
Abstract
Background:
Fragile X syndrome, with an approximate incidence rate of 1 in 4000 males to 1 in 8000 females, is the most prevalent genetic cause of heritable intellectual disability and the most common monogenic cause of autism spectrum disorder. The full mutation of the Fragile X Messenger Ribonucleoprotein-1 gene, characterized by an expansion of CGG trinucleotide repeats (>200 CGG repeats), leads to fragile X syndrome. Currently, there are no targeted treatments available for fragile X syndrome. In a recent large multi-site trial, FXLEARN, the effects of the mGluR5 negative allosteric modulator, AFQ056 (mavoglurant), were investigated, but did not show a significant impact of AFQ056 on language development in children with fragile X syndrome aged 3–6 years.
Objectives:
The current analyses from biospecimens collected in the FXLEARN study aimed to determine whether AFQ056 affects the level of potential biomarkers associated with Akt/mTOR and matrix metalloproteinase 9 signaling in young individuals with fragile X syndrome. Previous research has indicated that these biomarkers play crucial roles in the pathophysiology of fragile X syndrome.
Design:
A double-blind placebo-controlled parallel-group flexible-dose forced titration design.
Methods:
Blood samples for biomarkers were collected during the FXLEARN at baseline and subsequent visits (1- and 8-month visits). Biomarker analyses included fragile X messenger ribonucleoprotein-1 genotyping by Southern blot and PCR approaches, fragile X messenger ribonucleoprotein-1 mRNA levels determined by PCR, matrix metalloproteinase 9 levels’ detection using a magnetic bead panel, and targets of the Akt/mTOR signaling pathway with their phosphorylation levels detected.
Results:
This research revealed that administering AFQ056 does not affect the expression levels of the investigated blood biomarkers in young children with fragile X syndrome.
Conclusion:
Our findings of the lack of association between clinical improvement and biomarkers’ levels in the treatment group are in line with the lack of benefit observed in the FXLEARN study. These findings indicate that AFQ056 does not provide benefits as assessed by primary or secondary endpoints.
Registration:
ClincalTrials.gov NCT02920892.
Introduction
Fragile X syndrome (FXS) is the most prevalent cause of heritable intellectual disability (ID) and the most common monogenic cause of autism spectrum disorder (ASD).1,2 It is estimated that FXS affects approximately 1 in 4000 males to 1 in 8000 females. 3 The full mutation (FM) of the fragile X messenger ribonucleoprotein-1 (FMR1) gene, characterized by an expansion of CGG trinucleotide repeats (>200 CGG repeats), causes FXS. 4 This FM leads to the hypermethylation and transcriptional silencing of the FMR1 gene, resulting in a subsequent loss or substantial reduction in the production of the encoded protein, FMR1 protein (FMRP). FMRP is an essential messenger RNA (mRNA)-binding protein that regulates the translation of numerous proteins crucial for synaptic function and plasticity within dendritic structures. 5 The lack of FMRP leads to the disrupted synthesis of synaptic proteins, ultimately impairing synaptic plasticity and consequently to the clinical presentation of FXS.6,7
The clinical features of FXS vary between genders. Generally, males tend to exhibit more pronounced symptoms, whereas females often display a less severe phenotype due to the compensatory role of the unaffected active X chromosome. 1 Consequently, only about 25%–30% of females with FXS experience ID, while another 30% exhibit borderline IQ levels. Those individuals with FXS with an IQ in the neurotypical range often encounter emotional challenges or learning difficulties. 8 In general, FXS manifests as a diverse range of neurobehavioral conditions. These manifestations can be categorized as physical, psychological, or behavioral. Notably, over 80% of individuals with FXS exhibit distinctive physical characteristics, such as a lengthened face, prominent ears, a high palate, joint hypermobility, and the development of macroorchidism during or after puberty.1,9 In addition, the majority of individuals with FXS suffer from delayed speech and language development, social anxiety, shyness, atypical eye contact, heightened sensory sensitivity, attention deficit hyperactivity disorder (ADHD), aggressive behavior, sleep disturbances, seizures, hand flapping, repetitive behaviors, and, in some cases, obsessive-compulsive disorder (OCD). Seizures, particularly in those with ASD, occur in 15%–20% of those with FXS. 10
