
Abstract
Objectives:
Assessed the level of awareness of hepatitis B virus infection and hepatitis B immunoglobulin, and determined the proportion of pregnant women that will accept hepatitis B immunoglobulin if needed for their babies and the factors that were associated with the choices made by pregnant women in the Enugu metropolis.
Methods:
A cross-sectional study of 379 pregnant women in health facilities in the Enugu metropolis was undertaken between March and November 2019. A structured pre-tested interviewer-administered questionnaire was used for data collection. Data collected were analysed using SPSS version 23.
Results:
The overall knowledge of the respondents on hepatitis B virus infection was poor as only 26.6% had good knowledge. Only 25.6% of the respondents had heard of hepatitis B immunoglobulin but the majority of the respondents (93.1%) were both willing to accept to give the vaccine to their babies and recommend the vaccine to their relatives. The educational level and occupation of the respondents were significantly associated with overall knowledge of hepatitis B. Only the religion of the respondents correctly predicted the overall knowledge of the respondents on hepatitis B.
Conclusion:
Despite the poor knowledge of hepatitis B and hepatitis B immunoglobulin among the study participants, the acceptability of hepatitis B immunoglobulin was high.
Introduction
Hepatitis B virus (HBV) infection is an inflammatory condition of the liver. It is caused by the hepatitis B virus and runs a chronic course in humans. It is a major cause of morbidity and mortality both in males and females. Globally, about 2 billion people are infected, with more than 257 million persons becoming chronic carriers and 1–2 million people dying from this disease yearly as a result of severe morbidity/complications associated with the disease. 1 The prevalence of hepatitis B virus infection is highest among African countries with the prevalence highest in rural areas. 2 Africa harbours about 81 million chronic carriers and the mortality rate of this disease is as high as 25% in this region. 3 Prevalence rates ranging from 8% to 11% were recorded among pregnant women in Nigeria.4,5 The pooled prevalence of hepatitis B infection in Nigeria is 9.5% with the majority of the infections in rural communities (10.7%) with the North Western geo-political region with the highest rates of infection (12.1%). 6 In Enugu, the prevalence rate ranged from 1.0% to 12.4% among pregnant women and children.7–11
Africa harbours about 81 million people with chronic hepatitis B infection with a prevalence rate of 6.2% and most of these infections are gotten during pregnancy and childbirth. Previous global high rates of infection have reduced from 5% to less than 1% due to several interventions by the World Health Organization (WHO). 12 Despite the Expanded Program on Immunization (EPI) and several interventions to prevent maternal transmission of HBV to babies, the prevalence of the disease is still high in sub-Saharan Africa (>8%). Nigeria is one of the hyperendemic countries for hepatitis B virus infection in Africa (>8% prevalence rate) with about 9 out of 10 people unaware of their infection status. 13 The active transmission of hepatitis B virus in Nigeria is high with a pooled mother-to-child transmission rate for hepatitis B virus infection in Nigeria put at 55.49% (35.93%–75.04%). 14 The National Program on Immunization (NPI) is a major intervention for the elimination of hepatitis B virus infection in Nigeria but currently is faced with the problem of poor uptake. The uptake of the birth-dose of HBV vaccination is 53% leaving many babies unvaccinated at their first chance at prevention of perinatal transmission of hepatitis B virus at birth. 15 Worse still, there are no specific HBV vaccination programmes for at-risk populations such as Men Who Have Sex With Men, healthcare workers, People Who Inject Drugs, Incarcerated Populations etc., who constantly maintain increased transmission of the virus in the population. The rate of complete vaccination (at least three doses) against hepatitis B virus ranged from 36.2% to 59.5% in Nigeria, with the highest rate among doctors.16–18 This leaves Nigeria as a huge ground for the transmission of the virus and this may explain why Nigeria recorded some increase in the prevalence of hepatitis B virus infection in the last decade while other African countries had a decrease. 19
The age of infection with hepatitis B virus largely determines whether an individual will develop chronic hepatitis. This means that infection acquired during infancy/childhood will lead to higher chronic HBV infection, more morbidities, and mortalities than those acquired at the adult stage of life. 20 Therefore, infection acquired during childhood has the highest proportion of the burden of the infection associated with HBV.20,21 HBV infection may lead to an asymptomatic infection where the patient does not present with symptoms; it may also result in acute infection that may become self-limiting or become fulminant hepatitis which management involves liver transplantation. HBV infection may also progress to become a chronic infection that may subsequently lead to liver cirrhosis or hepatocellular carcinoma. 22
Hepatitis B virus is regarded as one the most highly infectious agents, about 50–100 times more infectious than the Human immunodeficiency virus (HIV), and constitutes major public health importance globally. 23 The virus is very contagious and can easily be transmitted from a pregnant mother to her baby during pregnancy, delivery, and post-delivery mainly during breastfeeding and through other contacts that result in the exchange of blood/serum primarily.24,25 Perinatal transmission from mother to her baby is a very important mode of transmission because, in the presence of a serologic marker for active hepatitis B virus replication, hepatitis B e antigen (HBeAg), the rate of chronic infection in the baby in the absence of immunoprophylaxis with hepatitis B immunoglobulin and hepatitis B vaccination at birth is 70%–90% 6 months after birth.25,26
The hepatitis B vaccine and hepatitis B immunoglobulin are both given as post-exposure prophylaxis to babies of infected mothers with the first dose given 12–24 h after birth in addition to the completion of the three-dose series of hepatitis B vaccine. This has been shown to give 90%–100% protection against acute and chronic HBV infection to infants of mothers who are positive for both HBsAg and HBeAg in pregnancy even with the first dose of these vaccines.21,27 Hepatitis B immunoglobulin (HBIG) is a substance that is prepared from human blood, and its administration increases the level of antibodies against HBV in the body. It can be given to the newborn and even pregnant mothers as part of immunoprophylaxis towards the prevention of infection in the newborn. 28
Despite the available information on hepatitis B and its prevention in neonates, the awareness of hepatitis B and the risk factors for its transmission among people is poor among pregnant mothers.29–31 Equally, increased awareness of hepatitis B immunoglobulin may increase the uptake of the vaccine which in turn may reduce the incidence of the disease among newborn babies. It has been established that our pregnant mothers have a poor understanding of the relationship between increased uptake of hepatitis B immunoglobulin and reduced prevalence of babies with chronic hepatitis B in their childhood. 32
There were few works in Nigeria on the acceptability of hepatitis B immunoglobulin by pregnant mothers.31,33,34 The objectives of this study were to assess the level of awareness of hepatitis B virus infection and hepatitis B immunoglobulin among pregnant women in the Enugu metropolis. Also, to determine the proportion of pregnant women that will accept hepatitis B immunoglobulin if needed for their babies and the factors that were associated with their choices. The baseline information evidence obtained at the end of this research may be utilized by the government, non-governmental organizations etc., in the review of existing policies and/or formulation of new ones that will help reduce the number of babies that live with chronic hepatitis B in the childhood and adult stages of their lives. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were strictly adhered to in the reporting of this research findings. 35
Methods
Study design and setting
This study was a cross-sectional study that involved pregnant women in tertiary, secondary, and primary health facilities (public and private faith-based) in the Enugu metropolis conducted between March and November 2019. Enugu metropolis is the capital of Enugu State. It has three local governments (Enugu South, Enugu North, and Enugu East). The Enugu metropolis has a total population of 722,664 (male = 348,902 and female = 468,223) according to the last Nigeria census figures of 2006. Enugu State also called “The Coal City State” is located in the Southeastern part of Nigeria. It was created out of the old Anambra State in 1991 by the then-military government of General Ibrahim Badamasi Babangida. The capital city is Enugu, “The Coal City.”
