
Abstract
Objectives:
The purpose of this scoping review is to explore research studies on the association between chronic pain and polycystic ovary syndrome to create local (U.S.-based) and global recommendations to improve access to and quality of affordable symptom management and treatment options for patients with polycystic ovary syndrome.
Methods:
The study sections used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews as a checklist reference. The review followed the York methodology by Arksey and O’Malley for the extraction, analysis, and presentation of results in scoping reviews.
Results:
Final analysis included two conference abstracts published in peer-reviewed journals and two peer-reviewed articles. The relationship between pain perception and health-related quality of life warrants further investigation in patients with polycystic ovary syndrome as the interconnected pathophysiology of symptoms renders exploring associations between the two factors difficult. A comprehensive understanding of the causes of polycystic ovary syndrome-associated symptoms, particularly those relating to pain perceptions can provide more insight into polycystic ovary syndrome pathophysiology and aid in the development of innovative therapeutic approaches for long-term polycystic ovary syndrome management and care.
Conclusion:
Future studies are necessary to examine associations between the disease and pathophysiological symptoms for a better quality of life for patients with polycystic ovary syndrome.
Synopsis:
More research studies are necessary to examine associations between polycystic ovary syndrome and chronic pain for a better quality of life for the population dealing with polycystic ovary syndrome.
Background
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder estimated to affect 6%–20% of childbearing age women worldwide. 1 It is estimated to affect at least 5 million women in the United States and cost the U.S. health care system approximately $4 billion annually. 2 Multiple comorbidities associated with PCOS include obesity, type 2 diabetes mellitus, metabolic syndrome, infertility, nonalcoholic steatohepatitis, obstructive sleep apnea, eating disorders, anxiety, and depression.3–5
In addition to an increasing risk for various morbidities, PCOS causes chronic pain. 6 Chronic pain has been defined as pain lasting more than 3 months. 7 In a qualitative study exploring the relative importance of PCOS symptoms and impact concepts to patients as compared to physicians, patients with PCOS report pain- and discomfort-related symptoms as having the most significant impact on emotional well-being (anxiety/stress) and coping behaviors (acne, medication, hair removal). 8 These symptoms include cramping, heavy bleeding, and bloating; however, the cramping is not always associated with menstruation due to the possibility of irregular periods and amenorrhea. 9 Additionally, even though the concept group of pain and discomfort accounted for the highest proportions of symptoms expressed by patients with PCOS, bodily pain, chronic pain, and associated symptoms were disregarded by clinicians and were not considered relevant or important to patients with this syndrome. 10 Pain symptoms in PCOS have been investigated using the Health-Related Quality of Life (HRQoL) Questionnaire and the Short Form-36, two commonly used quality-of-life patient-reported outcomes. 8 Multiple studies have demonstrated that patients with PCOS repeatedly score lower on questions in the pain domain within the 36-item Short Form Health Survey (SF-36) that has been used to evaluate HRQoL in PCOS patients, indicating that pain is a significant factor in the limited quality of life.10–12 Additionally, several research studies have reported that inflammation plays a key role in the development and maintenance of several types of pain extending from the peripheral to the central nervous systems.13–15 It was also reported that the association of chronic systemic inflammation and pain sensitivity is highly involved in the development and maintenance of chronic pain.13–15 Such proinflammatory status was seen to intensify pain perceptions in patients with PCOS.14,15 Quite visibly, there is a dearth of evidence for treatment directly addressing chronic pain in PCOS. 9 Although pain- and discomfort-related complaints are common among patients with PCOS, clinicians often overlook this aspect, regarding it only as a PCOS symptom and not an additional point of treatment. 9 Therefore, there is a crucial need for research to further explore and treat chronic pain in patients with PCOS.
Currently, the scope of the research studies exploring chronic pain symptoms among PCOS women of childbearing age is very limited. The purpose of this scoping review is to explore research studies on the association between chronic pain and PCOS to create local (U.S.-based) and global recommendations to improve access to and quality of affordable symptom management and treatment options for patients with PCOS.
Methods
The study sections used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) as a checklist reference. The review followed the York methodology by Arksey and O’Malley and incorporated recommendations from the Joanna Briggs Institute (JBI) for the extraction, analysis, and presentation of results in scoping reviews.
