
Abstract
Aim/Objective:
To evaluate the impact of an m-health training program on nurses’ knowledge, attitudes, and practices concerning antimicrobial resistance within hemodialysis units.
Background:
Hemodialysis patients face high infection risks, driving antimicrobial use and resistance. Nurses’ antimicrobial resistance knowledge gaps underscore the need for effective training.
Design:
A parallel group randomized controlled trial.
Methods:
A convenience sample of 64 nurses was cluster-randomized into either an m-health group (n = 32) or a control group (n = 32). The m-health group received antimicrobial resistance education through a WhatsApp Chatbot, while the control group received no information on the study topic. However, they were provided the study intervention after the evaluation was completed. The nurses’ knowledge, attitudes, and practices regarding antimicrobial resistance were assessed with self-developed instruments at three time points: Baseline (Time 1), immediately after the intervention (Time 2), and 1 month later (Time 3).
Results:
Repeated-measures Analysis of Variance (ANOVA) (within-subject) tests indicated significant differences in mean scores for antimicrobial resistance knowledge, attitudes, and practices across the three time points in the m-health group. The repeated-measures ANOVA (mixed model) tests revealed significant interaction effects in antimicrobial resistance knowledge, attitudes, and practice.
Conclusions:
m-Health training program significantly enhanced dialysis nurses’ knowledge, attitudes, and practice toward antimicrobial resistance. It is recommended to communicate the findings of this study to managers and policymakers to equip them with the information needed to develop and implement effective strategies, policies, and multidisciplinary interventions aimed at reducing antimicrobial resistance in hemodialysis units.
Keywords
Introduction
Patients undergoing hemodialysis treatment are at an increased risk for infections because these patients require prolonged healthcare interventions, have weakened immune systems, use antibiotics, receive treatment in a shared healthcare setting, and require vascular accesses such as catheters, fistulas, and venous central lines. 1 Infection is the second master cause of mortality in the hemodialysis population, accounting for 8% of all deaths. Patients undergoing hemodialysis have higher rates of infection in comparison with others, particularly sepsis. 2
Due to the high rate of infections among patients undergoing hemodialysis, there is a significant utilization of antimicrobial agents in this population. This extensive use has led to the emergence of multidrug-resistant organisms in hemodialysis units. 3 Antimicrobial resistance (AMR) arises when microorganisms, including bacteria, fungi, viruses, and parasites, evolve mechanisms to resist the effects of antimicrobial agents.4–6 Staphylococcus aureus is responsible for up to 70% vascular access infections among hemodialysis patients, a challenge exacerbated by the spread of methicillin-resistant S. aureus (MRSA) strains. Approximately 90% of those infected with MRSA require hospitalization, and 17% of these patients do not survive their hospital stay. 7
In Jordan, infections caused by gram-positive bacteria, along with significant antibiotic resistance rates, have been prevalent. Infections from MRSA and methicillin-resistant coagulase-negative Staphylococci are common, showing high levels of antibiotic resistance. Additionally, streptococcus pneumonia has shown increasing resistance to multiple antimicrobials. 8 Reports from hospitals in Jordan have highlighted a significant prevalence of AMR, with MRSA cases reaching 45%. This resistance contributes to higher rates of illness, mortality, and extended hospital stays. 9 The economic burden of AMR is significant, with projections indicating that by 2050, it could cost the global economy between $300 billion and $1 trillion. 10
Nurses play a crucial role in managing AMR in hemodialysis centers by promoting the appropriate use of antimicrobial drugs and implementing effective infection prevention and control measures. They ensure early diagnosis of infections by closely monitoring patients during dialysis sessions and promptly identifying any signs of infection. Nurses maintain strict hygiene protocols, such as frequent handwashing, proper use of personal protective equipment, and thorough cleaning of dialysis equipment and surfaces, to prevent the spread of infections. In addition, they educate patients about the importance of completing their antibiotic courses, understanding the risks of AMR, and adhering to prescribed treatments. By doing so, nurses help reduce the incidence of infections and the development of resistant organisms, ultimately improving patient outcomes and safety. 11 However, existing literature indicates that nurses often lack knowledge, attitudes, and skills related to various dimensions of AMR in patients undergoing hemodialysis. 12 This highlights the need for developing and implementing effective and innovative continuous educational programs to address these gaps. Recently, advanced technology has made it possible to implement new types of behavioral change education. Mobile health (m-Health) is an example. 13
e-Health is defined as the secure economical form to support healthcare services, health surveillance, education, literature, knowledge dissemination, and research in health-related fields. The e-Health technologies improve health and influence health behaviors by making health information and existing services more accessible, remote, and cost-effective. 13 m-Health is a subset of e-Health. While e-health encompasses all applications of information and communication technologies in healthcare, including electronic health records, telemedicine, and health information systems, m-health specifically refers to the use of mobile devices, such as smartphones and tablets, to deliver health services and information. A WhatsApp Chatbot is an example of m-Health, acting as an Artificial intelligence (AI)-powered tool designed to provide telehealth services through text-based interactions on electronic devices such as mobile. It can educate healthcare professionals and patients by delivering medical information, answering clinical queries, and providing training resources directly through the WhatsApp application. 14 Recent studies highlight the growing importance of healthcare AI chatbots for health education and e-health, especially during the COVID-19 pandemic. 15
Few studies have examined AMR training for nurses.5,15,16 However, none of them used m-health. Hendy et al. 15 and Lutfiyati et al. 16 both found that training on antimicrobial stewardship significantly improved nurses’ knowledge, attitudes, and practices. Boban et al. 17 observed significant improvement in AMR knowledge and attitudes in higher education students, including nurses. Similarly, Kpokiri et al. 18 noted that AMR training enhanced overall knowledge of antibiotic use and resistance among healthcare professionals. The current study aims to address this gap by evaluating the effectiveness of a WhatsApp AI Chatbot-based training program on AMR, focusing on the knowledge, attitudes, and practices of nurses working in hemodialysis units. The results of this study are clinically significant to improve patient care and safety by enhancing practices regarding AMR.
