
Abstract
Objective:
The aim of this work was to estimate cost-effectiveness of five common procedures for varicose vein surgery (high ligation and stripping, radiofrequency ablation, endovenous laser ablation, steam vein sclerosis and cyanoacrylate glue) in a Norwegian setting from both a societal and a healthcare payer perspective.
Design:
Cost-effectiveness analysis using decision tree modelling.
Methods:
A structured literature search was conducted to estimate the clinical effectiveness and the rate of complications in the five methods. Data on costs and health-related quality of life associated with varicose vein disease were also collected. With the aid of an expert panel, a structured decision tree was developed. A 1-year perspective was modelled, and a variety of common complications were included. Monte Carlo simulation was used for probabilistic sensitivity analyses.
Results:
The laser ablation strategy was the most cost-effective option from a societal perspective, with an incremental cost-effectiveness ratio of €8448 compared to a no-treatment alternative, and had a 42% probability of being cost-effective using the Norwegian willingness-to-pay threshold of €59,880. From a healthcare payer perspective, however, the steam vein sclerosis strategy was the most cost-effective with an incremental cost-effectiveness ratio of €4072 compared to a no-treatment alternative, and this strategy had a 50% probability of being cost-effective.
Conclusion:
Results from this study did depend upon the perspective chosen for analyses. Although recent endovenous surgical procedures (including laser ablation and steam vein sclerosis) provide clinically effective treatment for advanced, symptomatic varicose vein disease, availability of high-level data is currently limiting the cost-effectiveness analyses.
Keywords
Introduction
Endovascular techniques for treating varicose vein disease provide benefits, such as reduced invasiveness, less postoperative pain and shorter sick leave, compared to traditional open high ligation and stripping (HL/S).1,2 These advantages, however, should be weighed against associated costs of equipment and resources in order to gain a more complete understanding of their impact.1,3,4 Such cost-effectiveness assessments can provide important information in decision-making and policy settings. A recent example is a German study investigating the impact of reimbursement of a radiofrequency ablation (RFA) procedure for varicose veins. 5 The results of the analysis indicated that a general reimbursement of the procedure through the German Statutory Health Insurance could lead to cost saving for the healthcare sector.
To date, relatively few studies have made comparisons of costs and outcomes across varicose vein procedures.6,7 A recent health technology assessment (HTA) sponsored by the National Health Service (NHS; United Kingdom) developed a model for comparing the strategies of HL/S, RFA, endovenous laser ablation (EVLA), ultrasound-guided foam sclerotherapy (UGFS) and conservative treatment. 8 The study concluded that there are small differences in the clinical effectiveness of the endovascular procedures relative to the traditional HL/S and that the costs of these strategies could therefore have a major impact on the cost-effectiveness and therefore the choice of procedure.
To the best of our knowledge, no comprehensive cost and outcome analysis has been performed on the range of endovascular procedures from both a ‘healthcare payer’ and a ‘societal’ perspective. The objective of this study was therefore to (1) investigate the comparative cost-effectiveness of available interventions for great saphenous varicose veins disease that is available and reimbursed in the Norwegian National Healthcare System and (2) to evaluate how the choice of perspective would impact cost-effectiveness.
Materials and methods
Model structure
A decision tree model was developed using TreeAge Pro 2015 (TreeAge Software Inc., Williamstown, MA, USA) to compare treatment strategies (Table 1). 3 Only procedures available in the Norwegian National Healthcare System were included in the study, and an additional no-treatment strategy was added as a baseline for ranking the strategies. 9 Quality-adjusted life years (QALYs) were used as the main outcome measure.
Treatment strategies included in the cost and outcome analysis.

The model simulates the clinical course during the first year after the surgical procedure, where patients may have complications or not (Figure 1). If they have complications, a QALY-loss corresponding to the severity of the complication, and any additional cost due to the complication, is imposed. At the end stage, the 1-year perspective patients either face treatment failure, that is, recurrent varicose veins as in the pre-treatment condition, or treatment success, indicating a decline in varicose vein symptoms.