Step 1. Identify research questions
Two guiding research questions or the scoping review were: (1) Which research studies examined the association between chronic pain and PCOS among females of reproductive age? (2) What are the current local (U.S.-based) and global recommendations to improve access to and quality of affordable symptom management and treatment options for patients with PCOS?
Step 2. Search for relevant studies
Keywords were developed in collaboration with a research librarian (MK) experienced in systematic review protocols. The search terms focused on: PCOS, ovary polycystic disease, cystic ovary, Stein-Leventhal disease, polycystic ovary disease, chronic persistent pain, and chronic intractable pain. Four online databases (PubMed, Embase, Web of Science, and Cochrane) were selected, and review of the literature took place between April 2023 and June 2023. Screening of the articles carried out by senior author (LS) and co-authors (GO, AM, SD) (Figure 1).
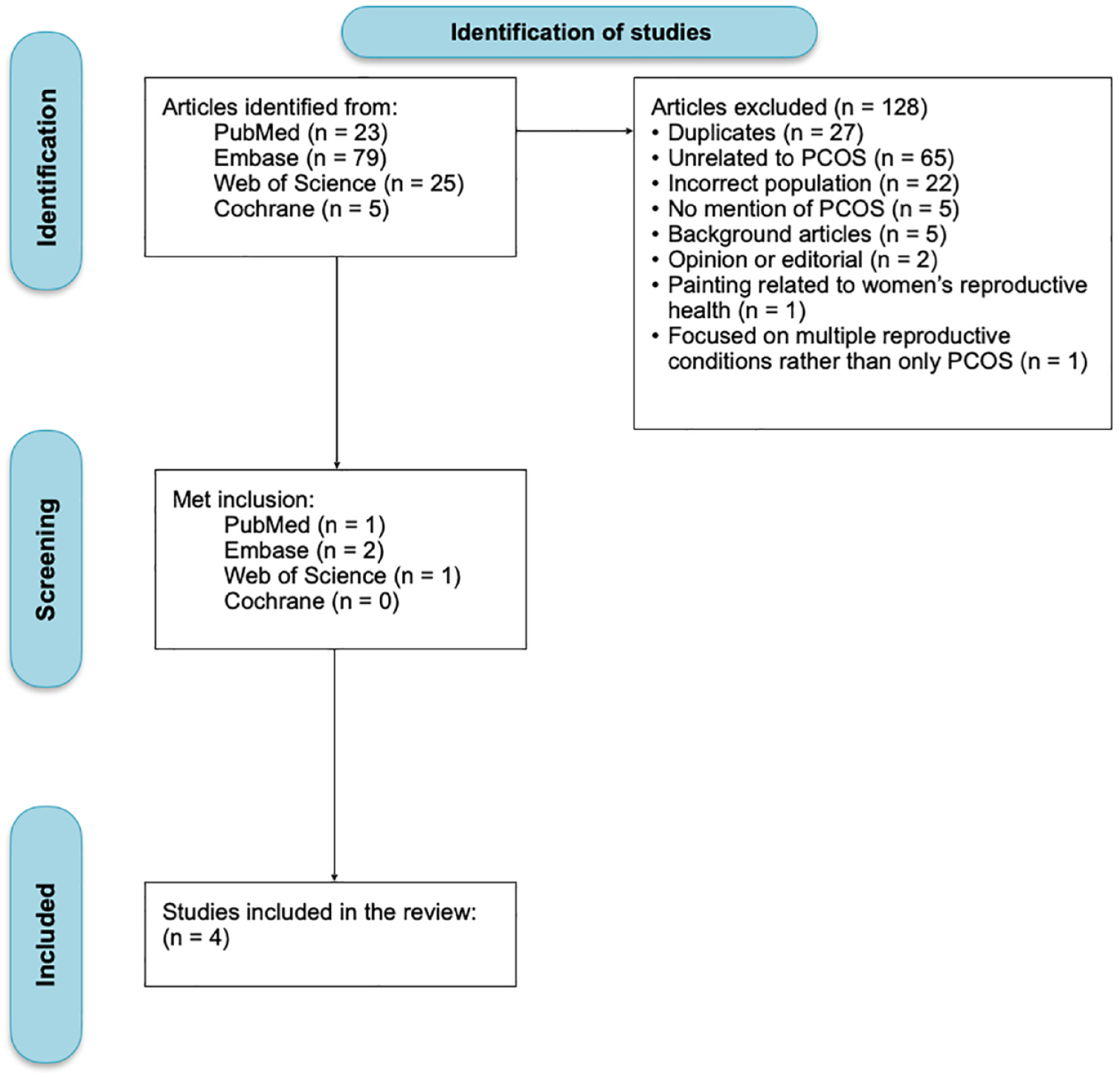
Study selection process.