The selected healthcare facilities were a tertiary (Enugu State University of Science and Technology Teaching Hospital (ESUTTH), Parklane), a secondary (Mother of Christ) and three primary (Poly Clinic, Uwani Health Centre and Primary Health Centre, Abakpa Nike, Enugu) health facilities all in Enugu metropolis. Available data from the Department of Health Planning, Research and Statistics (DHPRS) of the Ministry of Health Enugu revealed that there are two public tertiary hospitals, one district hospital, five missionary hospitals/Faith-based maternity hospitals, forty primary healthcare centres, 13 maternity homes and 22 private hospitals distributed in all the 3 local governments of Enugu metropolis. Most of the pregnant mothers are seen in these listed hospitals. The selected healthcare facilities were purposively selected from the list of all the maternity tertiary, secondary, and primary health facilities in the Enugu metropolis. The healthcare facilities were selected primarily because they conduct maternity services and their selection also reflected the distribution of pregnant women they manage in the Enugu metropolis. Consecutively consenting pregnant women were selected and interviewed from each hospital until the number of participants allotted to the hospital was reached.
Study population
The study population consisted of all the pregnant women in the Enugu metropolis from the selected study sites. All pregnant women in the selected hospitals who gave their consent for this research were recruited for this study while all pregnant women who were not in the selected hospitals or who did not give their consent for this study were excluded from this study. Also, pregnant mothers who were so ill that their mental capacity could not easily understand the questions in the questionnaire were equally excluded from this study.
Sample size estimation and sampling
The minimum sample size (n) was estimated by using the formula 36 : n = Z2 pq/E2. Where Z = coefficient of Z statistics obtained from the standard normal distribution table, p = prevalence rate (in percent), q = 100–p, E = sample error tolerated (in percent), using an awareness rate (p) of 71.5% for hepatitis B virus infection in pregnancy for a study carried out in Abakiliki, 34 at a confidence limit of 95%, and sampling error of 5%. Therefore, the calculated sample size (n) was 330. Assuming a non-response rate of 10%, 33 the minimum sample size was 363 pregnant women.
A multi-stage sampling technique was utilized in the selection of the participants in the study. Firstly, a purposive sampling technique was used to select healthcare facilities used for this research. The selection was done to reflect the distribution of pregnant women in the Enugu metropolis. The number of participants was proportionately distributed depending on the number of pregnant mothers seen in the selected health facilities. An allocation of 35% of the questionnaires was given to clients in the tertiary maternity institution, 20% in secondary healthcare facility, and the remaining 45% in the three selected primary healthcare centres. This purposive sampling technique was chosen to make sure it was only busy maternity hospitals where the majority of antenatal women in the Enugu metropolis go for maternity services were chosen for this research.
Secondly, a systematic sampling technique was utilized by choosing consenting participants after determining the number present in each antenatal clinic and developing a sampling frame. The sampling frame was generated from the number tally given to the pregnant women before they started seeing their doctors and other health personnel. Where such was not possible, every other consenting participant was selected from a particular health facility until the number allotted for such facility was reached. No participant was sampled more than once.
Data collection tool and technique
A structured interviewer-administered questionnaire was used to collect data from the participants utilizing the exit interview approach. The participants were assisted by the research assistants to complete the questionnaires. The questionnaires had three sections and each section was targeted at addressing each of the research questions. They were designed based on the objectives of the research. The validity (content, face, criterion, construct) and reliability of the questionnaire were enhanced by applying robust measures. The questionnaires were given to selected clients to correct noted gaps in the questionnaire and identified gaps were corrected. We conducted a pretesting of the questionnaires on 10% of the sample participants chosen from all the study sites and also, we had the questionnaires reviewed severally by experts in obstetrics, medicine, statistics, and health economics, management, and policy. All necessary corrections were made on the questionnaires after the pretesting and reviews before they were used for data collection.
The first section contained questions on the socio-demographic characteristics of the participants. This section contained questions trying to ascertain the basic demography of the participants like the age, educational level, employment status or occupation of the participants and the husband’s marital status, etc. The second section contained questions that tested the awareness of participants on hepatitis B and hepatitis B immunoglobulin. Questions on how well the participants knew hepatitis B and hepatitis B immunoglobulin were asked there. The third section of the questionnaire contained questions to determine the acceptability of hepatitis B immunoglobulin by the participants. This was ascertained by questions on whether they can use or recommend the hepatitis B immunoglobulin for their friends if the need arises.