Method and materials
Research design
The study employed a parallel group randomized controlled design between June and July 2024. The study participants were selected using a convenient sampling method and then distributed randomly into the study groups (1:1) by a cluster random assignment, a sequence generated by Random Allocation Software, this precaution was taken to reduce contamination.
Sample and setting
Participants were selected from four major hospitals representing the private, military, and public sectors. Registered nurses working at hemodialysis unit who met the following criteria were invited to participate in this study: (1) having smart phones, (2) the ability of reading and writing in English, (3) and commitment to complete all study protocols. The exclusion criteria consisted of (1) the nurses who have taken training about the prevention of AMR and antibiotic uses or the infection control measures in hemodialysis units, and (2) the nurses with less than 3 months of clinical experience. Nurses with less than 3 months of clinical experience were excluded from the study to ensure that all participants had a sufficient level of practical experience and familiarity with clinical protocols. These nurses were still under training probation.
Setting
Hemodialysis units at the Prince Rashid Ben AL-Hasan Militarily Hospital/Jordanian Royal Medical Services (JRMS), Al-Hussein Hospital at King Hussein Medical City/JRMS which is private hospital, the Princess Haya Bent Al-Hussein Military Hospital/JRMS, and the King Abdullah University Hospital which is university hospital during the period of January 2024 to February 2024.
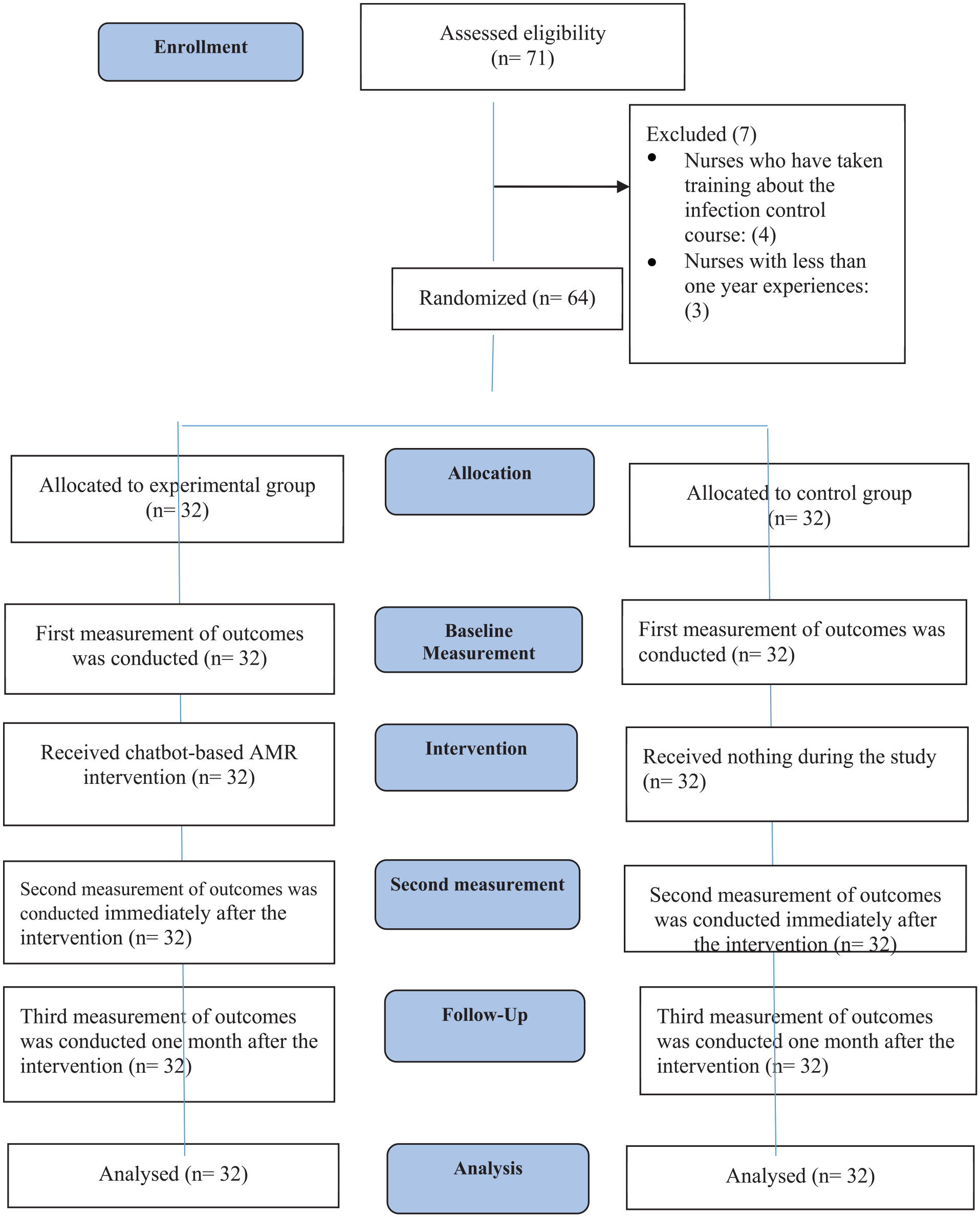
The sample size was calculated using G-power software (Version 3.1.7) (Heinrich Heine University Düsseldorf in Germany). With an alpha level of 0.05, a statistical power of 0.9, an effect size of 0.19, and a repeated-measures ANOVA test (mixed model), the minimum required total sample size was calculated to be 60 participants. Considering a 15% attrition rate, 9 participants were added, resulting in a final required sample size of 69. Out of the 69 participants initially recruited, 64 completed the study and had their data included in the analysis (see Figure 2).