Inclusion criteria
Included studies were published between 2013 and 2023, due to the relative novelty of the association between chronic pain and PCOS reported in the literature. Included studies were also published in English, described PCOS-associated symptoms and/or chronic pain in women of childbearing age, focused on exploring associations between PCOS, and reported pain symptoms among females affected with the syndrome. All types of qualitative, quantitative, experimental, review, and descriptive studies (including case reports and case series) were considered for inclusion. Published conference abstracts were also included if they satisfied the inclusion criteria. Women of childbearing/reproductive age were defined as adult women aged between 18 and 49 years old.
Exclusion criteria
Excluded studies were unrelated to the desired health outcome or condition, did not match the desired target population, had no mention of PCOS, were background articles, editorials, and opinion statements, and covered multiple chronic conditions rather than focusing on PCOS solely.
Step 3. Selection of studies relevant to the research questions
All co-authors (GO, AM, SD) extracted data and summarized data as major findings for overview of quality-of-life of PCOS in women of childbearing age and role of chronic pain in aggravation of PCOS symptoms.
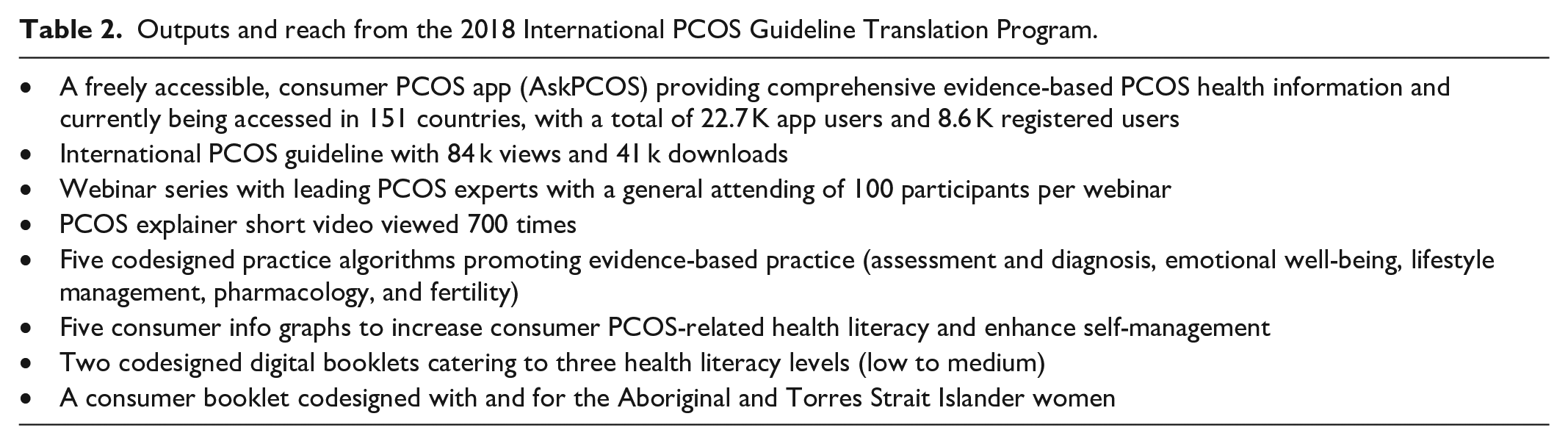
Summary tables included one listing study characteristics and major findings (Table 1) and one highlighting Outputs and Reach from the 2018 International PCOS Guideline Translation Program (Table 2). Table 3 lists the Aims and Principles of the 2023 International PCOS Guideline Update for future recommendations on how to effectively manage PCOS-associated symptoms.