The members of the research team were well-trained by the research team on the method of data collection technique before the commencement of the research.
Data collection was commenced from the hospitals selected for this study after approval by the Ethics Committee of the Enugu State University of Science and Technology Teaching Hospital, Parklane, Enugu. Following individual counselling, well-structured interviewer-administered questionnaires were given to selected consenting pregnant mothers for response and completion. The exit interviewer-administered approach was adopted. The questionnaires were given to the participants after they had finished seeing their doctors for that day.
Data processing and analysis
The overall knowledge of the participants on a subject matter was calculated by scoring the total percentage of the correct answers to all the knowledge questions on a particular subject. The participant was said to have good knowledge if the participant got ⩾50% of questions correctly while poor knowledge was given to those who scored correctly <50% of the questions. The data collected were entered and analysed with Statistical Package for Social Sciences (SPSS) version 23. Data were presented using tables, graphs, charts, etc., as appropriate. Univariate statistics were used to analyse quantitative and qualitative variables. Means and standard deviations were reported for numeric (quantitative) variables while frequencies, percentages, and proportions were used to report categorical variables. Bivariate statistical analysis was performed to determine the factors that were significantly associated with good knowledge of hepatitis B and hepatitis B immunoglobulin. The Chi-square test was used to establish an association of independent variables like socioeconomic characteristics with overall knowledge, and willingness to take hepatitis B for free. Multivariate analysis using Binary logistic regression was used to determine predictors of good knowledge and willingness to take hepatitis B immunoglobulin for free (acceptability). Fisher’s exact test was applied where Chi-square was not appropriate such as where <20% of the cells have expected counts of less than 5. 37 Only variables with a Chi-Square p-value of at least 0.25 in the bivariate analysis were used in the multivariate analysis. Statistical significance was set at a p-value of less than 0.05. Each respondent’s socioeconomic status was determined using the “International Wealth Index Scale.” 38
Exchange rate for calculation of costs
All calculations of costs were based on the exchange rate of ₦370 for US$1 which was the average exchange rate of the local currency in Nigeria for a United States American Dollar within time (between March and November 2019) the study was conducted.
Ethical consideration
The ethical clearance certificate for this research was obtained primarily from the research and Ethics Committee of the Enugu State University of Science and Technology Teaching Hospital, Parklane, Enugu with certificate number ESUTHP/C-MAC/RA/034/VOL.11/70. Also, a clearance certificate was obtained from the Enugu State Ministry of Health with certificate number MH/MSD/REC18/042 to cover other hospitals used for this study. A written informed consent was read and signed by each participant in the presence of the interviewer and a witness. Women below 18 years (minors) had their consent forms signed and granted by their legally authorized representatives/relatives.