Despite years of preclinical investigations and clinical trials, there are currently no authorized treatments available for FXS. 11 In 2004, the metabotropic glutamate receptor (mGluR) theory emerged as an attempt to explain the clinical features observed in FXS. 12 FMRP has been demonstrated to play a crucial role in the translational control of target mRNAs in synaptosomes, functioning as a translational silencer or repressor, following the activation of group 1 mGluR (particularly mGluR1 and mGluR5) at the synapse.13,14 As a result of this process, the AMPA (α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid) receptors become internalized.15,16 Thus, the mGluR theory suggested that mGluR5 and FMRP have opposing roles in regulating mRNA translation at the synapse, with mGluR5 activation triggering protein synthesis, and FMRP inhibiting it. In FXS, where FMRP is absent, mGluR5-dependent protein synthesis occurs without restraint, resulting in the wide range of clinical features that characterize the syndrome. 17 Finally, there is a precise balanced relationship between FMRP and mGluRs. The absence of FMRP in neural cells leads to an upregulation of glutamate receptors. The synthesis of FMRP is boosted by the activity of mGluR5. This, in turn, acts as a negative feedback mechanism to control the activity of mGluR, creating a regulatory loop. 18 In addition, under normal conditions, the activation of mGluR1 and mGluR5 leads to the initiation of signaling pathways involving the extracellular signal-regulated kinase (ERK) and the mammalian target of rapamycin (mTOR).19,20 This eventually leads to the removal of the repressor function of FMRP at the ribosome, followed by a burst of new protein synthesis.18,21 Thus, FXS pathophysiology and disrupted signaling pathways encompass various pathways, including mTOR, ERK, microtubule-associated protein kinase (MAPK), and protein kinase A (PKA).12,16,21 These disruptions may play a role in the observed excessive metabotropic glutamate receptor-dependent long-term depression (mGluR-LTD) in FMR1 knockout (KO) mice and contribute to the neurobehavioral symptoms observed in FXS. 15 Furthermore, the deficiency of FMRP is linked to changes in the levels of several extracellular proteins, including matrix metalloproteinase 9 (MMP-9).5,22–24 More precisely, when mGluRs synaptic stimulation occurs, FMRP separates from the MMP-9 mRNA complex, enabling the translation of MMP-9 to take place. In FXS, the absence of FMRP results in the overexpression of MMP-9 (reviewed in Laroui et al. 25 and reported both in the FMR1 KO mouse model and human).5,23,26
Preclinical studies with animal models of FXS using mGluR5 negative allosteric modulators (NAMs) have been promising.27,28 Despite the findings in mouse models suggesting that learning and cognition should be the primary targets for mGluR5 NAMs in FXS, practical constraints such as regulatory considerations and the absence of robust cognitive assessments for FXS limited the focus on learning in initial human trials. However, it is worth noting that three Phase 2b studies showed significant placebo effects, and none demonstrated the efficacy of the drug over the placebo.29,30 An additional sub-study conducted within the Phase 2b trial did indicate that the drug engaged with its intended target. This sub-study revealed improvements in the group treated with NAM, such as AFQ056 (mavoglurant) in comparison with the placebo group, particularly in performance-based assessments, such as eye gaze behaviors during an eye tracking task and accuracy as well as a reduction in omissions in the Kiddie Test of Attentional Performance (KiTAP). 31
Recently, a large multi-site trial, FXLEARN (ClincalTrials.gov NCT02920892), investigated the impact of the mGluR5 NAM, AFQ056, on language improvement in children aged 3–6 with FXS. This age group was chosen due to the assumption that children during early development might exhibit greater learning plasticity compared to adults and show benefits not seen in unsuccessful previous trials of mGluR5 NAMs in adult populations. FXLEARN, however, did not show a significant difference between the AFQ056 and placebo-treated groups and suggested that better strategies are needed to determine which mechanisms will translate from pre-clinical models to humans in genetic neurodevelopmental disorders. 32 As with any clinical trial in which the findings are null as regards efficacy, the question remains as to whether there are effects at the neurobiological level that have not translated into more readily observable effects on the specific set of neurocognitive and behavioral functions measured in the trial. The current exploratory analyses from samples collected in FXLEARN aimed to determine whether AFQ056 affects the levels of potential molecular biomarkers associated with Akt/mTOR and MMP-9 signaling in young individuals with FXS.