Study characteristics.

Outputs and reach from the 2018 International PCOS Guideline Translation Program.
Aims and principles of the 2023 International PCOS Guideline update.

Steps 4 and 5. Data charting and collation, summarization, and reporting of results
Results were reported based on associations examined between PCOS and chronic pain symptoms. Provided were considerations for standardized global measurement tools to diagnose PCOS and associated symptoms, including chronic pain and mental health impact, as well as recommendations for PCOS to Improve International Access to Affordable and Quality Treatment for Women with PCOS with the intention to inform the translation of evidence on the disease and its associated comorbidities into action for a better quality of life for individuals affected with this syndrome.
Results
During the initial screening process, 132 articles were identified from April to June 2023. Among these, 79 articles were obtained from Embase (n = 79), 25 articles from Web of Science (n = 25, including 8 duplicates), 23 articles from PubMed (n = 23, including 17 duplicates), and five articles from Cochrane (n = 5, including 2 duplicates). A total of 65 articles were excluded due to being unrelated to the desired health outcome or condition (n = 65). Additionally, 22 articles did not match the desired target population (n = 22), and five articles did not mention PCOS (n = 5). Furthermore, five articles were considered background articles (n = 5), two were opinion or editorial pieces (n = 2), and one article described a painting related to women's reproductive health (n = 1). Lastly, one article covered multiple reproductive conditions instead of focusing solely on PCOS (n = 1). After removing the duplicates from the initial screening (n = 27) and excluding articles during the secondary screening (n = 101), the final analysis included two conference abstracts published in peer-reviewed journals16,17 and two peer-reviewed articles6,18 (Figure 1). Study characteristics and major findings were tabulated in Table 1 and summarized below.
Overview of quality-of-life of PCOS in women of childbearing age
Commonly diagnosed by hyper and rogenism, polycystic ovary morphology, and ovulatory dysfunction, PCOS can drastically reduce the quality of life. 19 Acne, hirsutism, amenorrhea, insulin resistance, obesity, and infertility are specific PCOS-related symptoms most cited to have a detrimental impact on quality of life.6,16 The SF-36 has been used to evaluate HRQoL in various patient populations, including women and females of reproductive age.6,20,21 When comparing scores between a healthy control group and females with PCOS, results have consistently revealed statistically significant differences in every area of HRQoL regardless of the PCOS symptom profile. 6 Additionally, the SF-36 data showed that patients with PCOS across multiple populations scored lower in areas relating to both mental and physical quality of life. 6 For instance, PCOS patients in Denmark consistently reported lower sexual satisfaction scores than controls, but additional research is warranted to isolate the cause. 22 Further studies have used the Revised Life Orientation Test to reveal severely impaired optimism of patients with PCOS compared to controls. 23 In Spain, a study revealed that hirsutism and weight gain were the central factors affecting HRQoL in women with PCOS. 24 Alongside obesity and hirsutism, bodily pain represented the most common disturbance to quality of life (QoL) for patients with PCOS.6,17 SF-36 survey in the United Kingdom showed that pain scores in patients with PCOS were 14% lower than those of healthy controls. 6 Elevated body mass index (BMI) has also been established as a crucial factor influencing pain perception and adjusting for BMI between the two study groups revealed no statistically significant difference in HRQoL or pain perception.6,16 The relationship between pain perception and HRQoL warrants further investigation in patients with PCOS as the interconnected pathophysiology of symptoms renders exploring associations between the two factors difficult.
