
Abstract
Objectives:
Recently, there has been a decline in the use of vacuums and forceps. This is due to complications that occur in the mother and baby as well as the operator’s ability to operate the instruments. Concerning Professional Education Standards for Obstetrics and Gynecology Specialists, the minimum skill that must be achieved by vacuum extraction and forceps is a minimum of five cases. This is difficult to achieve with the number of obstetrics and gynecology residents in West Java.
Methods:
A retrospective study was conducted using medical records based on the International Classification of Disease 10th Revision from 1 to 28 February 2023 at teaching hospitals and Academic Health System in West Java, namely Hasan Sadikin Hospital, Al-Ihsan Hospital Bandung, and Cikalong Wetan Hospital West Bandung, in the period 1 January 2018 to 31 December 2022. The main outcome was vacuum and forceps extraction with consecutive sampling. The relationship between maternal characteristics such as maternal age, parity, gestational age, and indication for delivery with vaginal operative delivery was descriptive statistics analyzed using IBM SPSS Statistics 26.
Results:
Trends indicate that the percentage of vaginal operative deliveries tends to be low, below 5%. Vacuum deliveries decreased from 0.75% in 2018 to 0.68% in 2022, while forceps deliveries decreased from 2.77% to 0.98% over the same period.
Conclusion:
This study concludes that there was an insufficiency of vacuum extraction and forceps delivery cases at the teaching hospital and Academic Health System in West Java to achieve a minimum case of vacuum and forceps. Further research studying how educational interventions improve operative delivery skills might be considered.
Introduction
Vaginal operative delivery involves the assisted delivery of forceps and vacuum extraction. These deliveries are carried out for indications of conditions related to the mother or fetus, and their use in obstetric practice in cases of fetal distress or prolonged second stage is common. Complications due to instrumental delivery can include vaginal and perineal lacerations and other complications such as bladder injuries and pelvic muscle injuries. 1 In 1999, Johanson et al. 2 published the first comparison of long-term outcomes of forceps versus vacuum delivery. Johanson et al. 2 conducted a 5-year follow-up on women who were part of the original randomized control trial sample. Three women reported symptoms of fecal incontinence. It was previously known that anal incontinence is a common occurrence in cases of obstetric trauma. Sultan et al 3 studied 43 women who delivered with instruments (26 forceps and 17 vacuum), endosonography, and neurophysiological tests. It is known that 80% of deliveries with forceps and 24% of deliveries with vacuum experience anal sphincter defects. Symptoms of difficult defecation were reported to occur in 38% of women who underwent forceps delivery and 12% of women who underwent vacuum delivery. The long-term effects of vacuum and forceps on neonatal and pediatric outcomes are still being studied. Current research still concentrates on the initial assessment of newborns. There was an increased risk of cephalhematoma (OR 2.7, 95% CI: 1.71–4.25) and retinal hemorrhage (OR 1.90, 95% CI: 1.70–2.00) in the vacuum extraction group. This is also directly proportional to the trend of low APGAR scores in the vacuum extraction group. There was 1 in 10 RCTs that examined the long-term outcomes of babies, namely 232 babies followed up for 1 year, strabismus was found in 8/115 babies born with vacuum extraction and 6/117 babies born with forceps. Hearing problems were not found in babies born with vacuum extraction, whereas there were three babies born with forceps. 2
This study shows that operative vaginal deliveries—both by forceps and vacuum—are decreasing every year. Trends in this analysis suggest that although the American Congress of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine support vaginal operative delivery as an alternative to cesarean delivery in certain clinical scenarios, the application of operative delivery is less common and accounts for the high rate of cesarean delivery.4,5 Women have the right to consider potential risks and benefits in making decisions regarding their mode of delivery. Obstetricians face increasing pressure from patients demanding elective cesarean delivery. 6 Current guidelines issued by the Royal College of Obstetricians and Gynecologists (RCOG) state that instrument selection is based on the operator’s ability to adapt to the clinical circumstances of the patient. 5 The most important factors in determining vaginal delivery are considerations of which interventions are necessary for delivery, the risks associated with the particular technique, and the skill level of the practitioner. 4 In terms of national competence, as reported by Perkonsil Number 86 of 2020 concerning Professional Education Standards for Obstetrics and Gynecology Specialists, the minimum skill that must be achieved by vacuum extraction and forceps is a minimum of five cases. 7 This is difficult to achieve with the number of obstetrics and gynecology residents in West Java totaling 90 students.