Materials and methods
Study design
A double-blind placebo-controlled parallel-group flexible-dose forced-titration design of the FXLEARN study was recently described in detail. 32 The FXLEARN study enrolled participants between September 2017 and March 2020, and participants were randomized between January 2018 and July 2020. The last participants visit was in September 2021. Samples for blood biomarkers were collected during FXLEARN and analyzed as exploratory outcomes to identify potential blood biomarkers able to predict the efficacy of the AFQ056 target treatment. The study and all research protocols were carried out in accordance with the central Institutional Review Board (IRB) at Massachusetts General Hospital working with the Network for Excellence in Neuroscience Clinical Trials (NeuroNEXT). Records of central IRB approval were submitted to local IRBs at participating sites. Written informed consent was obtained from legally authorized representatives before the study.
Participants
Participants were children diagnosed with FXS and enrolled in the FXLEARN trial, from 13 sites, both sexes, aged between 3 and 6 years. Inclusion and exclusion criteria for the FXLEARN study were previously reported. 32
The FM of the FMR1 gene (CGG repeat size > 200) was confirmed within the project via Southern blot and PCR approaches. The participants all met entry criteria to be included in FXLEARN (details were described in the recent paper published by Berry-Kravis et al. 32 ). After a 4-month placebo lead-in, all participants were randomized in a 1:1 ratio to AFQ056 (other name: mavoglurant) or placebo, taken orally twice per day. Over 8 weeks, they titrated up to 100 mg twice a day or their maximum tolerated dose without significant side effects. Although blood samples were obtained from 101 FXS patients in total, biomarker analyses were performed on specimens derived from 63 patients who blood drawn was available at both 1- and 8-month visits (visit 1 and visit 9), marked as baseline and subsequent visits. See the diagram in Figure 1, which is adapted from a detailed FXLEARN Protocol Design published in 2023. 32

The adopted diagram of the FXLEARN protocol design. The diagram is adopted according to study design published by Berry-Kravis et al. 32
Biomarkers analyzed
Blood biomarker analyses included FMR1 genotyping, methylation status, and FMR1 mRNA, which were measured as previously described33–36 and markers known to be key proteins in the signaling pathways regulated by FMRP, whose expression is altered in FXS. Specifically, blood biomarkers analyzed included MMP-9 and targets of the Akt/mTOR signaling pathway (as described below).
MMP-9
Plasma specimens were acquired from vacuum blood collection tubes containing ethylenediaminetetraacetic acid. These samples were intended for the quantification of plasma MMP-9 expression, both prior to (baseline) and to a subsequent visit. MMP-9 was quantified by the Milliplex MAP Human MMP magnetic bead panel, named HMMP2MAG-55K (EMD Millipore Corp., Billerica, MA, USA), in strict adherence to the manufacturer’s protocols. This panel allows the assessment of both MMP-2 and MMP-9. In brief, calibrators, quality controls, and plasma samples were diluted in assay buffer and subsequently incubated with the antibody-magnetic beads mixture on pre-washed 96-well plates for 2 h. Following repeated washes of the plates, a biotinylated detection antibody was introduced and incubated for an additional hour. Subsequently, streptavidin–phycoerythrin concentrate was incorporated into the plates for 30 min. After repeated washes, the beads were resuspended on a plate shaker utilizing drive fluid (Luminex Corp., Austin, TX, USA) for a minimum of 5 min prior to the reading process. All washing steps were meticulously executed using an automated magnetic 96-well plate washer (Bio-Plex Pro Wash Station, Bio-Rad, Mississauga, ON, Canada). All incubation steps were conducted in a light-protected environment at room temperature on a plate shaker. Fluorescence measurements were performed using a Luminex instrument (Luminex Corp., Austin, TX, USA); MMP-9 levels were normalized with MMP-2 levels, and subsequent data analysis was carried out as previously described. 37
Akt/mTOR activity