Role of chronic pain in aggravation of PCOS symptoms
Pain and discomfort-related symptoms are among the most frequent QoL-related complaints from women and females of reproductive age with PCOS.6,16,25 Additionally, an SF-36 survey of PCOS patients in Poland indicated that women with PCOS had significantly greater pain perception scores than healthy controls. 26 This was further demonstrated by a German study that enrolled 423 patients with PCOS. 27 While the presence of chronic pain in patients with PCOS is well established, the pathophysiological cause is difficult to isolate given the variable symptom profile.6,18 Proinflammatory PCOS pain further connects to obesity, a major symptom seen in approximately 50%–80% of patients with PCOS. 6 While researchers have demonstrated elevated pressure pain threshold (PPT), serum endorphins, and CRP in lean patients with PCOS, suggesting chronic pain and inflammation independent of obesity, there is a well-established connection between obesity and proinflammatory states.6,16,18 The precise relationship between PCOS chronic pain and abnormal adiposity requires further investigation, but obesity remains a risk factor for worsening chronic pain in PCOS states.6,16,18 Insulin resistance (IR) is a prevalent symptom of PCOS yet to be evaluated in the development of chronic pain. Although pain induction is controversial, the relationship between IR and chronic pain conditions (i.e., fibromyalgia) is well established. The administration of metformin, a first-line medication for type 2 diabetes with IR, has been seen to provide pain relief in chronic pain conditions (e.g., fibromyalgia, rheumatoid arthritis). 6 Hence, IR may be a source or risk factor for worsened pain development in patients with PCOS.
Discussion
Vulnerable female population subgroups with PCOS in the United States
In the United States, PCOS has significant public health importance with a high prevalence of metabolic syndrome and diabetes as associated comorbidities, along with long-term health consequences of cardiovascular disease (CVD). 28 Specifically, racial and ethnic minorities in the nation are more susceptible to having the severe phenotype form of the disease.28,29 A study by Engmann et al. 28 showed that Hispanic women with PCOS had more serious symptoms of hyperandrogenism and metabolic criteria as compared to non-Hispanic Black women and non-Hispanic White women. The high prevalence of the metabolic syndrome reported in Hispanic women with PCOS is mostly attributed to a higher prevalence of obesity, IR, and diabetes. 29 However, Asian and Native American, and multiracial individuals are often neglected in studies exploring chronic pain and other PCOS-associated comorbidities in the U.S. 30 Future studies should encompass a broader range of racial and ethnic groups for a more holistic and comprehensive understanding of the role that race and ethnicity plays on the expression of such syndrome. 30
Aside from genetic racial and ethnic vulnerabilities, female students in the medical field are more likely to suffer from the complications of PCOS since the majority of women graduating from medical school were reported to face unique stressors not seen with their male counterparts. 31 According to a recently published review study by Coffin et al., 31 the pooled prevalence across 11 included studies of 2206 female medical students diagnosed with PCOS was 24.7%, which is significantly higher than the estimated global prevalence of PCOS of 6%–7%. These findings were supported by other global studies on female students enrolled in diverse STEM and non-STEM majors.32,33 For instance, among female students taking health sciences courses in South India, 91.3% were diagnosed with PCOS. 34 Similarly, the prevalence of PCOS syndrome among Omani women in the Middle Eastern region was estimated at 7% in a hospital-based study. 35 Moreover, in Iran, a cross-sectional descriptive study of 636 female students attending the Kerman University of Medical Sciences identified a PCOS prevalence rate in the sample of 11.5%. 36 These results strongly emphasize the role of academic institutions in bridging the knowledge gap on the prevalence of PCOS and the particular health impact on the lives of the women affected. 36
Furthermore, Active-Duty Service Women (ADSW) were highlighted in the literature as being at high risk for severe PCOS comorbidities, particularly when it comes to the syndrome’s impact on their readiness in the field through adverse mental and physical consequences.37,38 In 2019, a retrospective analysis of the 2011–2016 electronic health record data from the Department of Defense showed that 11,190 ADSWs from all branches and ranks and aged 18–61 were diagnosed with PCOS. Moreover, 9112 (0.17%) were diagnosed with symptoms that meet the profile and characteristics present in PCOS but had no diagnosis. Despite the high prevalence rate of PCOS among ADSW, it is still lower than the prevalence rate of the syndrome in the U.S. population. 38 This may be either due to women, who were disqualified from entering the service because of having an increased abdominal girth or a pre-military diagnosis of PCOS, or due to women who have neglected PCOS symptoms to avoid raising concerns to military health care providers and the risk of compromising their career. 38 Hence, there is a need for active involvement from key public health stakeholders to address this condition in the military population while mitigating its consequences compromising the health, operational, and deployment readiness of these women.