Considering that, this analysis aims to assess the adequacy of the Obstetrics and Gynecology Specialist Education Program student in achieving the minimum cases in performing vacuum and forceps extraction skills at teaching hospitals and the Academic Health System (AHS) in West Java. The study aims to incorporate its findings into the obstetrics and gynecology specialist education system. This integration is expected to enhance the proficiency of healthcare professionals in performing vacuum extraction and forceps procedures. By attaining this level of competency, it is anticipated that more patients will opt for vacuum extraction and forceps delivery methods, aligning with the guidelines set by RCOG. Ultimately, this shift in preference can help reduce the frequency of cesarean sections.
Methodology
Sample size and study population
This research is a retrospective study conducted at teaching hospitals and AHS in West Java, which includes Hasan Sadikin Hospital (RSHS), Al Ihsan Hospital Bandung, and Cikalong Wetan Hospital West Bandung, in the period 1 January 2018 to 31 December 2022. Data were collected using medical records from 1 to 28 February 2023. The inclusion criteria for this study were pregnant women who gave birth by forceps and vacuum extraction. Of the 29,102 data collected, 857 data were incomplete and were the exclusion criteria. We analyzed maternal characteristics such as maternal age, parity, gestational age, and indications of delivery. The main outcome of the study was vacuum and forceps extraction with consecutive sampling. There were 28,245 data entered, 747 were data with operative vaginal delivery and 27,498 data were deliveries other than operative vaginal delivery. The association of vaginal operative delivery was analyzed using the Statistical Product and Service Solutions computer application program (IBM Corp., Chicago, IL, USA). Multiple investigators were recruited to collect data, and to determine the consistency of measurements, inter-rater reliability was assessed. When dealing with missing data, our study uses data removal as a part of our exclusion criteria to help reduce the bias.
Variable
The study began by collecting data from medical records based on the International Classification of Disease 10th Revision (ICD-X). 8 First, grouping based on the type of delivery included vaginal operative delivery, cesarean section, and spontaneous delivery. In general, two types of instruments are widely used for operative vaginal delivery, namely forceps and vacuum. Forceps are classified depending on the need for rotation of the baby’s head or non-rotational forceps. Rotational forceps are used to rotate the baby’s head and provide axial traction while non-rotational forceps are used when only linear traction is required. Vacuum cups are also classified depending on the need to turn the fetal head or not. Cups are divided into anterior cups where rotation is not required or posterior cups where rotation to the occiput anterior position is required. Then combine these data and evaluate the proportion of deliveries using forceps and vacuum with all deliveries in 2018–2022 without any bias. Maternal characteristics such as maternal age, parity, gestational age, and indications of delivery associated with operative vaginal delivery were analyzed. Maternal characteristics including age (<20 years, 20–35 years, and >35 years), parity (1, 2–5, and >5), gestational age (<37 weeks, 37–40 weeks, and >40 weeks), and indications of delivery such as prolonged second stage of labor, an indication of time, preeclampsia, heart disease, and lung disease.
Ethics statement
The department issued a letter of ethical approval on 10th May 2023, with reference no. LB.02.01/X.6.5/156/2023 by the chairman of The Research Ethics Committee of Dr. Hasan Sadikin General Hospital Bandung, West Java, Indonesia.
Statistical analysis
Patient data were then tabulated on a personalized Microsoft® Excel v16.16.3 database (Microsoft®, Redmond, USA), and descriptive statistics were analyzed. The association of vaginal operative delivery was analyzed using the Statistical Product and Service Solutions computer application program (IBM Corp., Chicago, IL, USA). The numeric data were first checked for normal distribution using the Kolmogorov–Smirnov test, then presented as mean ± SD if normally distributed and as median (min–max) if not normally distributed. The unpaired t-test or Mann–Whitney test was used to identify significance among groups. A chi-square test was performed for bivariate analysis, followed by multivariate logistic regression. Bivariate analysis was done to identify candidate variables using p ⩽ 0.25. Multivariate logistic regression was used to control the effect of the confounder and a variable with p ⩽ 0.25 was included in multivariable logistic regression analysis. Finally, statistical significance was declared at p-value < 0.05.
Results
Trends indicate that the percentage of vaginal operative deliveries tends to be low, below 5%. A total of 28,245 deliveries from 2018 to 2022 were included in the analysis. There were 195 (0.69%) deliveries with vacuum extraction and 552 (1.95%) deliveries with forceps extraction at teaching hospitals and AHS in West Java. From data at RSHS, Al Ihsan Hospital, and Cikalong Wetan Hospital, there were only 638 (2.26%) vaginal operative delivery at Hasan Sadikin Hospital, 114 (0.40%) at Al Ihsan Hospital, 29 (0.10%) at Cikalong Wetan Hospital from 2018 to 2022 (Figures 1 and 2). The number of Padjadjaran University students is 90 people with the minimum number of cases that must be achieved for forceps and vacuum delivery is five cases each. While vacuum and forceps delivery rates decreased over the study period. Vacuum deliveries decreased from 0.75% in 2018 to 0.68% in 2022, while forceps deliveries decreased from 2.77% to 0.98% over the same period.