Intervention
The educational program developed by the researchers is meticulously designed, drawing on extensive insights from the WHO curricula guide and the literature review addressed the use of antibiotics and prevention of AMR in hemodialysis facilities (see Figure 1). 19 The curriculum, using simple English, provides a broad set of learning objectives tailored to the expected roles of nurses. The educational materials were reviewed and validated by a team of experts, including experienced nurses with advanced degrees in adult health nursing and specializations in nursing nephrology (n = 2), as well as an infectious disease specialist (n = 1). This multidisciplinary team ensured that the content was accurate, relevant, and appropriate for the target audience. In addition, the materials were pilot-tested with a small group of hemodialysis nurses (n = 5) to gather feedback and make necessary adjustments before the full implementation of the training program. Feedback from the pilot participants indicated that the educational materials and questionnaires were clear and feasible. The participants involved in the pilot study were not included in the final sample size. The study was registered in the Clinical Trial. Gove (Date: 10/08/2024, ID: NCT06632132).

Intervention framework.
The educational program is structured into four primary modules:
Fundamental Concepts—This module aims to raise awareness about AMR, covering key areas such as a systemic approach to managing infections at an individual level and understanding antimicrobial agents and their appropriate management.
Responsible Use of Antimicrobials—Focused on ensuring the proper clinical application of antimicrobial agents, this module addresses the clinical management practices for their use. Clinical management practices refer to the standardized procedures and protocols that nurses follow to ensure the appropriate use of antimicrobial agents. This includes guidelines for prescribing antibiotics, monitoring patient responses to treatment, and adjusting dosages as necessary.
Infection Control and Prevention—This module examines healthcare-associated infections, AMR, and infection control practices necessary for effective prevention.
Diagnostic Stewardship and Surveillance—Highlighting the connection between diagnostic practices and AMR monitoring, this module also covers the broader aspects of antimicrobial stewardship.
To design a suitable Chatbot for the participants, The study researchers provided the engineering team with detailed requirements and specifications. This included the educational content structured into four primary modules: Fundamental Concepts, Responsible Use of Antimicrobials, Infection Control and Prevention, and Diagnostic Stewardship and Surveillance. They also provided sample dialogues, user interaction flows, and specific functionalities such as auto-reply with educational dialogue, tracking user progress, and delivering content in various formats (text, images, and videos). The video materials included in the educational modules were designed to be concise and engaging, with each video lasting approximately 5–10 min. The videos were a mix of animated and live-action formats, providing visual explanations of key concepts, demonstrations of best practices, and real-life scenarios to enhance understanding.
For the m-health group, the educational material was sent by a study researcher to the WhatsApp number for all members of the m-health group via Chatbot software, which was designed by a software engineer. This software is a strategic move that holds immense potential for transforming the way nurses access information and support. In the dynamic and demanding field of healthcare, nurses often face time constraints and require immediate access to relevant resources. A WhatsApp Chatbot designed for nursing education can serve as a virtual companion, providing real-time assistance and information crucial to their roles. The way information is presented and shared on a Chatbot is one of the most important factors that directly affect the user experience. In contrast to conventional interfaces, a Chatbot method is usually more dynamic and user-friendly since information is frequently communicated through conversational engagements. 20 AMR training programs were presented in Chatbot software as outlined. The educational materials were sent in the form of written materials, photos, and videos. The study researcher, who was an experienced nurse with a master’s degree in nursing and received extensive training about using WhatsUp Chatbot from the engineering team explained how to use the program to each nurse in m-health group.
The program was auto-reply with the educational dialogue that had been previously entered into this program. Also, the researcher advised the participant to read each part carefully. The application allows the researcher to view the parts that have been accessed and read by participants in the educational program. For 1 week, nurses in m-health group completed the AMR training program, then the Chabot software was closed before evaluation phase started. For the control group, they were not given any educational content during the study. However, they were provided with the educational material received by m-health group via Chatbot software after evaluation completed.