New international guideline recommendations define PCOS as a high-risk condition in pregnancy. 39 Pregnant females exhibit higher vulnerability to PCOS complications, including difficulty in conceiving, having a miscarriage, hypertensive disorders, gestational diabetes, and premature birth.40,41 As a result, PCOS has profound implications for women and their offspring in the short term on reproductive function and in the longer term on the risk of chronic illnesses and congenital anomalies. 40 Moreover, as of 2020, the additional total healthcare-related economic burden of PCOS due to pregnancy-related and long-term morbidities in the United States is estimated to be around $4.3 billion on an annual basis. 42 Adequate support should be provided to support lifestyle changes during pregnancy and ensure these women adhere to adequate treatment and interventional methods when necessary.43,44
Although, outside the scope of this study’s target population, perimenopausal and menopausal females with PCOS are also an under-researched group suffering from symptoms and chronic pain associated with the syndrome.45,46 Ovarian androgen secretion capacity declines with age in both healthy women and in women with PCOS; however, it remains enhanced in females and individuals with PCOS until the late reproductive years. 47 Hence, unfavorable hormonal and metabolic changes, which are experienced during menopause, will more likely be exacerbated by hyperandrogenism in PCOS patients. 25 Additionally, individuals with PCOS were more likely to exhibit signs of IR through increased insulin responses in oral glucose tolerance tests before and after menopause. 25 However, the significant heterogeneity of the results, along with the low quality of the evidence from studies carried out on perimenopausal and menopausal females and individuals with PCOS, hinders reaching definite conclusions on the best methods of treatment to adopt.48,49 Therefore, there is a need for evidence-based research studies, including experimental studies, for appropriate guidance on most suitable measures to be adopted by these women.48,49
Considerations for measuring, treating, and managing chronic pain in PCOS patients
Despite the diversity of PCOS-related pathologic factors exacerbating pain perception among females with this syndrome, the questionnaires available to assess chronic pain PCOS symptoms have failed to evaluate the various dimensions of pain expression including pain type, potential causes, location, frequency, and pain scores.50–52 For instance, the current HRQoL survey format is limited in its capacity to obtain holistic perceptions of PCOS patients toward the pain they experience from their condition. Additionally, the survey designed specifically for patients with PCOS, known as the PCOS HRQoL questionnaire (i.e., PCOSQ), excludes pain perception. 6 Hence, the association between chronic pain and PCOS remains unclear. Future studies are required not only to examine the correlation between PCOS and chronic pain but also to determine whether the pathophysiology of PCOS exacerbates pain development and maintenance. 6
Mental health status of PCOS females experiencing chronic pain symptoms was also highlighted in the literature, whereby mental status was seen to have a bidirectional association with pain perception as risk factors and comorbidities for each other.53–57 Mental disorders such as fear, depression, anxiety, and stress contribute to experiencing an increased level of severe pain symptoms. 55 Although mental disorders were consistently reported as a dominant aspect of the lives of patients with PCOS in several HRQoL surveys, the bilateral link between physical problems and mental disorders should be further examined through experimental studies to enhance the management of psychological factors adversely affecting health outcomes of patients with PCOS.54,56 Furthermore, HRQoL surveys designed for patients with PCOS should encompass a section assessing all possible causes of pain and the influence of pain on the QoL of PCOS patients.56,57 Such surveys could provide clinicians with a better understanding of problems associated with PCOS to develop patient-centered strategies for appropriate intervention. 54 Due to the high association of negative mental health and PCOS, the international evidence-based guidelines developed by Monash University on behalf of the National Health and Medical Research Council, Centre for Research Excellence in PCOS, and the Australian PCOS Alliance recommend all adults with PCOS should be routinely screened for anxiety and depressive symptoms at diagnosis. 58 A comprehensive understanding of the causes of PCOS-associated symptoms, particularly those relating to pain perceptions can provide more insight into PCOS pathophysiology and aid in the development of innovative therapeutic approaches for long-term PCOS management and care. 58
Global recommendations to improve international access to affordable and quality treatment for women with PCOS