Whole blood was collected using Cell Preparation Tube vacutainers containing sodium citrate (Becton Dickinson, Franklin Lakes, NJ, USA). Subsequently, the vacutainers were subjected to centrifugation, as per the manufacturer’s guidelines, to facilitate the separation of mononuclear cells from the whole blood. Peripheral blood mononuclear cells were isolated, washed with Dulbecco’s phosphate-buffered saline, and cryopreserved in RPMI 1640 medium containing 10% fetal bovine serum and 10% dimethyl sulfoxide. To evaluate the Akt/mTOR phosphor activity, a MILLIPLEX® MAP Akt/mTOR Phosphoprotein 11-plex Magnetic Bead Kit (Millipore, Burlington, MA, USA) was used to detect the phosphorylation levels of several crucial targets of this pathway. To determine the Akt/mTOR total activity, a MILLIPLEX® MAP Akt/mTOR total protein 11-plex Magnetic Bead Kit (Millipore, Darmstadt, Germany) was used. The 11 targets were: (i) Phosphorylated Ribosomal Protein S6 Kinase (p-70S6K, (Thr412)); (ii) Phosphorylated Insulin Receptor Substrate 1 (p-IRS1, (Ser636)); (iii) Phosphorylated Glycogen Synthase Kinase 3 Alpha (p-GSK3α, (Ser21)); (iv) Phosphorylated Glycogen Synthase Kinase 3 Beta (GSK3β, (Ser9)); (v) Phosphorylated Protein Kinase B (p-Akt, (Ser473)); (vi) Phosphorylated Phosphatase and Tensin Homolog (p-PTEN, (Ser380)); (vii) Phosphorylated Insulin Receptor (p-IR, (Tyr1162/Tyr1163)); (viii) Phosphorylated Insulin-like Growth Factor 1 Receptor (p-IGF1R, (Tyr1135/Tyr1136)); (ix) Phosphorylated Ribosomal Protein (p-S6 RPS6, (Ser235/Ser236)); (x) Phosphorylated Tuberous Sclerosis Complex 2 (TSC2, (Ser939)); and (xi) Phosphorylated Mammalian Target of Rapamycin (p-mTOR, (Ser2448)).
The optimal protein concentration (10 µg) was determined through preliminary analyses, and samples were subsequently diluted to a final volume of 25 μL in MILLIPLEX® MAP assay buffer. These diluted samples were mixed with 25 μL of 1 × bead mix within a 96-well plate. Several controls, including HeLa cell lysate: Phosphatase, HepG2 cell lysate: insulin, and MCF7 cell lysate: IGF1were included in the analysis. Additionally, blank wells, containing all assay components except for the protein, were prepared and added to the same plate. Subsequently, 25 μL of 1 × MILLIPLEX® MAP Detection Antibody was introduced into each well, and the plate was sealed and incubated at room temperature for 1 h with gentle shaking. After the incubation period, the excess detection antibody was removed, and 25 μL of 1 × MILLIPLEX® MAP streptavidin-phycoerythrin (SAPE) was added to each well. The plate was then incubated for an additional 15 min at room temperature with gentle shaking. Subsequent, to the SAPE/Amplification Buffer incubation, the excess solution was removed, and the beads were resuspended in 150 μL of MILLIPLEX® MAP Assay Buffer for 5 min with continuous shaking. All the reagents used for this assay were from Millipore, Darmstadt, Germany. The plate was read using a Luminex detection system (Luminex, Austin, TX, USA), and the data were analyzed accordingly.
Statistical analyses
Sample size calculations for FXLEARN trial were based on the key secondary endpoint of Mullen Scales of Early Learning (MSEL). Data from the observational study of Indah Winarni et al. (2012) were used, along with additional estimates of effect size (no raw data) from an unpublished pre-post randomized clinical trial. Indah Winarni et al. 38 extracted data from chart reviews for 45 FXS children aged 12–50 months. There is no disease modifying treatment for FXS, and there is an urgent need to develop therapeutics that show efficacy signal. In light of this, the alpha-level for sample size estimation was set to detection for any efficacy signal, measuring the alpha of the likelihood ratio test was set to detect ΔAIC > 0. The required N for the smallest effect proportion for expressive language (π = 1.43) and the required sample size with α = 0.16 is N ≈ 40 per arm. Therefore, a total of N = 100 (50 per group) was more than sufficient to detect any magnitude of efficacy (i.e., ΔAIC > 0). Because of high parental motivation, the dropout rate was anticipated to be extremely low. The calculation indicated that with total N = 100, power might be sufficient to detect ΔAIC > 0 with as much as 20% dropout (100–0.2 × 100 = 80, or 40 in each group for expressive language).