Instruments
The study questionnaire was developed by the study researchers based on the educational program’s objectives. Two of these researchers hold PhD degrees in adult health nursing with specializations in nephrology and infection control, while one has a master’s degree in acute adult health nursing. It consists of four parts: (1) Sociodemographic characteristics, (2) Dialysis Nurses’ Knowledge of Antimicrobial Use and AMR in HD units, (3) Dialysis Nurses’ Attitudes Toward Antimicrobial Use and AMR in HD units, and (4) Dialysis Nurse’s practice of Antimicrobial Use and AMR in HD units.
Sociodemographic data form
The sociodemographic data sheet included questions about sex, age, phone number, highest professional qualification, current hospital of employment, overall working experience, working experience in hemodialysis unit (years), previous attendance of training courses about AMR, and infection control training course.
Knowledge of antimicrobial use and resistance
A self-developed questionnaire to assess the dialysis nurses’ knowledge of antimicrobial use and resistance included 28 true and false questions. The answer choices constituting each of the questions were True, False, and I do not know. One point was given for each right answer and 0 points for each wrong answer. If participants selected the choice of “I do not know” for certain question, they would be given 0 on that question. The maximum possible score was 28 points with a range from 0 to 28 points. A higher total score indicated a higher level of knowledge of antimicrobial use and resistance (Appendix A).
Attitudes toward antimicrobial use and resistance
The self-developed scale to measure the dialysis nurses’ attitude toward antimicrobial use and resistance includes 11 well-formulated items. Each item was rated on a five-point Likert-type scale (strongly disagree (1) to strongly agree (5)). The maximum possible score was 55 with a range from 11 to 55 points. A higher score means the participants had a more positive attitude toward the appropriate use of antimicrobials and higher sensitivity to AMR (see Appendix B).
Practice of antimicrobial use and resistance
The self-developed questionnaire to evaluate the dialysis nurses’ practice regarding the proper use of antimicrobials and the issue of AMR, includes 27 well-formulated items. Each item was assessed on five-point Likert scale, which ranges from 1 (never) to 5 (always). The total scale ranges from 27 to 135. A higher score of this scale indicated higher strictness of antimicrobial use practices and strong compliance with protocols to prevent AMR.
Content validity of the tools
The completed tool underwent a content validity assessment (CVI) conducted by a panel of four experts. This panel included professionals with master’s degree in pharmacy specializing in clinical pharmacology, infection control specialists with master’s degrees in nursing, and a nursing education expert with a PhD in nursing and extensive experience in adult health nursing. The tool items were overlaid in a matrix with two option rating scales: (1) Importance which is divided to three rating scales (Not necessary, Useful but not necessary, Essential), and relevance which is divided into four rating scales (Not relevant/not clear, Item needs some revision, Relevant/clear but need minor revision, very relevant/clear). Statistics were subsequently used to assess the degree of reviewers’ agreement on the importance and relevance of the tool items. The Content Validity Index values for the Dialysis Nurses’ Knowledge of Antimicrobial Use and AMR, the Dialysis Nurses’ Attitudes Toward Antimicrobial Use and AMR, the Dialysis nurse’s practice of Antimicrobial Use and AMR were 0.978, 0.927, and 0.977, respectively. These values indicated an acceptable level of validity index values.
Pilot testing
A pilot study was conducted on 15 registered nurses working in HD units to assess the clarity, objectivity, and feasibility of the study’s self-developed instruments. Through the pilot study, the time required for data collection was estimated to be approximately 30 min. The nurses in the pilot study were not included in the main study sample.
Reliability
In the current study, the Cronbach’s alpha values for the Dialysis Nurses’ Knowledge of Antimicrobial Use and AMR, Dialysis Nurses’ Attitudes Toward Antimicrobial Use and AMR, Dialysis nurse’s Practice of Antimicrobial Use and AMR 0.705 and were 0.75, and 0.86, respectively. These values indicated an acceptable level of internal consistency reliability.
Data collection procedure
Institutional Review Board (IRB) approval was obtained prior to commencing the study, followed by securing administrative approvals from the respective study settings. A list of nurses working in the hemodialysis units was then acquired from the head nurse of each unit at the target hospitals. This list included the names and telephone numbers of the nurses. After obtaining the list of nurses, each nurse was contacted by phone. The call followed these steps: the researcher introduced themselves, explained the purpose of the call and the study, and sought verbal consent from the nurse to participate if they met the study criteria. The researcher then gathered information from each nurse to assess their eligibility for the study.
A list of nurses who met the study criteria was compiled, including their work shifts (A, B, and C) and the names of their respective hospitals. The authors ensured that the nurses in each shift remained on the same shift throughout the duration of the study. Each shift at each hospital was treated as a cluster, with six participants recruited from each cluster. This resulted in the identification of 12 clusters (4 hospitals × 3 shifts). These 12 clusters were done randomly with six for each. This randomization strategy was carried out by an independent researcher who was not involved in the recruitment process and remained blinded to the participant list. The purpose of employing cluster randomization was to prevent contamination between the intervention (m-health group) and control groups (no intervention).