Outcome measures: The primary outcome measure was the level of awareness of hepatitis B and hepatitis B immunoglobulin. The secondary outcome measures were the level of acceptability of hepatitis B immunoglobulin and predictors of good knowledge of HBV and hepatitis B immunoglobulin.
Results
Socio-demographic characteristics of participants
A total of 379 participants were interviewed and all the questionnaires (100%) were filled out and used for analysis. The mean age of the respondents was 28.84 ± 4.74 years and the majority were in the 25–34 years age range (271, 71.5%). The majority of the respondents had tertiary education (244, 64.4%), were married (377, 99.5%) and were Christians (365, 96.3%). About half (208, 54.9%) of the respondents were employed. The details of the socio-demographic characteristics of the respondents are shown in Table 1
Socio-demographic characteristics of the participants.

Participant’s knowledge of hepatitis B virus infection
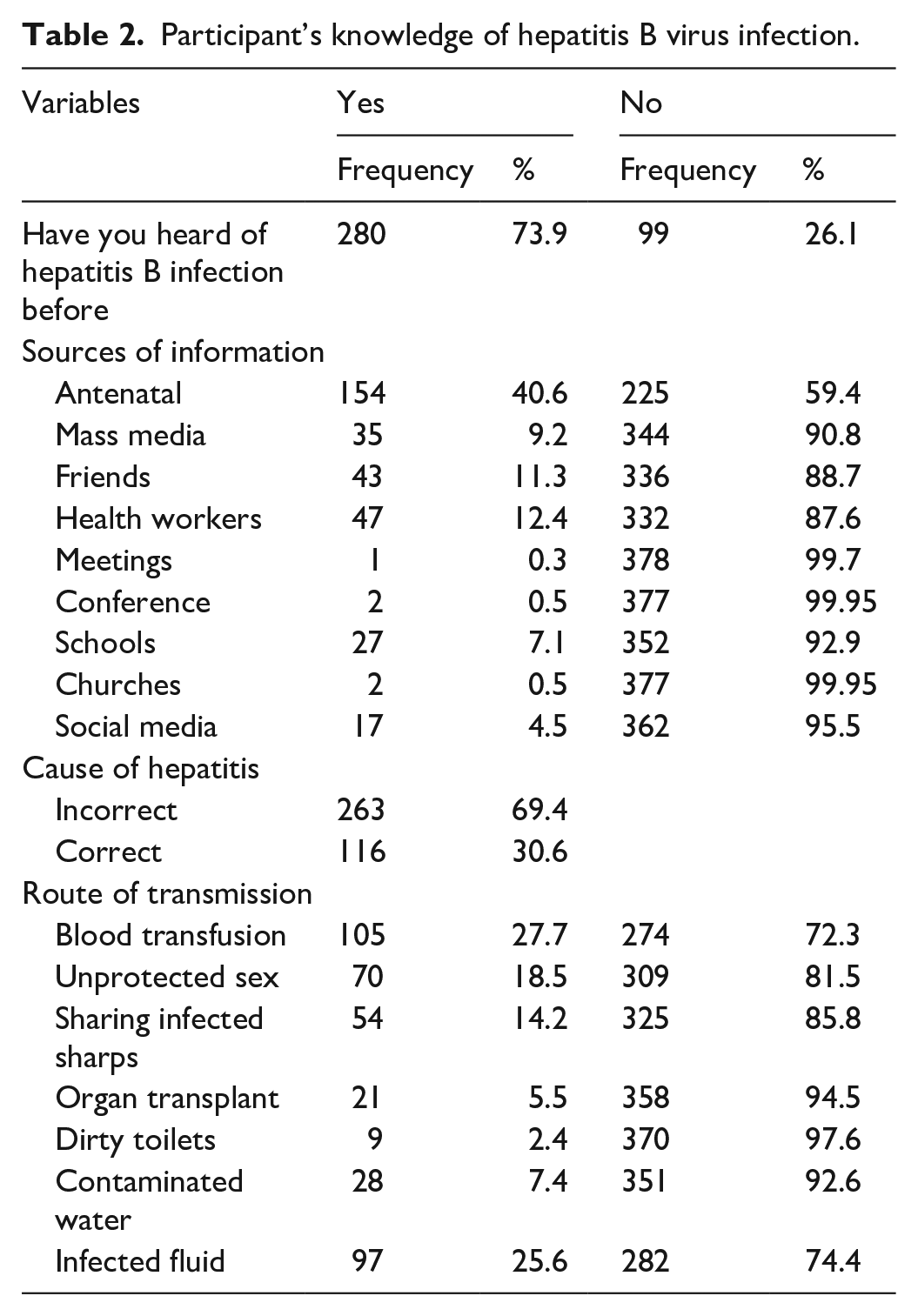
The majority of the respondents (280, 73.9%) have heard of hepatitis B and most (154, 40.6%) of them got the information from the antenatal clinics, friends (43, 11.3%) and health workers (47, 12.4%). The majority of the participants (263, 69.3%) do not know the cause of hepatitis B virus infection. The participants identified that blood transfusion (105, 27.7%), unprotected sex (70, 18.5%), sharing of infected sharps (54, 14.2%), and infected body fluids (97, 27.6%) among others are major routes of transmission of hepatitis B virus infection. The other details of the respondent’s knowledge of hepatitis B virus infection are shown in Table 2
Participant’s knowledge of hepatitis B virus infection.
Participant’s overall knowledge of hepatitis B virus infection
The overall knowledge of the respondents on hepatitis B virus infection was poor as only 26.6% (101) of the respondents had good knowledge of the hepatitis B virus infection. The knowledge of the respondents on routes of transmission, treatment options and prevention was generally poor among the respondents. However, it is important to note that up to 72% (273) of the respondents knew that HBV infection could be prevented. The details of the participant’s overall knowledge of hepatitis B virus infection are shown in Table 3
Participant’s overall knowledge of hepatitis B continued.

Participant’s knowledge of hepatitis B immunoglobulin
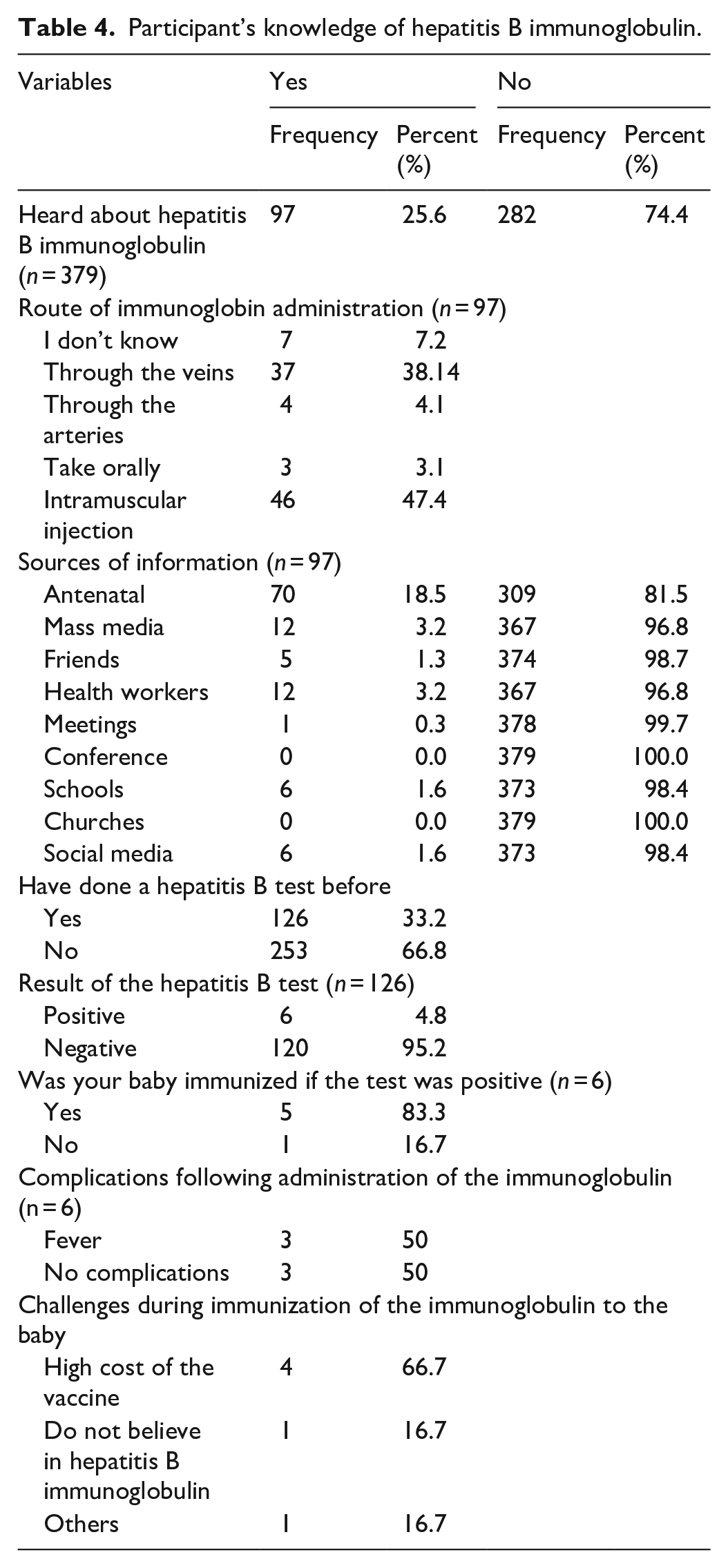
Only 25.6% (97) of the respondents have heard of hepatitis B immunoglobulin and most got the information from antenatal care (ANC) clinics (70, 18.5%), mass media (12, 3.2%) health workers (12, 3.2%) etc. Only 33.2% (126) of the respondents knew that they had done hepatitis B virus screening tests in the past and out of this group, 4.8% of them tested positive for hepatitis B. Among the positive women, the majority (83.3%) of them gave hepatitis B immunoglobulin to their babies. The major challenge to the administration of hepatitis B Immunoglobulin was the high cost of the vaccine. Other details are in Table 4.