Gender and methylation status were compared between groups using Fisher’s exact test. The protein levels of the investigated markers, at baseline and subsequent visits, were compared using linear mixed effect models that included fixed effects for treatment, time, and their interaction, and a random intercept for subjects. Analyses were conducted using R version 4.2.1 39 and linear mixed effects models were fitted using the R package nlme, version 3.1-159. 40
Results
Characteristics of the study groups
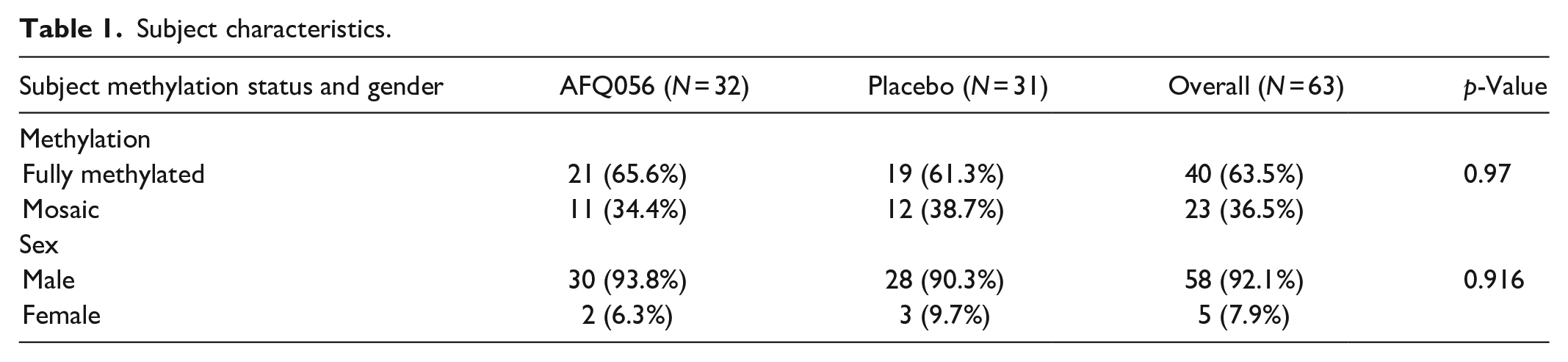
This research included 63 randomized participants diagnosed with FXS: 32 of them were given AFQ056 and 31 were on placebo. The gender and methylation status of the study’s participants divided by treatment group is presented in Table 1. Gender and methylation status were well balanced between groups and neither characteristic differed significantly.
Subject characteristics.
Differences between markers related to treatments
There were no significant biomarker changes over time in either treatment group, and no marker had a difference between treatment groups in its change over time. Detailed statistical results on fold changes over time in targets of the Akt/mTOR signaling pathway for all subjects are presented in Table 2.
Fold changes in targets of the Akt/mTOR signaling pathway between visits in markers for all subjects (N = 63) in AFQ056 (N = 32) and placebo (N = 31) groups.

p-GSK3β: phosphorylated glycogen synthase kinase 3 beta; p-IGF1R: phosphorylated insulin-like growth factor 1 receptor; p-IRS1: phosphorylated insulin receptor substrate 1; p-Akt: phosphorylated protein kinase B; p-mTOR: phosphorylated mammalian target of rapamycin; p-P70S6K: phosphorylated ribosomal protein S6 kinase; p-IR: phosphorylated insulin receptor; p-PTEN: phosphorylated phosphatase and tensin homolog; p-GSK3α: phosphorylated glycogen synthase kinase 3 alpha; p-TSC2: phosphorylated tuberous sclerosis complex 2; p-RPS6: phosphorylated ribosomal protein S6.
Differences between treatments (AFQ056 compared to placebo) in targets of the Akt/mTOR signaling pathway for all subjects and males at baseline and subsequent visit are presented in Supplemental Tables 1 and 2, respectively.
Analyses of changes over time in all listed biomarkers for male subjects only are presented in Supplemental Table 3.
The influence of methylation status on differences between markers related to treatments
MMP-9 did not differ significantly between treatments at either timepoint for either methylation status (AFQ056 vs placebo for fully methylated p = 0.47 and 0.19 at baseline and subsequent visit, respectively; AFQ056 vs placebo for partially methylated p = 0.09 and 0.71 at baseline and subsequent visit, respectively). Similarly, regardless of methylation status, MMP-9 did not change significantly over time in either treatment group (baseline vs subsequent visit for fully methylated p = 0.82 and 0.46 in AFQ056 and placebo group, respectively; subsequent visit vs baseline for partially methylated p = 0.57 and 0.11 in AFQ056 and placebo group, respectively).