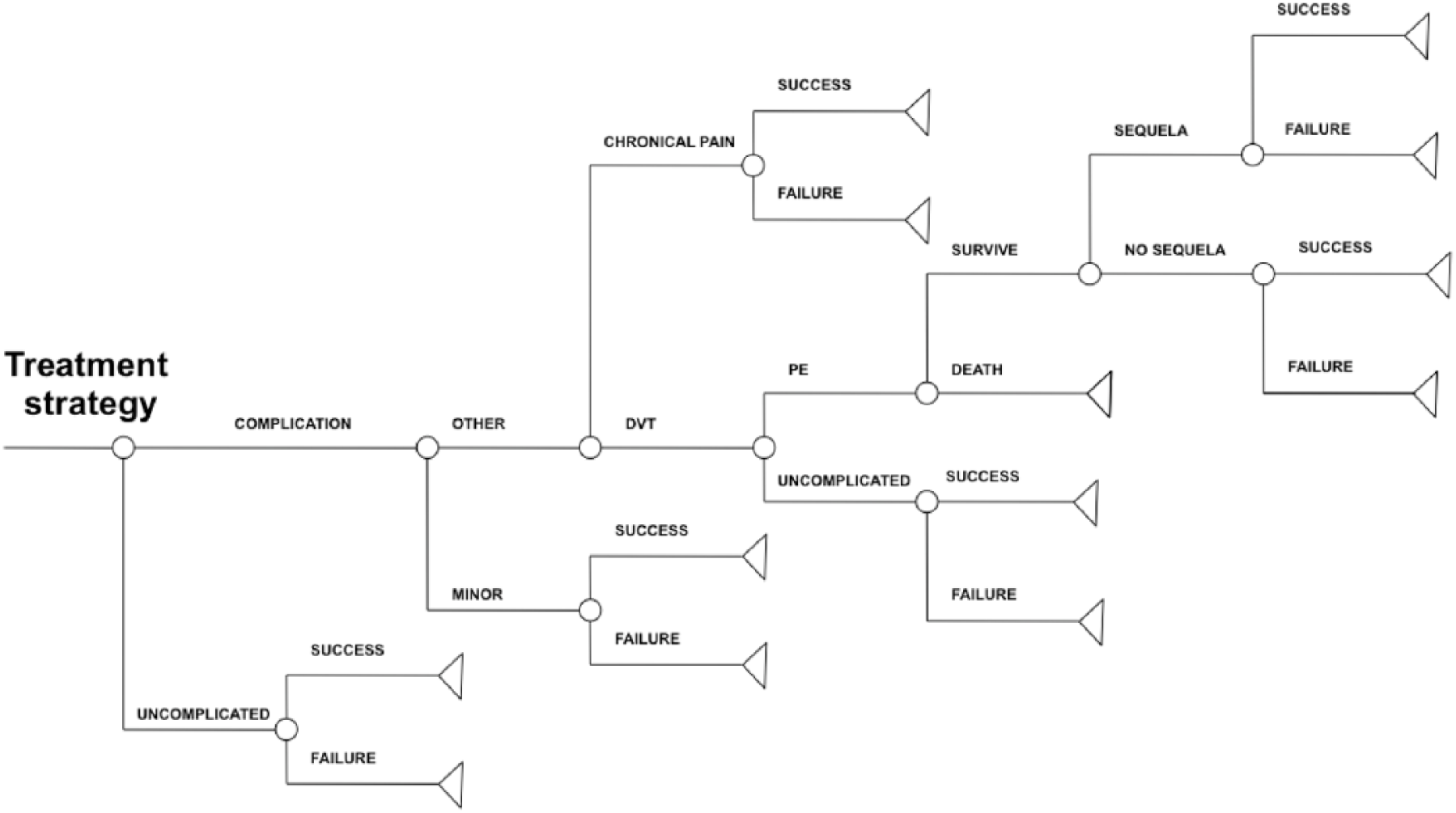
Detailed structure for a treatment strategy in the model.
The model was developed to capture direct costs as well as societal costs, and simulations could be performed either in a narrow healthcare payer perspective or a broader societal perspective. A panel of two vascular surgeons and an internal medicine specialist provided expert advice about clinical practice to help inform development of the model.