Comparison of deliveries in 2018–2022 in teaching hospitals and AHS in West Java.

Comparison of forceps and vacuum extraction in 2018–2022 in West Java teaching hospitals and AHS.
Maternal age <20 years had a risk of vacuum delivery 1.6 times greater than the age group 21–34 years (RR: 1.666; 95% CI: 1.023–2.715), and maternal age 35 years had a risk of vacuum delivery 2.25 times greater than the age group 21–34 years (RR: 2.257; 95% CI: 1.581–3.223). Meanwhile, parity 2–5 had a 2.78 times greater risk of vacuum delivery than the other parity groups (RR: 2.780; 95% CI: 2.162–3.573). Meanwhile, preterm and post-term gestational ages had a higher risk of undergoing vacuum delivery compared to the term group (RR: 7.532; 95% CI: 3.410–16.363; and RR: 0.312; 95% CI: 0.277–0.351). The prolonged second stage of labor and the indication of time had a greater risk of undergoing a vacuum than the other groups (p < 0.001).
In the forceps delivery group, it was concluded that the relative risk of patients aged 21–34 years to deliver with forceps was 0.9 times compared to patients aged <20 years (RR: 0.904; 95% CI: 0.733–1.115) and aged >35 years to deliver with forceps was 0.87 less than those aged 21–34 years (RR: 0.874; 95% CI: 0.762–1.003). Patients with 37–40 weeks’ gestation to deliver by forceps were 1.2 times compared to patients with <37 weeks’ gestation (RR: 1.200; 95% CI: 1.044–1.381). Preeclampsia was the indication for delivery by forceps 1.677 times compared to patients without preeclampsia (RR: 1.677; 95% CI: 1.434–1.962) and was the most common indication for forceps delivery (75.5%) and had a statistically significant relationship p < 0.001 (Tables 1 and 2).
Maternal characteristics in 2018–2022 at the West Java Teaching Hospital and AHS.
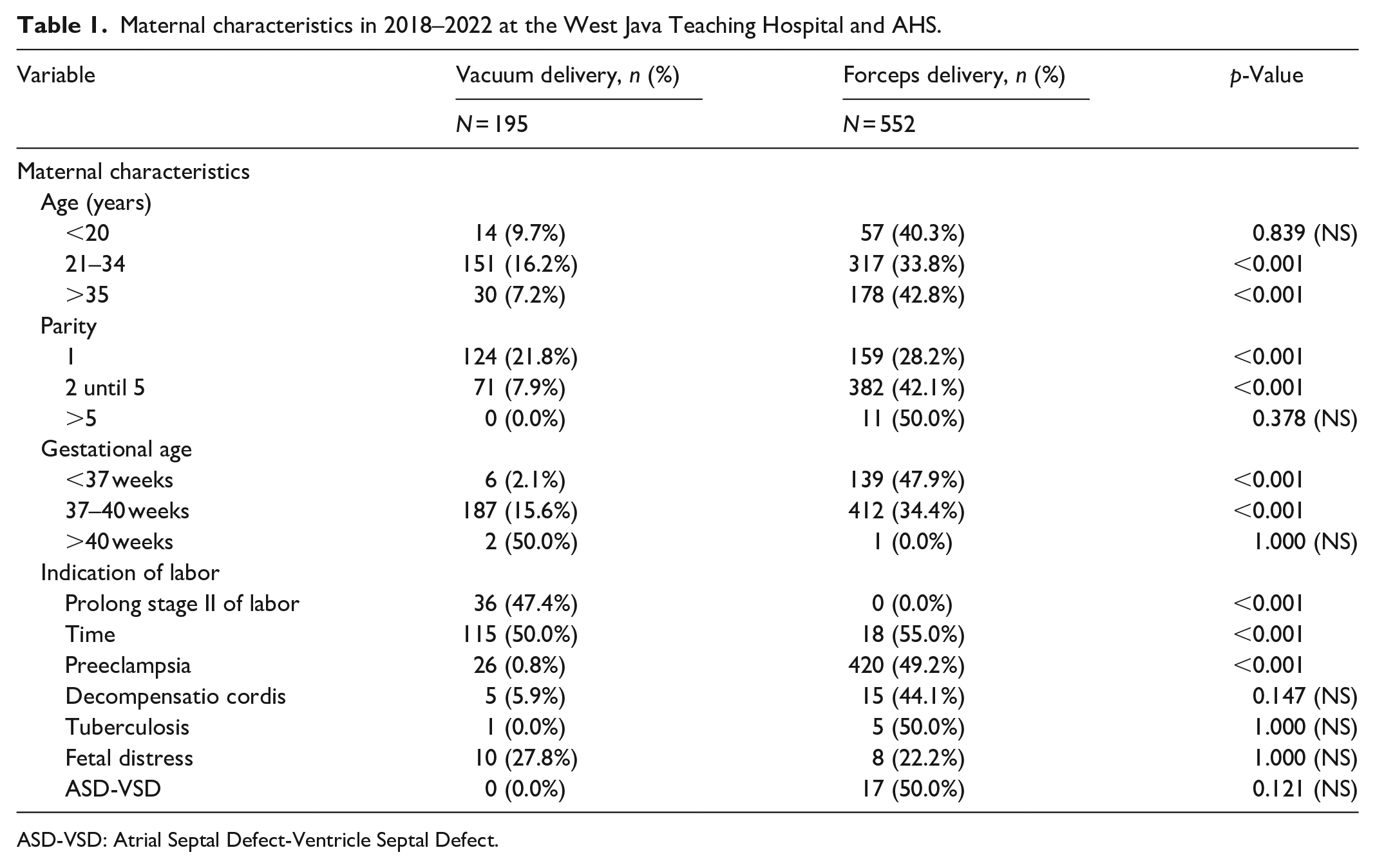
ASD-VSD: Atrial Septal Defect-Ventricle Septal Defect.