In addition, differences between treatments (AFQ056 vs placebo) in marker phosphorylation related to Akt/mTOR activity for all subjects broken down by methylation status showed that p-TSC2 was significantly higher at subsequent visits in fully methylated subjects treated with AFQ056 compared to fully methylated subjects treated with placebo (p = 0.036). Note, however, that the difference in p-TSC2 between AFQ056 and placebo at subsequent did not differ significantly between fully methylated and partially methylated subjects (treatment–methylation interaction effect p = 0.19).
Statistical analyses of changes over time (baseline vs subsequent visit) in markers of Akt/mTOR activity by methylation status for all subjects revealed that the change in p-P70S6K between baseline and subsequent visit differs marginally significantly between AFQ056 and placebo in fully methylated subjects (treatment–time interaction effect p = 0.0408), although neither treatment group changed significantly over time for these subjects. p-P70S6K changes significantly between baseline and subsequent visits in the AFQ056 group for mosaic subjects (p = 0.015); however, this change over time did not differ significantly between treatment groups (treatment–time interaction effect p = 0.35). Finally, the difference between treatment groups in the change over time in p-P70S6K differs marginally significantly between fully methylated and mosaic (partially methylated) subjects (treatment–time–methylation interaction effect p = 0.05). Finally, p-TSC2 changes significantly between baseline and subsequent visits in the AFQ056 group for mosaic subjects (p = 0.01); however, this change over time did not differ significantly between treatment groups (treatment–time interaction effect p = 0.13).
Discussion
This research revealed that administering AFQ056, an mGluR5 NAM, does not affect the levels of investigated blood biomarkers in young children with FXS. The blood levels of some of the key proteins in the signaling pathways regulated by FMRP and, known to be abnormal in FXS, were the primary endpoint/outcome measure in this investigation. Although this research included young children characterized by higher neural plasticity and adaptability and utilized objective measures less susceptible to the placebo effect, AFQ056 did not affect the levels of any biomarkers we investigated. However, there were unexpected results such as a significant decrease in the levels of p-Akt in the placebo group, but not in the AFQ056 group, as well as a significant decrease in levels of p-P70S6K in the placebo group, but not in the AFQ056 group.
Among other biomarkers, the focus of this investigation was on the effect of AFQ056 on the MMP-9 plasma levels in the included participants. MMP-9 is an enzyme responsible for encoding an endopeptidase that plays a vital role in dendritic spine maturation and synaptic formation. In FXS, MMP-9 levels are increased due to the absence of FMRP, which inhibits the translation of MMP-9 mRNA 23 in both the FXS mouse model and in humans. 26
The expectation that AFQ056 treatment could affect MMP-9 plasma levels is based on preclinical studies with minocycline and metformin. Minocycline treatment showed to restore MMP-9 levels to normal levels 41 and, in the FMR1 KO mice, showed to improve dendritic spine maturation, synapse formation, anxiety levels, cognitive performance, and even ultrasonic vocalizations.42,43 Such investigations paved the way for a successful clinical trial of minocycline in FXS treatment. Furthermore, treatment with metformin reduced MMP-9 levels in FMR1 KO mice. 44 However, AFQ056 treatment did not affect MMP-9 plasma levels in the current study. In addition, AFQ056 did not change the level of Akt/mTOR pathway activity in young children with FXS. One potential explanation for the absence of observed changes in biomarkers could be attributed to the distinct expression patterns of these biomarkers in blood and brain tissues. There are significant challenges in using blood biomarker expression levels because their levels may not accurately reflect the intracellular neuronal values that could be more directly associated with brain function. However, altered expression of targets of the mTOR pathway has been demonstrated in peripheral blood from subjects with FXS. 48 Results obtained in this investigation, which revealed no changes in the levels of the investigated biomarkers induced by AFQ056, are in agreement with the FXLEARN clinical trial published results, which revealed that there were no benefits on language learning for the FXS 3 to 6-year-old children AFQ056 group. 32