Model assumptions
Costs assumed to be equal across procedures, for example, preoperative assessment, were omitted. Based on availability of data in the existing literature, a 1-year perspective was chosen to capture the postoperative course. 10 Based on epidemiological data, a base case representative of the patient population – a 50-year-old female with CEAP C2, great saphenous vein insufficiency – was chosen for modelling purposes.11,12 This choice influenced the following input data: life expectancy, annual income, success-rates of procedures and rate of complications. The cost of sick leave and potential loss of future production were only included in the societal perspective.
Postoperative complications included in the model are as follows: minor complications, deep venous thrombosis, pulmonary embolism, post-thrombotic syndrome and chronic pain. Minor complications represent a hybrid state consisting of occurrences of haematoma, wound infection, temporary sensory loss, pain or bruising. We included certain restrictions: a thromboembolic event was only allowed once during the 1-year model period, and the chronic pain was modelled as a separate state to reflect its persistent nature.
Input parameters
A PubMed search was performed in May 2014 to identify clinical studies from 2004 to date on the five relevant procedures. The initial search resulted in 175 papers on RFA, 604 papers on EVLA, 114 papers on HL/S, 11 papers on stem vein sclerosis (SVS) and 1 paper on cyanoacrylate. The highest level evidence papers were then selected according to Grading of Recommendations, Assessment, Development and Evaluations (GRADE) criteria so that meta-studies and randomised controlled trials were used where available. 13
Probabilities. All probabilities used in the model are presented in Table 2. If no published data were available, the expert panel was consulted.
Probabilities for treatment failure and specific complications for the treatment strategies.

HL/S: high ligation/stripping; EVLA: endovenous laser ablation; SVS: Steam vein sclerosis; CA: cyanoacrylate adhesive; RFA: radiofrequency ablation; DVT: deep vein thrombosis; RCT: randomized controlled trial.
When an SD was not available, half of the ‘Value’ was set as default SD.
Utilities. In cases where no equivalent health-state could be found, a health-state resembling that in the model was chosen (Table 3). In the deep venous thrombosis arm of each treatment, the option ‘death’ was assigned as a possible outcome of pulmonary embolism. The associated life-year loss was based on 2014 mortality tables from Statistics Norway. 41 Thus, for a 55-year-old woman, the life-year loss was 29.4 or 16.8 discounted by 4%, as recommended by Ministry of Finance in Norway.
Health-related quality of life (utilities) according to disease states.

DVT: deep vein thrombosis; PE: pulmonary embolism; TTO: time trade off; SF-6D: Short Form 6D; SD: standard deviation.
Costs. All costs are measured in 2015 Norwegian kroner (NOK) and then translated into Euro (€) (€1.00 = NOK8.35; Table 4). 42 Loss of future production was calculated in case of death due to pulmonary embolism. Micro-costing was performed for all surgical techniques (Supplemental Tables 5–9). Prices of multi-use and disposable equipment were collected from distributors of surgical equipment. Wage rates from the Western Norwegian Health Care Enterprise were used to calculate cost of personnel. Furthermore, a cost estimation was performed to give an average cost of complications (Supplemental Tables 10–12).
Costs of the different treatment strategies and complications used for the model.

HL/S: high ligation/stripping; EVLA: endovenous laser ablation; SVS: Steam vein sclerosis; CA: cyanoacrylate adhesive; RFA: radiofrequency ablation; DVT: deep vein thrombosis; PE: pulmonary embolism.
Statistical analysis
Because many model parameters were uncertain, their point estimates were replaced by probability distributions (Gamma for costs and Beta for probabilities/utilities) to allow for probabilistic sensibility analysis. 43 A Monte Carlo simulation with 10,000 iterations was run to get an overall estimate of uncertainty in the model. Procedures were ranked by expected (mean) cost. Strategies that were costlier and without greater expected benefit were denoted as ‘dominated’ and therefore excluded. For the remaining strategies, we calculated the additional cost per additional QALY gained (the so-called incremental cost-effectiveness ratios (ICERs)). Cost-effectiveness acceptability curves were also used as a summary of the uncertainty in the cost-effectiveness estimates. 3 A suggested threshold for cost-effectiveness in the Norwegian National Healthcare System of €59,880 was applied. By applying this threshold, it is possible to present the uncertainty that any treatment strategy will be cost-effective in a Norwegian setting. 44
Results
One year without any treatment for varicose veins entailed 0.790 QALYs, but no costs (Supplemental Table 13). SVS and EVLA strategies had the best outcomes (0.976 and 0.975 QALYs, respectively), while the lowest QALY was found in RF ablation (0.960). In terms of societal costs, the HL/S strategy had the highest expected total cost over the first year with €3506, while EVLA had the lowest with €1558.