Many physicians are unfamiliar with the diagnostic criteria for PCOS, leaving many patients dissatisfied with the care received.59–61 This barrier was also reported in other continents, including Canada, Australia, and Europe, where patients with PCOS continue to urge their primary care providers, endocrinologists, and gynecologists to become well-versed on how to diagnose and manage PCOS to prevent delays in diagnosis and provide easier access to care.62–64 To exacerbate this situation further, funding for research on PCOS appears to be very limited in scope relative to its prevalence and its economic consequences. 65 PCOS was also excluded from the Kennedy Shriver National Institute of Child Health and Human Development (NICHD) 2020 Strategic Plan, the principal funding agency for PCOS research in the United States, thus hindering accurate prioritization of this disorder as a public health interest. 66 Furthermore, the financial burden of this syndrome is amplified after considering the cost of the initial evaluation and treatment of reproductive endocrine disorders (menstrual dysfunction/abnormal uterine bleeding, hirsutism, and infertility). 42 The economic analysis carried out by Riestenberg et al. 42 estimated the burden to increase to $8 billion annually when combined with these additional costs. Such findings emphasize the need for greater clinician vigilance and public awareness, along with more holistic screening measures and early diagnosis, to ameliorate the economic, health, and QoL of U.S. females with PCOS. 42
Given the distressing symptomology of PCOS, patients deserve affordable and quality treatment. Fortunately, some interventions show promise.6,17,18,67 Lifestyle modification remains first-line in PCOS treatment. 9 Regular physical activity and a healthy diet can address the health concerns surrounding PCOS, such as IR and hyperlipidemia. 9 Additionally, these lifestyle changes increase sex hormone binding globulin, decrease androgen levels, assist with weight management, and lower blood pressure. 9 Moreover, a Swedish study recommends acupuncture as a possible treatment for the IR characteristic of PCOS. 17 Electroacupuncture, whether in a single application or through 5 weeks of treatment, has improved glucose regulation in females and individuals with PCOS. 17 Next, due to the established relationship between inflammation and PCOS, anti-inflammatory treatment options are necessary. 6 Specialized pro-resolving lipid mediators (SPMs) are lipid mediator molecules derived from essential ω3-poly-unsaturated fatty acids (PUFAs), docosahexaenoic acid (DHA), and eicosapentaenoic acid (EPA), and SPMs have been investigated as a possible intervention. 67 SPMs show profound anti-inflammatory activity by decreasing proinflammatory cytokines IL-6, TNF-α, and IFN-γ, increasing anti-inflammatory cytokine IL-10, counteracting adipokine secretion and monocyte accumulation, promoting M2 macrophage polarization, and increasing insulin sensitivity. 67
In the realm of inflammation-focused PCOS treatment is the manipulation of the kynurenine pathway (KP), the metabolic pathway of tryptophan that creates serotonin and metabolites involved in mood disorders, neurodegenerative diseases, and chronic pain conditions, including PCOS. 18 PCOS and KP have been linked to a poor gut microbiome with low diversity and composition with high intestinal concentrations of Bacteroidetes. 18 In an animal study, where the animals were manipulated to develop the PCOS phenotype, continuous administration of an antibiotic cocktail reduced the bacterial load of Bacteroidetes, which coincided with reduced IR and PCOS phenotype. 18 This, in turn, reduced the rate of degradation and availability of tryptophan for the KP. 18 Furthermore, progesterone has been found to inhibit the proinflammatory indoleamine 2,3-dioxygenase (IDO-1) pathway of the KP, indicating another role for OCPs in PCOS pain management. Therefore, the KP provides another prospective treatment angle for PCOS pain management. 18
Translating evidence into action
Although significant advances in PCOS management and treatment approaches have been reported, the length of time from evidence creation to implementation of evidence-based practices remains lengthy and inconsistent. 68 This could be attributed to the existing research-to-practice gap, where it is estimated that 85% of research efforts were lost over the past decade due to the absence of effective and longitudinal evidence-based translation practice. 69 Translating research evidence to clinical practice ensures the safe, transparent, and efficient delivery of healthcare services to patients, families, and society. 69 However, over 40% of adult patients have been receiving care that is not based on current evidence guidelines, leading to a lack of benefit to end-users of advances in healthcare, elevated risk of iatrogenic harm, and enhanced opportunity costs to the health system of continued delivery of obsolete, ineffective, or harmful care. 70 There is a need for translational frameworks, informed by implementation science, to guide methodological rigor, improve stakeholder engagement and partnership, and strengthen timely translational efforts. 71 One of these frameworks that has been applied to translate the 2018 International PCOS guidelines is the Monash Centre for Health Research and Implementation Framework. 58 The application of this framework contributed to a list of outputs (listed in Table 2) from the 2018 International PCOS Guideline translation program following the implementation of an evidence-informed research translation process.