Furthermore, in the present study, we did not observe any AFQ056 effect, on any of the biomarkers, regardless of the methylation status. Interestingly, Jacquemont et al. 49 described that AFQ056 improved behavior in some fully methylated individuals with FXS, while those who were mosaics with a partial methylation pattern had a variable response with a lack of overall efficacy. There was no explanation for the varying responses observed, where some individuals lacking methylation responded while others did not. This was also the case in a recent clinical trial of cannabidiol in FXS that showed significant improvements in measures of social avoidance, irritability, and social interaction, but only in those with ⩾90% methylation of the FMR1 gene. 50
In preclinical research studies, the correction of synaptic plasticity and morphological issues in animal models of FXS using mGluR5 NAMs has been associated with a return to normalcy in learning capabilities.27,51 Michalon et al. 27 demonstrated that chronic treatment with long-acting mGlu5 inhibitor decreased ERK activity and mTOR phosphorylation levels in FMR1-KO mice, while such changes were not observed in the WT mice. This effect was more pronounced and comprehensive in younger, preadolescent animals when compared to adult mice. 27 The extent of improvement was also linked to the duration of treatment. Furthermore, certain behavioral characteristics, such as anxiety and perseverative behavior, showed signs of improvement in these studies.27,28 However, these improvements were not consistently as significant as those observed in synaptic functions and tended to be influenced by experimental variables like the mouse strain, environment, and laboratory conditions.27,28,51 In addition, some neural signaling pathways in animal models of FXS may exhibit greater conservation and relevance when extrapolated to humans, whereas others have changed, becoming less significant and less applicable to human translation. For example, recent research has revealed varying reactions of human iPSC-derived neurons to mGluR5 NAMs when compared with mouse neurons, 52 and there is evidence of the absence of favorable outcomes for mGluR5 NAMs in human FXS iPSC-derived cerebral organoids. 53 The findings from such studies can be highly informative when determining which investigated mechanisms of action of targeted treatments in FXS may be utilized in clinical trials. In addition, preclinical research with lovastatin demonstrated that it blocks the ERK/MAPK pathway using model HIRcB cells, a rat fibroblast cell line.45,46 Metformin has also been demonstrated to lower ERK signaling and reduce the levels of p-EIF4E in the FMR1-KO mouse. 44 In the Drosophila model of FXS, metformin can also ameliorate FXS characteristics by mitigating the up regulation of the mTOR pathway typically observed in FXS. 47
This result corresponds to the negative FXLEARN trial results with no benefit of AFQ056 on any primary and secondary endpoints. 32 Finally, consideration could be given to a recent study in mice that offers significant proof that this potential treatment for FXS was ineffective because the brain develops resistance, or “tolerance” to it. Stoppel et al. 54 suggested that, besides the approach of giving mGluR5 inhibitors at a young age and then discontinuing them, patients might also benefit from a dosing regimen that includes breaks to prevent resistance from building up. Furthermore, the study indicates that, despite treatment resistance, FMR1 KO mice began synthesizing an unknown protein that causes symptoms. Authors noted that identifying and targeting this protein could provide a promising new direction for drug development. Our findings strongly suggested that further preclinical and clinical studies are needed to answer important questions from the failed fragile X mGluR5 trials.
The limitation of this research includes a restricted number of samples available for biomolecular analyses. The negative findings at both the clinical 32 and the molecular level point to the lack of efficacy of AFQ056 in FXS. There is also learning for groups working on other neurodevelopmental conditions around the choice of biomarkers.
Conclusion
Our findings on the lack of association between clinical improvement and biomarkers’ levels in the treatment group are in line with the lack of benefits observed in the FXLEARN study. These findings indicate that AFQ056 does not provide benefits as assessed by primary or secondary endpoints in children diagnosed with FXS, both sexes, aged between 3 and 6 years.