In the societal perspective, EVLA was the most cost-effective treatment strategy with an ICER of €8448 compared to the no-treatment strategy (Supplemental Table 13). Replacing EVLA by SVS entails €39,258 per additional QALY. All other strategies had higher costs and worse outcomes (strictly dominated). In the healthcare payer perspective, SVS was the most cost-effective strategy with an ICER of €4072 compared to the no-treatment strategy (Supplemental Table 14). All other cases were strictly dominated.
Based on a willingness-to-pay of €59,880 per QALY in the societal perspective, the probability that EVLA is cost-effective was 45%, while the probability that SVS is cost-effective was 42% (Figure 2). For RF, cyanoacrylate adhesive (CA), HL/S and ‘no treatment’, these probabilities are all below 5%. In the healthcare payer perspective, using the same willingness to pay, the probability that SVS is cost-effective was 50%, and the probability that EVLA is cost-effective was 42%. For HL/S, the probability that the procedure was cost-effective was 8%, while CA, RF and no treatment all had a probability below 5%.

Cost-effectiveness acceptability curve (CEAC) of treatment strategies from analysis using the societal perspective.
Discussion
The results of this study indicate that the optimal choice of treatment for varicose veins depends on the perspective of the decision maker, with EVLA as the most cost-effective strategy from a societal perspective and SVS as the optimal choice from a healthcare payer perspective. Because of minimal differences in the clinical effectiveness of the surgical techniques, differences in societal costs had a major influence on the results when comparing the two perspectives.
Our results, indicating endovascular laser treatment as a favourable choice, are not unique. Gohel and co-workers also report that EVLA would likely be cost-effective given a potential NHS threshold of £20,000–£50,000. 7 The optimal choice of treatment in their analysis, however, was UFGS. The recent HTA performed by Carroll and co-workers had the same finding; the UFGS alternative was favoured over EVLA treatment. 8 Concerns have been raised about the safety of UGFS because of reports of cerebral and neurological side effects of this procedure.46,47 These effects were not modelled in any of the studies above. Another concern is the relatively high early recurrence rate within the first 3 months following initial surgery. In the base case analysis of the Gohel model, this contributed to a low probability (<10%) that the UFGS alternative would be cost-effective at a willingness-to-pay threshold of £20,000. The UGFS is not used in the Norwegian Healthcare System and has therefore not been considered in this study.
A concern of most decision models is the adequacy of the chosen time perspective. While the 1-year time horizon used in our model is short and was driven by the characteristics of available data, it is likely to capture the majority of costs and the most common complications associated with the treatments.6,8,10 A 1-year perspective will, however, likely underestimate the health gain of varicose vein surgery, as it does not include future QALY gains associated with the procedure. In a work by Kuhlmann and co-workers, varicose vein treatment by HL/S and RFA was modelled in the Statutory German Health Insurance setting. 5 They found that the robustness of the economic analysis deteriorated as the time horizon increased due to the lack of good input data. In light of this potential trade-off between the accuracy of the model and the completeness of the perspective, we believe that this work gives an adequate presentation of the alternative procedures.
A challenge when modelling treatment for varicose veins is the slight skewness of the available data on clinical effectiveness and the incidence of complications after surgery. The more established procedures, that is, HL/S, RF and EVLA, have a substantially larger body of published evidence, permitting more accurate estimates of these probabilities. To date, only a few clinical studies on the effectiveness of the SVS and CA procedures exist;31,32 therefore, the evidence is less robust than that for the former three. Greater certainty in cost-effectiveness estimates could be achieved in the future if additional clinical studies expanded data availability. Another important reason for repeat evaluation of endovenous techniques for varicose reflux treatment is the potential advances in effectiveness of the technology that can come of their further development.
