Thus, no clinical information surrounding the tests could be substantially recruited. It is therefore not possible to evaluate whether a laboratory test is clinically relevant, nor to evaluate potential risk factors associated with inappropriate use of tests. Since we included all the test data during the study period. We did not calculate the sample size.
Conclusion
In conclusion, our study depicted a substantial number of tests that were repeated within intervals shorter than recommended, indicating MRI breaches in our university hospital. These highlight potential gaps in adherence to established guidelines and suggest the need for interventions to optimize testing practices. Furthermore, the financial implications of MRI breaches were considerable, emphasizing the importance of effective utilization strategies in healthcare resource management. The findings suggest that addressing inappropriate testing practices through interventions like MRI implementation can lead to significant cost savings and improved resource allocation.
Footnotes
Acknowledgements
The author would like to acknowledge Dhulikhel Hospital, the IT department, and special thanks to the laboratory staff of clinical biochemistry for their help during the study.
Authors’ contribution
TS: Conceptualization, study design, execution, acquisition of data, analysis, and interpretation; HM: study design and execution; TB: execution, acquisition of data; NA: Data analysis and interpretation. All authors took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, and agreed on the journal to which the article was to be submitted.
Data availability statement
All relevant data that support the findings of this study are included in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee with the reference number of IHRERC/3688/22 Kathmandu University School of Medical Sciences (KUSMS).
Informed consent
Informed consent was not applicable to this study. The information obtained from patient medical record cards was kept confidential, and the name of the patient and other information that specifically identified the patient were not recorded. This information was included in the research proposal.
Trial registration
Not applicable.