Supplemental Material
sj-doc-1-smo-10.1177_20503121241282401 – Supplemental material for Negative effect of treatment with mGluR5 negative allosteric modulator AFQ056 on blood biomarkers in young individuals with Fragile X syndrome
Supplemental material, sj-doc-1-smo-10.1177_20503121241282401 for Negative effect of treatment with mGluR5 negative allosteric modulator AFQ056 on blood biomarkers in young individuals with Fragile X syndrome by Dragana Protic, Elizabeth Breeze, Guadalupe Mendoza, Marwa Zafarullah, Leonard Abbeduto, Randi Hagerman, Christopher Coffey, Merit Cudkowicz, Blythe Durbin-Johnson, Paul Ashwood, Elizabeth Berry-Kravis, Craig A Erickson, Robin Filipink, Andrea Gropman, Lenora Lehwald, Angela Maxwell-Horn, Stephanie Morris, Amanda Palladino Bennett, Lisa Prock, Amy Talboy, Nicole Tartaglia, Jeremy Veenstra-VanderWeele and Flora Tassone in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241282401 – Supplemental material for Negative effect of treatment with mGluR5 negative allosteric modulator AFQ056 on blood biomarkers in young individuals with Fragile X syndrome
Supplemental material, sj-docx-2-smo-10.1177_20503121241282401 for Negative effect of treatment with mGluR5 negative allosteric modulator AFQ056 on blood biomarkers in young individuals with Fragile X syndrome by Dragana Protic, Elizabeth Breeze, Guadalupe Mendoza, Marwa Zafarullah, Leonard Abbeduto, Randi Hagerman, Christopher Coffey, Merit Cudkowicz, Blythe Durbin-Johnson, Paul Ashwood, Elizabeth Berry-Kravis, Craig A Erickson, Robin Filipink, Andrea Gropman, Lenora Lehwald, Angela Maxwell-Horn, Stephanie Morris, Amanda Palladino Bennett, Lisa Prock, Amy Talboy, Nicole Tartaglia, Jeremy Veenstra-VanderWeele and Flora Tassone in SAGE Open Medicine
Footnotes
Acknowledgements
A particular thanks to all patients participating in the study who have made this research possible. This work is dedicated to the memory of Matteo.
Author contributions
Dragana Protic: formal analysis, writing—original draft. Elizabeth Breeze: data curation; writing—review and editing. Guadalupe Mendoza: data curation; writing—review and editing. Marwa Zafarullah: data curation, writing—review and editing. Leonard Abbeduto: investigation; writing—review and editing. Randi Hagerman: investigation, writing—review and editing. Christopher Coffey: investigation; writing—review and editing. Merit Cudkowicz: investigation; writing—review and editing. Blythe Durbin-Johnson: formal analysis, software, writing—review and editing. Paul Ashwood: investigation, writing—review and editing. Elizabeth Berry-Kravis: writing—review and editing, conceptualization, methodology, investigation. Craig A Erickson: investigation, writing—review and editing. Robin Filipink: investigation, writing—review and editing. Andrea Gropman: investigation, writing—review and editing. Lenora Lehwald: investigation, writing—review and editing. Angela Maxwell-Horn: investigation, writing—review and editing. Stephanie Morris: investigation, writing—review and editing. Amanda Palladino Bennett: investigation, writing—review and editing. Lisa Prock: investigation, writing—review and editing. Amy Talboy: investigation, writing—review and editing. Nicole Tartaglia: investigation, writing—review and editing. Jeremy Veenstra-VanderWeele: investigation, writing—review and editing. Flora Tassone: writing—review and editing, conceptualization, methodology, supervision.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dragana Protic has received funding from The Science Fund of the Republic of Serbia and the FRAXA Research Foundation for carrying out studies on Fragile X Syndrome. Flora Tassone has received funding from Zynerba and Azrieli Foundation for carrying out studies on Fragile X Syndrome. Elizabeth Berry-Kravis has received funding from Acadia, Biogen, BioMarin, Erydel, GeneTx/Ultragenyx, Ionis, Jaguar, Kisbee, Neuren, Neurogene, Orphazyme/Kempharm/Zevra, PTC Therapeutics, Roche, Taysha, Tetra/Shionogi, Yamo, Zynerba, and Mallinckrodt Pharmaceuticals, for consulting or on clinical trials in genetic neurological disorders, all funds directed to Rush University Medical Center. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NeuroNEXT network NIH grants U01NS096767, U24NS107200, U24NS107209, U01NS077323, U24NS107183, U24NS107168, U24NS107128, U24NS107199, U24NS107198, U24NS107166, U10NS077368, U01NS077366, U24NS107205, U01NS077179, and U01NS077352, NIH grant P50HD103526, and Novartis IIT grant AFQ056X2201T for provision of AFQ056.
Ethics approval and consent to participate
The study and all research protocols were carried out in accordance with the central Institutional Review Board (IRB) at Massachusetts General Hospital working with the Network for Excellence in Neuroscience Clinical Trials (NeuroNEXT; NeuroNEXT; NN107 Insight Protocol #: 2016P001804; Mass General Brigham IRB #s: IRB00012706 and IRB00012707). Records of central IRB approval were submitted to local IRBs at participating sites.
Informed consent
Written informed consent was obtained from legally authorized representatives before the study.
Consent for publication
All authors gave their consent for publication.
Trial registration
ClincalTrials.gov NCT02920892.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.