Despite the presence of such guiding evidence-based frameworks, the prevalence, complexity, and burden of this syndrome continues to be underappreciated and underfunded for innovative research approaches compared to fewer common conditions. 72 Fortunately, robust research recommendations are being developed in 2023 with the input of clinicians, academics, and consumers to update the 2018 International PCOS guideline. 73 These specific recommendations will be tailored to the need for greater research efforts for this neglected condition and will include correspondence to major funding bodies that have been endorsed by partner societies globally. 74 Table 3 lists the aims and principles of the 2023 update for the International PCOS guideline.
Limitations
Findings from this scoping review should be interpreted in the context of study limitations. First, although our search only identified a total of two articles and two abstracts that satisfied our inclusion and exclusion criteria, several findings have been highlighted that could inform future patient-centered chronic pain treatment approaches for patients with PCOS. Second, due to the limited research available on the topic of chronic pain and PCOS and the exploratory nature of this review, an inadvertent omission of search terms specific to pain symptoms in PCOS patients might have happened. However, the guidance provided by the senior librarian in the development of the search strategy helped in mitigating the impact of this concern. Third, the scope of the current review was limited. Formal assessment of the quality of the included studies was not carried out. However, important findings from our review on the necessity to bridge the gap in treatment between chronic pain and PCOS can act as a guide for the write-up of comprehensive protocols for randomized clinical trials to build evidence on the reported associations between chronic pain symptoms and the disease.
Conclusion
The purpose of this scoping review is to explore current research on the association between chronic pain and PCOS to create local and global recommendations to improve access to affordable symptom management and treatment options for patients with PCOS. The advent of various methods to manage chronic pain in PCOS provides hope for patients. More research studies are necessary to examine existing associations between the disease and pathophysiological symptoms for a better QoL for the population dealing with PCOS.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241262158 – Supplemental material for Polycystic ovary syndrome and chronic pain among females and individuals of childbearing age: A scoping review
Supplemental material, sj-docx-1-smo-10.1177_20503121241262158 for Polycystic ovary syndrome and chronic pain among females and individuals of childbearing age: A scoping review by Lea Sacca, Goodness Okwaraji, Sebastian Densley, Adeife Marciniak, Michelle Knecht, Candy Wilson, Julie G Pilitsis and Dawn Kimberly Hopkins in SAGE Open Medicine
Supplemental Material
sj-pdf-2-smo-10.1177_20503121241262158 – Supplemental material for Polycystic ovary syndrome and chronic pain among females and individuals of childbearing age: A scoping review
Supplemental material, sj-pdf-2-smo-10.1177_20503121241262158 for Polycystic ovary syndrome and chronic pain among females and individuals of childbearing age: A scoping review by Lea Sacca, Goodness Okwaraji, Sebastian Densley, Adeife Marciniak, Michelle Knecht, Candy Wilson, Julie G Pilitsis and Dawn Kimberly Hopkins in SAGE Open Medicine
Footnotes
Author contributions
LS, GO, SD, and AM had substantial contributions to the conception and design of the work, interpretation of data, drafting of the work, and final approval of the work for publication. MK had substantial contribution to data analysis, drafting of the work, and providing final approval for publication. CW, JGP, and DKH provided critical feedback on important intellectual content and reviewed the final version for approval on publication. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article (and/or) its supplemental materials.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
The Florida Atlantic University Institutional Review Board considered this review paper as exempt research.
Informed consent
Not applicable since this study is a review and does not involve human participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.