Participant’s knowledge of hepatitis B immunoglobulin.
Willingness to accept (acceptability) hepatitis B immunoglobulin
The majority of the respondents (93.1%) were willing to accept giving the vaccine to their babies. Also, the same proportion of people were willing to recommend the vaccine to their relatives and their close contacts as shown in Figure 1

The distribution of respondents that were willing to accept hepatitis B immunoglobulin for their babies and contacts.
Association of socio-demographic characteristics and overall knowledge of hepatitis B virus infection
The educational level (p < 001) and occupation (p < 001) of the respondents were significantly associated with the overall knowledge of hepatitis B virus infection among the respondents. Other details on the relationship between the overall knowledge of hepatitis B virus infection and other socio-demographic characteristics were documented in Table 5.
Association of socio-demographic characteristics and overall knowledge of hepatitis B.

Association of economic characteristics of the respondents with overall knowledge of hepatitis B virus infection
Most of the economic variables (wealth index, average income, household income, non-food expenditure) of the respondents are significantly associated with the overall knowledge of the respondents. The details of the relationship between the economic variables of the respondents and the overall knowledge of the participants are in Table 6.
Association of economic characteristics of the respondents and overall knowledge of hepatitis B.
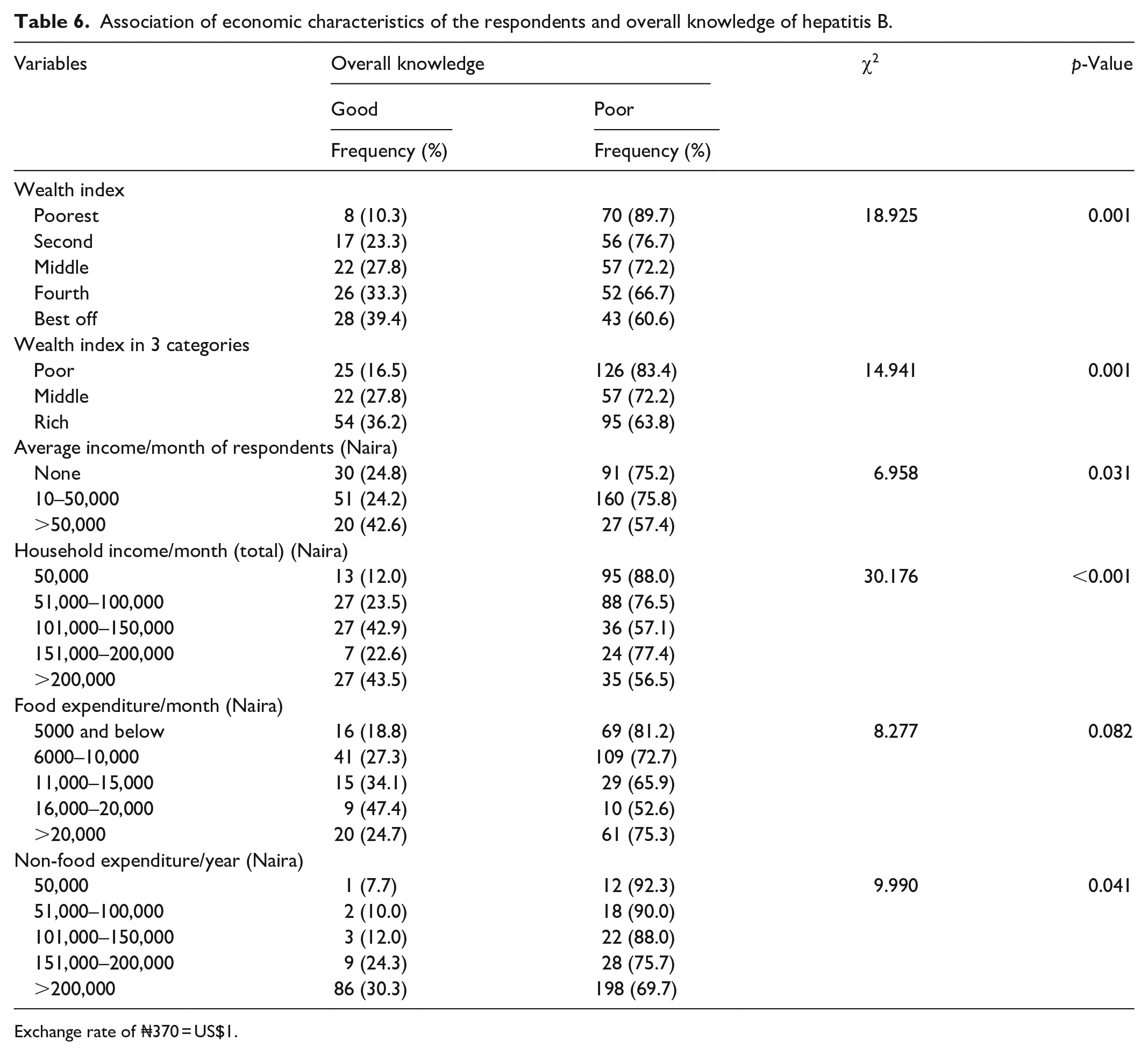
Exchange rate of ₦370 = US$1.