Micro-costing of the different surgical techniques indicated that compared to HL/S, the endovascular procedures had a higher cost for necessary disposable equipment (e.g. RF/laser/SVS catheters, cyanoacrylate glue). If the endovascular procedures can be performed in an office-based setting, these costs are partially offset by savings associated with not needing an operating room. Macario and co-workers suggested that the price of running an operating room was US$29–US$80 per minute. 48 An important part of these cost are the so-called overhead costs (ranging from electricity bills to facility maintenance). In the current calculation, general costing rules from the Norwegian Directorate of Health were applied for overhead costs. 49 In a study by Schreyögg and co-workers, a micro-costing approach for appendectomy was performed across 54 hospitals in nine European countries. 50 The overhead costs were highly variable across hospitals and across countries, spanning from €105 (Spain) to €2028 (Denmark). Variability is likely to depend strongly on factors such as size of the surgical facilities and the surgical case-mix; therefore, the approach used in the current thesis might be somewhat crude in estimating the true overhead costs.
An important finding in this study is the great difference in the total cost of the first year of treatment between the healthcare payer and societal perspectives. In light of a relatively small difference in the clinical effectiveness of the strategies, there seems to be a much higher societal cost for the traditional HL/S strategy due to the long sick leave period as compared to endovascular alternatives. We would therefore underscore the importance of adopting the societal perspective when undertaking cost-effectiveness analyses of surgical procedures. Furthermore, the costs found to rise from the range of complications that can potentially be seen after varicose vein surgery should be considered. In 2015, the estimated costs of in-hospital care for deep venous thrombosis and pulmonary embolism was €3893 and €6628, respectively. 49 Minor differences in the incidence of deep venous thrombosis could therefore potentially change the results of an economic evaluation when modelling the treatment options of varicose vein surgery. Finally, the cost involved in the use of different treatment methods is also an important factor driving the likelihood that they are cost-effective. It is well-known that newer technologies might come at a higher cost and that the cost-efficiency profile might change over time as patents run out or competing products might reduce their price.
There are several limitations to this study – some of which have already been mentioned. The time-span of 1 year after surgery limits assessment of cost and outcomes. A model will never be more realistic than the quality of the input data: both the unequal availability of data across the procedures and the limited availability of long-term data did, in that sense, restrict this study. The ongoing and rapid evolution in varicose vein treatment justifies repeat analyses to account for new methods and also to include updated results on outcomes and complications on existing techniques. An example of a recent promising advance in techniques that have not been included in the current work is mechanochemical endovenous ablation (MOCA) that justifies further analyses.51–53 Also, the simplification of a postoperative course, for example, in minor complication and deep venous thrombosis, limits how realistic the model can be. The strength of the current methodology is, however, the ability to compare costs and outcomes across a range of treatment strategies using a synthesis of published data from various sources.
Conclusion
Among the five procedures for varicose veins in middle-aged women, EVLA is the most cost-effective treatment strategy with a cost of €8448 per QALY gained in a societal perspective, while steam vein sclerosis is most cost-effective in a healthcare payer perspective (€4072 per QALY). Due to uncertainty in the input data, the ranking of procedures should be interpreted with caution except that traditional stripping has higher societal costs than the others. The current analysis found that societal costs have a major impact on the outcome. These costs should therefore be considered when making decisions on implementing new surgical treatments.
Supplemental Material
SUPPLEMENTAL_MATERIAL-tables – Supplemental material for Cost-effectiveness analysis of five procedures for great saphenous vein reflux in a Norwegian healthcare setting or societal setting
Supplemental material, SUPPLEMENTAL_MATERIAL-tables for Cost-effectiveness analysis of five procedures for great saphenous vein reflux in a Norwegian healthcare setting or societal setting by Eivind Inderhaug, Carl-Henrik Schelp, Inge Glambek and Ivar S Kristiansen in SAGE Open Medicine
Footnotes
Acknowledgements
All the contributing parties are co-authors on the papers, so no further acknowledgements are needed. Finally, no ethical approval was needed for this work since the model only made use of formerly published data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for this study because not applicable since study involved modelling.
Trial registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.