The researchers scheduled a meeting and interviewed each eligible nurse individually to obtain written consent and implement the baseline measurement. The baseline assessment was conducted onsite in a private, quiet room to ensure confidentiality and comfort. Participants completed the self-administered questionnaire in this setting without any external influence. Upon written consent obtained by the study researchers, a well-trained nurse—a research assistant from each hospital took the nurses’ names from the researchers without knowing which of the two groups the nurse was assigned to. Each research assistant underwent a comprehensive training program lasting 2 days. The training covered the study protocol, ethical considerations, data collection procedures, and the use of the Chatbot software. Competency was ensured through practical demonstrations, role-playing scenarios, and a final assessment to confirm their understanding and ability to deliver the intervention effectively.
All nurses received the self-administered questionnaire from the research assistants. On the same day, the questionnaires were collected once the nurses had finished. Informed consent was obtained in person during scheduled meetings at the participants’ units.
The average time to complete the questionnaire was 30 min. The data obtained during this phase served as the baseline (Time 1). The same questionnaire, excluding the demographic characteristics, was completed again by the two study groups immediately at the end of interventions for m-health group (Time 2) and 1 month later (Time 3). Each participant completed the study questionnaire individually in a private, quiet room in the hospital without anyone else present, including the research assistant.
Ethical consideration
Before collecting data, ethical approval was obtained from the IRB at Jordan University of Science and Technology and the IRB committees (Approval Number: 2023/16-4/81) of Jordan Royal Medical Service (Approval Number: T.F/3/1). Nurses were then given a comprehensive verbal explanation of the study and asked to consider their participation within 1 h. Informed written consent was signed in the study setting and obtained from those willing to participate. A copy of the consent form was provided to each nurse. It was clearly communicated that participation was voluntary and they could refuse without any consequences.
Privacy expectations were explained to participants by a study researcher with a master’s degree in acute adult health nursing. Participants were informed that their data would be kept confidential and used only for research purposes. They were given 1 h to consider participation, ensuring no pressure to participate. The voluntary nature of the study was emphasized, and participants were assured that their decision would not affect their professional standing or the care they received.
All data were stored in a locked cabinet at the academic advisor’s office and on a password-protected computer, ensuring that only the study researchers had access to the data. Identification was anonymized by replacing names with numbers. Participants were informed of their right to withdraw from the study at any time.
Data analysis
The Statistical Package for Social Sciences (SPSS version 26, IBM SPSS Statistics) was utilized. Descriptive statistics such as mean, standard deviation, percentage, and frequency were used to describe the study variables. For each main study variable, the repeated-measures ANOVA test (within groups) examined the mean differences over time for each group separately. In addition, repeated-measures ANOVA tests (mixed model) examined the mean score differences between the study groups over time. p-values of 0.05 or less were used to determine whether the results were statistically significant.
Results
The study flow diagram (Figure 2) outlines the progression of participants in the current study. Initially, 71 nurses were assessed for eligibility. Seven were excluded, including four who had previously completed infection control training and three with less than 1 year of nursing experience, leaving 64 eligible participants. These nurses were randomly allocated into two equal groups: 32 in the experimental group, who received the intervention, and 32 in the control group, who did not receive the intervention or received standard care. Both groups demonstrated full adherence, with no dropouts, as all 64 participants completed the study protocol. The final analysis included all 64 participants, ensuring that the study retained statistical power and provided reliable insights into the effectiveness of the intervention in improving infection control practices among nurses.
Study protocol.
Participants’ sociodemographic characteristics
Experimental group
The demographic characteristics of the m-health group are displayed in Table 1. In the m-health group (n = 32). Approximately 60% of them were male. All of them had a minimum bachelor’s degree in nursing. Approximately half of them were working in military hospitals (50%). The mean age of the participants was 36 years old. The mean experience years in hemodialysis units for the m-health group participants was 10.34.
Sociodemographic characteristics of m-health (n = 32) and control groups (n = 32).

Source: Author.
Control group
The demographic characteristics of the control group are displayed in Table 1. In the control group (n = 32). Half of them (50%) were male. All of them had a minimum bachelor’s degree in nursing. Approximately half of them were working in military hospitals (47%). The mean age of the participants was 35.5 years old. The mean experience years in hemodialysis units for the control group participants was 9.96.
Baseline differences in demographic characteristics between the study groups
The results of the Chi-square test demonstrated that there were no significant variations between the two groups in terms of sex (X2(1) = 0.56, p = .451), working place (X2(3) = 0.17, p = 0.982, and work shift (X2(2) = 0.9, p = 0.63). The t-test findings showed that there was no significant difference between the two groups in terms of age (t(62) = −0.82, 95% CI = (−2.02, 0.84), p = 0.411), clinical experience in hemodialysis unit (t(62) = −0.428, 95% CI = (−2.12, 1.37), p = 0.67) (See Table 1).