Association of participant’s socio-demographic characteristics with the acceptability of hepatitis B immunoglobulin
The acceptability of the vaccine by the respondents was not significantly associated with the respondent’s socio-demographic variables. The details are shown in Table 7.
Association of participant’s socio-demographic characteristics with the acceptability of hepatitis B immunoglobulin.

FT: fisher exact test.
Association of economic characteristics of respondents with the acceptability of hepatitis B immunoglobulin
It was only the non-food expenditure patterns of the respondents that were significantly associated with willingness to accept the vaccine. Details are in Table 8.
Association of economic characteristics of respondents and acceptability of hepatitis B immunoglobulin.
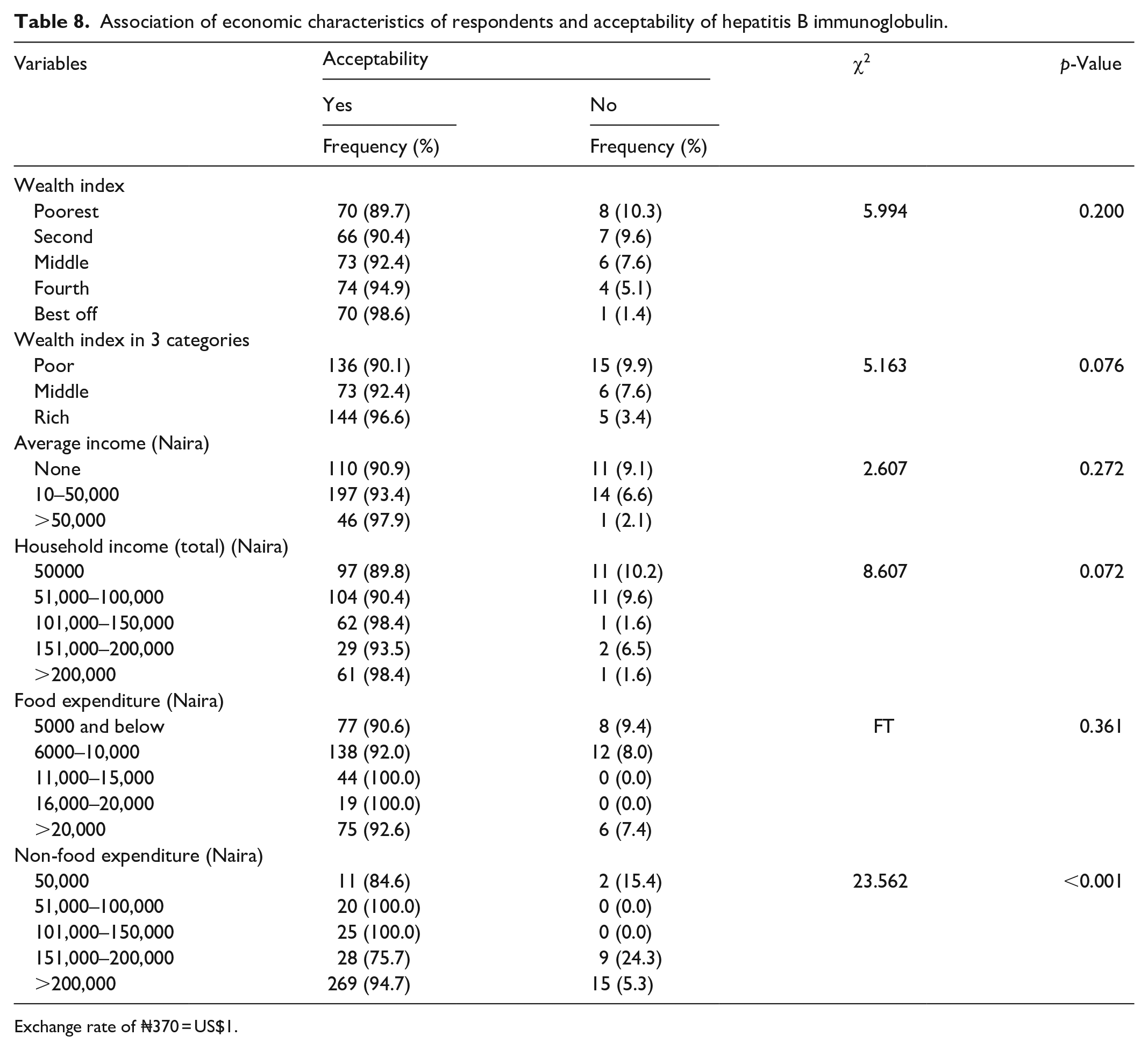
Exchange rate of ₦370 = US$1.
Association of participants’ husband’s characteristics and acceptability of hepatitis B immunoglobulin
Only the educational status of the respondent’s husbands was significantly associated with willingness to accept the hepatitis B immunoglobulin. Other details are as shown in Table 9.
Association of participants’ husband’s characteristics and acceptability of hepatitis B immunoglobulin.

Predictors of overall knowledge of hepatitis B virus infection of respondents
None of the respondent’s characteristics correctly predicted the overall knowledge of the respondents about hepatitis B virus infection excluding the religion of the respondents which showed that being a Christian was about nine times more likely to have good knowledge compared to those of other religions (p = 0.047, AOR = 9.629, 95% CI: 1.027–90.299), details are shown in Tables 10 and 11.
Predictors of overall knowledge of hepatitis B virus infection of respondents.

Economic predictors of participant’s overall knowledge of hepatitis B virus infection.