Analysis of variance on dependent variables across three repeated measures for each group
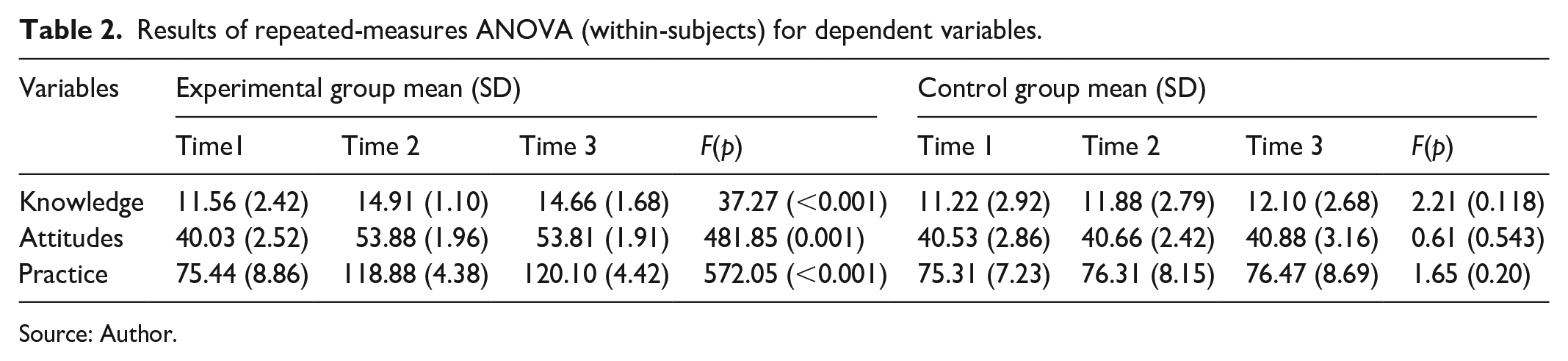
To determine if the dependent variables changed over time in the m-health and control groups, RM ANOVA (within-subject) tests were initially performed (see Table 2).
Results of repeated-measures ANOVA (within-subjects) for dependent variables.
Source: Author.
AMR knowledge
RM ANOVA (within-subject only) results revealed that there were significant main effects of time for AMR knowledge in the m-health group (F(1.66, 51.59) = 37.27, p < 0.001, partial eta squared = 0.54). However, there is a nonsignificant mean effect of time in the control group (F(1.46, 45.34) = 2.21, p = 0.118, partial eta squared = 0.06).
Pairwise comparisons in the m-health group indicated significant differences between AMR knowledge mean scores at Time 1 and Time 3 (Mean difference = −3.09, 95% CI = (−4.48, −1.83), p < 0.001), and at Time 1 and Time 2 ((Mean difference = −3.34, 95% CI = (−4.48, −2.20), p < 0.001). However, there was nonsignificant differences between AMR knowledge scores at Time 2 and Time 3 (Mean difference = −0.18, 95% CI = (−0.87, 0.49), p = 1.00).
AMR attitudes
RM ANOVA (within-subject only) results showed that there were significant main effects of time for AMR attitude in the m-health group (F (2, 62) = 481.85, p < 0.001, partial eta squared = 0.94). However, a nonsignificant meaning effect of time in the control group (F (1.62, 50.36) = 0.61, p = 0.543, partial eta squared = 0.2).
Pairwise comparisons in the m-health group indicated significant differences between AMR attitude mean scores at Time 1 and Time 2 (Mean difference = −13.84, 95% CI = (−15.17, −12.50), p < 0.001), and at Time 1 and Time 3 ((Mean difference = −13.78, 95% CI = (−15.17, −12.38), p < 0.001). However, there were nonsignificant mean differences between AMR attitude scores at Time 2 and Time 3 (Mean difference = 0.06, 95% CI = (−1.09, 1.22), p = 1.00).
AMR practice
RM ANOVA (within-subject only) results showed that there were significant main effects of time for AMR practice in the m-health group (F (1.17, 36.52) = 572.05, p < 0.001, partial eta squared = 0.94). However, there is a nonsignificant mean effect of time in the control group (F (1.46, 45.43) = 1.65, p = 0.20, partial eta squared = 0.05).
Pairwise comparisons in the m-health group indicated significant differences between AMR practice mean scores at Time 1 and Time 2 (Mean difference = −43.43, 95% CI = (−47.67, −39.20), p < 0.001), and at Time 1 and Time 3 ((Mean difference = −44.65, 95% CI = (−49.43, −39.88), p < 0.001). However, there was nonsignificant mean difference between AMR practice scores at Time 2 and Time 3 (Mean difference = −1.21, 95% CI = (−2.86, 0.43), p = 0.213).
Analysis of variance on dependent variables across three repeated measures by group
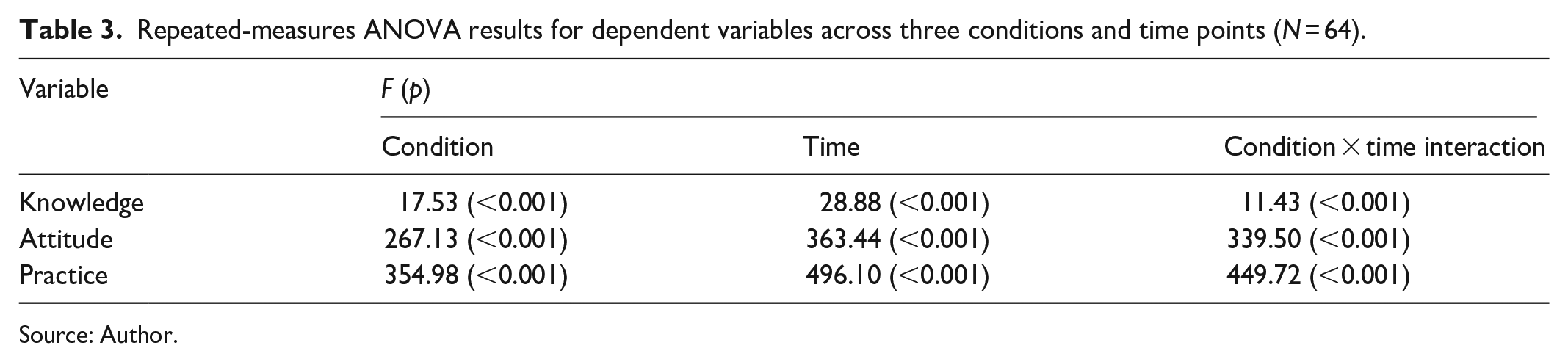
2 × 3 RM ANOVA (mixed model) was conducted to examine differences in each dependent variable by condition (m-health and control groups) and time (Time 1, Time 2, and Time 3) (see Table 3).