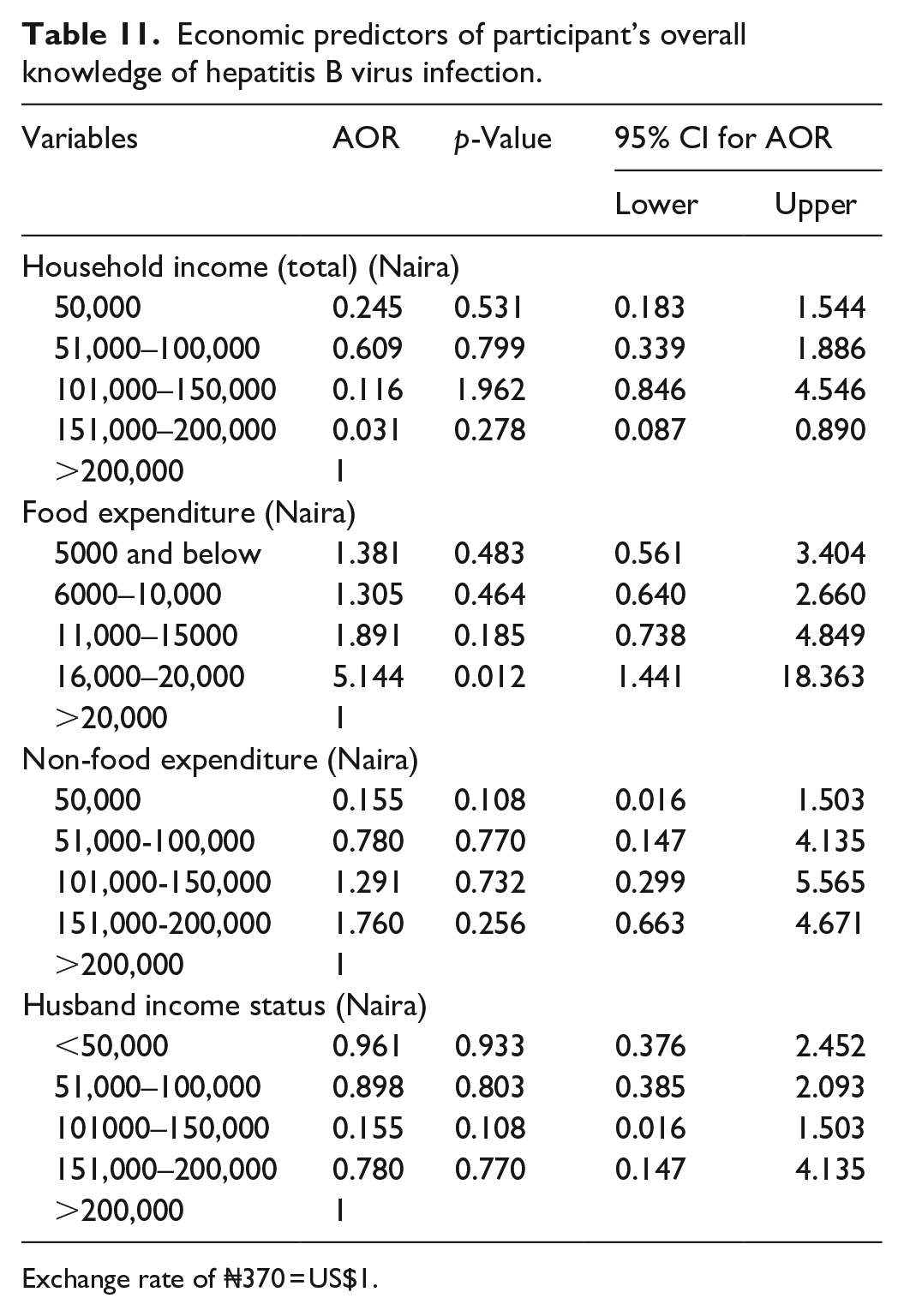
Exchange rate of ₦370 = US$1.
Predictors of acceptability of hepatitis B immunoglobulin by respondents
None of the socio-demographic variables and economic characteristics of the respondents and family correctly predicted the acceptability pattern for hepatitis B immunoglobulin.
Discussion/conclusion
This study was undertaken to assess the level of awareness of hepatitis B virus infection and hepatitis B immunoglobulin among pregnant women in the Enugu metropolis. It also determined the proportion of pregnant women who will accept hepatitis B immunoglobulin if needed for their babies (acceptability). The study also identified the predictors of the level of knowledge of hepatitis B virus infection among the participants. Findings showed that the overall knowledge of hepatitis B virus and hepatitis B immunoglobulin was poor, however, the acceptability for the hepatitis B immunoglobulin was high. The educational level and occupation of the respondents were significantly associated with overall knowledge of hepatitis B virus infection. Only the religion of the respondents correctly predicted the overall knowledge of the respondents on hepatitis B virus infection.
The overall knowledge of the participants with good knowledge of hepatitis B virus infection was low even though the majority of the participants had tertiary education. However, it is important to note that most of the participants were unemployed and were not healthcare workers and this may have affected their ability to know more about hepatitis B virus infection. Some of the participants despite their attending antenatal care have not heard of hepatitis B virus infection even though such tests may have been done for them during their antenatal care. This may go on to describe the quality of antenatal care received by these women as being sub-optimal. It is also possible that those antenatal attendees do not pay attention to the health education that is usually given to them during antenatal clinic sessions.
This general poor knowledge among the study participants is in keeping with that of other studies,39–41 which also showed low levels of knowledge and awareness of hepatitis B virus infection. Even a lower level of knowledge of hepatitis B virus infection was observed in a similar study in Mumbai, India involving women of childbearing age in three slums in Mumbai city. 42 Many of these studies were performed among women attending antenatal care (general population) therefore the findings reflected the true level of information on hepatitis B among the women in the population.
The overall knowledge was found to be significantly associated with the level of education and occupation of the study participants as was similarly observed by Abdulai et al. 40 in a similar study in Kintampo North Municipality of Ghana. Both education and occupation were observed as predictors of good knowledge in the study by Abdulai et al. 40 A similar finding was also observed in a related study by Frambo et al. 41 among rural pregnant women in the Buea Health District of Cameroon. Higher levels of education were also found to be a predictor for good knowledge and awareness as was noted in a cross-sectional study by Han et al. 43 in Guangdong Province, China.