Repeated-measures ANOVA results for dependent variables across three conditions and time points (N = 64).
Source: Author.
AMR knowledge
The findings showed that there were significant main effects of time (F (1.59, 98.68) = 28.88, p < 0.001, partial eta squared = 0.31), conditions (F (1, 62) = 17.53, p < 0.001, partial eta squared = 0.22), and time-by-condition interaction (F (1.59, 98.68) = 11.43, p < 0.001, partial eta squared = 0.15).
AMR attitude
The findings showed that there were significant main effects of time (F (2, 124) = 363.44, p < 0.001, partial eta squared = 0.85), conditions (F (1, 62) = 267.13, p < 0.001, partial eta squared = 0.81), and time-by-condition interaction (F (2, 124) = 339.50, p < 0.001, partial eta squared = 0.84).
AMR practice
The findings showed that there were significant main effects of time (F (1.22, 76.12) = 496.10, p < 0.001, partial eta squared = 0.88), conditions (F (1, 62) = 354.98, p < 0.001, partial eta squared = 0.85), and time-by-condition interaction (F (1.22, 76.12) = 449.72, p < 0.001, partial eta squared = 0.87).
Discussion
Few studies have assessed the effectiveness of m-health AMR training programs on nurses’ knowledge, attitudes, and practices concerning AMR. This study evaluated the impact of such a program specifically on these aspects within hemodialysis units.
AMR knowledge
The results of the present study demonstrate a statistically significant increase in nurse knowledge mean scores over time in the m-health group compared to the control group, indicating that the m-health AMR training program had a beneficial impact on nurses’ knowledge. These results concur with previous research reporting similar positive effects of AMR training programs to improve nurses’ knowledge. Kpokiri et al. 18 in their study discovered that the AMR training for healthcare professionals, including nurses impacts the knowledge. In addition, authors in their study showed that utilizing m-Health applications by nurses are making differences in healthcare outcomes. 21
The current study found significant mean differences between AMR knowledge scores at (Time 1 and Time 2) and (Time 1 and Time 3) for m-health group. The significant difference in AMR knowledge scores between Time 1 and Time 2 and between Time 1 and Time 3, as obtained from the m-health group, may suggest the effectiveness of the m-Health training program. This could mean that the intervention significantly improved knowledge just after its implementation from Time 1 to Time 2 and then managed to sustain the improvements over the longer term from Time 1 to Time 3. Also, this study found nonsignificant mean differences between AMR knowledge scores at (Time 2 and Time 3) for m-health group. The nonsignificant difference between AMR knowledge scores at Time 2 and Time 3 in the m-health group may be explained by the idea that the lack of significant mean changes between Time 2 and Time 3 suggests that while the initial gains in AMR knowledge were significant and maintained over time, improvements because of the training may have reached a plateau. This plateau may be a result of the participants’ consolidation of newly learned information, which after an initial phase of learning may stabilize. Cognitive learning theories suggest that early learning gains tend to be rapid, while the stabilization of knowledge retention then follows as individuals begin integrating their new understanding and applying it. 22 In addition to the plateau effect, other factors such as reinforcement and the duration of the intervention could influence the nonsignificant difference in AMR knowledge scores at time points 2 and 3. Reinforcement through periodic reminders or additional training sessions might help sustain knowledge gains. The duration of the intervention could also be adjusted to ensure more comprehensive coverage of the material.
AMR attitudes
Our study reveals a statistically significant increase in the mean scores of nurse attitudes over time within the m-health group, compared to the control group. Similar to AMR knowledge, the current study identified significant mean differences in AMR attitude scores between Time 1 and Time 2, as well as between Time 1 and Time 3. This suggests that the m-health AMR training program had a positive and lasting impact on nurses’ attitudes toward AMR.
These results concur with previous research reporting similar positive effects of AMR training programs to improve nurses’ attitudes. Boban in their study indicates that the Antibiotic Resistance training for higher education students including nurses, had significant improvement in the knowledge and attitude scores. 17 Also Lutfiyati et al. 16 showed effective improvement in their attitude regarding AMS after using Zoom as an educational tool for nurses.