Furthermore, other characteristics of the participants in this study that were associated with good knowledge of hepatitis B virus infection include the wealth index, average monthly income, total income, and non-food expenditures by the study participants. The participants’ husband’s educational level, occupation, and income status were all associated with good knowledge of hepatitis B virus infection.
Importantly, to further expose the poor level of knowledge among the respondents it was observed that unprotected sexual intercourse was not recognized as a major means of transmission of hepatitis B virus infection. The poor general knowledge of hepatitis B virus infection among the general population may have contributed to the findings of this study. Furthermore, only 18.5% of the participants knew that the virus can be transmitted through unprotected sexual intercourse. This finding was in contrast with a proportion of up to 65% that knew that HBV can be transmitted sexually in a Hong Kong, China study. 44 Likewise, as many as 37.5% of the respondents do not know that mothers can transfer this virus to their babies. Despite the teachings these mothers received during their antenatal care visits, these findings were rather surprising and exposed at the same time the deficiencies of the participant’s antenatal care delivery. On the other hand, a slightly higher value was obtained among antenatal women in a Guangdong Province, China study where only 20% of the antenatal women were unaware of mother-to-child transmission (MTCT) of hepatitis B virus. 43
In contrast to the generally poor knowledge of hepatitis B virus infection findings of this research, other studies32–34 recorded high levels of knowledge among participants. The study participants in these studies were mainly health workers who had the extra opportunity of having been taught and they equally treated patients who had hepatitis B virus infection. The hospital environment where these participants worked made it easier for them to gain more information on the hepatitis B virus. The high level of knowledge (62.5%) found by Gboeze et al. 34 in the Abakiliki study among antenatal women may have resulted from a few parameters that they used to constitute good knowledge of hepatitis B virus infection.
Furthermore, the trend of poor knowledge also affected the proportion of women who knew about hepatitis B immunoglobulin as only 25.6% of the respondents knew about the vaccine. This finding is related to the proportion of study participants who have good knowledge (26.6%) of hepatitis B virus infection. It, therefore, suggests that the proportion of the participants with good knowledge of HBV infection were those who were aware of the hepatitis B virus immunoglobulin.
After a thorough explanation of the hepatitis B immunoglobulin, a large proportion (93%) of the respondents accepted to use of this vaccine for their children if needed. The reason for this level of acceptance of the immunoglobulin was not associated with the socio-demographic characteristics of the respondents. It is suggested that the amount of health education (that explained and assured them of protection from this vaccine) given to the participants in the course of the interview may have contributed to this finding. This further suggests that mass education of pregnant women and other members of the population irrespective of their educational levels and occupation on a health product may increase the acceptance of that product as observed in this study.
Strengths and limitations of the study
One of the strengths of this study was that the study drew participants proportionally from all levels of healthcare in the study area using a robust multi-stage sampling technique. Also, the questionnaires were administered to the participants by trained interviewers, and this helped to eliminate wrong responses from the participants. Additionally, the trained research assistants equally helped to educate those who were not aware of the topic to the extent that appropriate information was elicited from them that their real willingness to accept the vaccine was determined. Our study can serve as a baseline in this field of study as there are no previous studies in the study area that addressed this topic from our point of view.
Limitations of this study include the use of purposive sampling technique (in our bid to get at the majority of the participants in the different health facilities in the Enugu metropolis) in choosing the health facilities that participated in the research which may have unjustly excluded some women in participating in the research. Also, recall bias among the participants may have limited the amount and quality of data obtained although trained assistants were utilized to ensure correct data were collected from the participants.
Conclusions and recommendations
The level of knowledge of hepatitis B virus and hepatitis B immunoglobulin among pregnant women in the Enugu metropolis was poor and despite that the acceptability of hepatitis B immunoglobulin was high. Given the generally poor knowledge of hepatitis B virus infection and immunoglobulin despite the high level of education of most of the respondents and daily antenatal health talks received by the mothers, there is a need to reorganize the content of antenatal health education given to pregnant mothers during every antenatal visit to give more attention to the perinatal transmission of common diseases like hepatitis B virus infection. There is also a need to retrain healthcare workers on the method and content of their daily antenatal health talks/education to be delivered in such a way as to increase the understanding of pregnant mothers. The government should also intensify public enlightenment on hepatitis B and its preventive measures. Media campaigns on the long-term consequences of hepatitis B infection should be well explained to the public just like was done for HIV/AIDS.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241257083 – Supplemental material for Assessing the awareness and acceptability of hepatitis B immunoglobulin among pregnant women in Enugu metropolis, Southeast, Nigeria: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241257083 for Assessing the awareness and acceptability of hepatitis B immunoglobulin among pregnant women in Enugu metropolis, Southeast, Nigeria: A cross-sectional study by Enebe Joseph Tochukwu, Enebe Nympha Onyinye and Onwujekwe Emmanuel Obinna in SAGE Open Medicine
Footnotes
Acknowledgements
I appreciate contributions from the lecturers in the department of Health Administration and Management, UNEC, Enugu: Dr OG Ochonma, Dr Charles Ezenduka, Prof BSC Uzochukwu and Prof IJ Okoronkwo for their continued support and assistance to the team with intelligent contributions and materials for this study. I also appreciate all the research assistants especially, Ozoeze Amarachi for their steadfastness and dedication towards gathering the needed data for the conclusions reached in this study.
Availability of data and materials
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The ethical clearance certificate for this research was obtained primarily from the research and Ethics Committee of the Enugu State University of Science and Technology Teaching Hospital, Parklane, Enugu with certificate number ESUTHP/C-MAC/RA/034/VOL.11/70. Also, the clearance certificate was obtained from the Ministry of Health with certificate number MH/MSD/REC18/042 to cover other hospitals used for this study.
Informed consent
A written informed consent was read and signed by each participant in the presence of the interviewer and a witness. Women below 18 years (minors) had their consent forms signed and granted by their legally authorized representatives/relatives.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.