Also, this study found nonsignificant mean differences between AMR Attitudes scores at Time 2 and Time 3. The nonsignificant difference between AMR Attitudes scores at Time 2 and Time 3 in the m-health group can be explained by Festinger’s cognitive dissonance theory. This cognitive dissonance theory is a powerful tool for understanding and influencing attitudes and behaviors around AMR. Festinger’s cognitive dissonance theory explains how individuals strive for internal consistency between their beliefs and behaviors. When nurses receive training on AMR, they may experience dissonance if their previous practices are inconsistent with the new information. To reduce this dissonance, they adjust their attitudes and behaviors to align with the training. This theory helps explain the observed changes in attitudes and behaviors related to AMR, as nurses integrate the new knowledge into their daily practices. 23
AMR practice
The results of the present study reveal a statistically significant increase in AMR practice mean scores over time in the m-health group compared to the control group. This indicates that the m-health AMR training program had a beneficial impact on nurses’ practices related to AMR. The post hoc analysis in this study revealed significant mean differences in AMR practice scores between Time 1 and Time 2, as well as between Time 1 and Time 3, in the m-health group. These results suggest that the m-health AMR training program had a sustained beneficial impact on nurses’ practices. These results concur with previous research reporting similar positive effects of AMR training programs to improve nurse’s practice. Hendy et al. 15 discovered that there is improvement in perception, knowledge, and practice among nurses that easily translated to the practice.
The nonsignificant differences in the means of AMR practice scores at Time 2 and Time 3 among participants of m-health group were established in the current study. This result can be explained by the concept of habit formation, which suggests that as new practices become routine, the differences observed between successive time points may diminish. Initially, there is often a significant change in behavior, which then gradually stabilizes as the new practices become ingrained. This aligns with the principle that the most substantial changes occur early in the process, with subsequent adjustments becoming smaller as behaviors become more stable. 24
Limitations
This study had limitations. First, the use of a convenient sampling technique has potentially affected external validity. Second, the reliance of the study on self-report measures for assessing outcomes could be susceptible to response bias, including social desirability bias, as participants might answer in a way that they believe will portray them as good nurses.
Clinical implications
The results of the current study are promising. The m-health AMR training program could enhance nurses’ practices by utilizing modern technology to offer accessible, flexible, and interactive learning opportunities. The use of a WhatsApp Chatbot ensures that training materials are readily available to nurses at any time and place. This accessibility is crucial for healthcare professionals who often have irregular and demanding schedules. Nurses can engage with the training content during breaks, after shifts, or whenever it is most convenient for them, ensuring that learning is not constrained by time or location.
The flexibility of the program allows nurses to learn at their own pace. They can revisit materials as needed, which is particularly beneficial for reinforcing complex concepts. This self-paced learning approach accommodates different learning styles and speeds, making it more effective for a diverse group of learners. In addition, the interactive nature of the WhatsApp Chatbot enhances engagement and retention. Nurses can ask questions, receive instant feedback, and participate in interactive modules that simulate real-life scenarios. This interactive approach helps to solidify understanding and makes the learning experience more engaging and enjoyable.
By providing ongoing access to training materials, the program supports continuous professional development. Nurses can stay updated with the latest best practices in AMR and infection control. This continuous learning is essential for adapting to new guidelines and improving clinical practices over time. The program aims to improve nurses’ knowledge, attitudes, and practices regarding AMR. By understanding the importance of infection control measures and the appropriate use of antimicrobial drugs, nurses can implement these practices more effectively in their daily work. This leads to better infection control, reduced spread of resistant bacteria, and more judicious use of antibiotics.
The goal of the training program is to enhance patient care. By applying the knowledge gained from the training, nurses can contribute to better patient outcomes. Effective infection control and appropriate antimicrobial use are critical for preventing the spread of resistant infections and ensuring successful treatment outcomes. Incorporating technology into education makes it easier for nurses to stay current with evolving medical guidelines and practices. The use of a familiar platform such as WhatsApp ensures that the technology is user-friendly and widely accessible. This integration supports nurses in applying best practices effectively in their clinical settings.
Conclusion
These findings from the present study, which dwelled on nurses’ knowledge, attitudes, and practices, illustrate that the m-health AMR training program can have a positive effect in these areas concerning measures of AMR. As a result, it is recommended to improve the knowledge of nurses and build positive attitudes toward AMR through well-designed education and training programs, such as the m-health AMR training used in this study. This, in turn, is bound to improve the quality of care provided by health professionals in hemodialysis settings.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251318153 – Supplemental material for Boosting knowledge, attitudes, and practices: An experimental controlled study evaluating the effectiveness of m-health training on antimicrobial resistance for hemodialysis nurses
Supplemental material, sj-docx-1-smo-10.1177_20503121251318153 for Boosting knowledge, attitudes, and practices: An experimental controlled study evaluating the effectiveness of m-health training on antimicrobial resistance for hemodialysis nurses by Hossam Alhawatmeh, Mohammed Aljarrah, Issa M Hweidi, Nezam Al-Nsair, Mohammad S Alyahya and Sawsan Abuhammad in SAGE Open Medicine
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received funding from Jordan University of Science and Techology, Deanship of Research # 2023/581.
Ethics approval
Ethical approval for this study was obtained from Jordan University of Science and Technology # 2023/581.
Consent statement
Consent was received from all participants prior of conducting of this study.
Trial registration
The study has been registered with the trial registration number, NCT06632132.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.