Analysis adjusted for factors associated with forceps and vacuum delivery in 2018–2022 at the West Java Teaching Hospital and AHS.

Discussion
There has been a decline in operative vaginal deliveries worldwide, with a more significant decline in forceps deliveries compared with vacuum deliveries. In the United States, the rate of operative vaginal deliveries has dropped to 3.1%, with forceps deliveries accounting for only a quarter of all assisted vaginal deliveries. 9 In the United Kingdom, the rates of operative vaginal deliveries have remained relatively stable, ranging from 10% to 15%, with a more balanced use of both instruments. 10 Several factors contribute to the decrease in operative vaginal deliveries, including concerns about medicolegal implications, declining competency due to reduced training opportunities, and safety and efficacy concerns from both patients and healthcare providers. This decline in operative vaginal deliveries has been accompanied by an increase in the rates of cesarean sections. 11 According to Jeon, 6 the rates of surgical vaginal deliveries are decreasing in private hospitals in particular in Korea. The data showed it is decreasing from 9.38% vaginal operative delivery cases in 1995 to 3.21% in 2014. The decrease in surgical vaginal delivery is due to a lack of experience with these techniques among medical residents, as hospitals and medical schools tend not to focus on training in surgical vaginal delivery. Meanwhile, according to Zhang et al., 11 the rate of operative vaginal delivery in Singapore was maintained at approximately 10% from 2012 to 2017.
Operative vaginal delivery in obstetrics is an integral part of obstetric care worldwide. 12 Instrument selection takes into account many factors, both patient and operator dependent. The choice of operator is paramount and is influenced by the operator’s experience and training; clinical scenarios; local practices; geographical location; and sometimes the mother’s preference. Clinical factors that must be considered are the station and position of the lowest part of the fetus; fetal head molding, morale, and maternal cooperation. The choice of instrument is sometimes limited by clinical circumstances. For example, for facial presentation and the presence of an after-coming head in the breech position, only forceps can be used as an option. By contrast, the success of a vacuum birth depends on the mother’s active participation in pushing, and her inability to do so may increase the risk of failure. Instrument selection is a difficult one because it has advantages and disadvantages. It was shown in a 2010 review that forceps are superior to a vacuum for successful vaginal birth, but this comes with an increased risk of adverse maternal outcomes. The success of forceps in achieving a vaginal delivery can be explained simply by the ability to direct greater operator force through the forceps when compared to a vacuum before the cup dislodges. Meanwhile, the higher vacuum failure rate is caused by suction failure and the risk of cup detachment. However, operator skill and correct technique for using instruments are the keys to successful operative vaginal delivery. There is an increase in maternal and fetal morbidity if the instrument is used not according to the recommended technique. Suboptimal placement is associated with an increased risk of neonatal trauma and cesarean delivery due to failure of vaginal delivery. 13
Current trends show that the operative vaginal delivery rate has declined overall, although both rates are very high varies around the world and the cesarean delivery rate has increased over the last decade (30.3% in the United States in 2005 and 21.3% in the United Kingdom in 2001). Of these operative vaginal deliveries, the percentage of forceps deliveries decreased while the percentage of vacuum deliveries increased. According to data from the World Health Organization (WHO), cesarean sections continue to increase globally, accounting for more than 1 in 5 (21%) of total births. This number will continue to increase over the next decade, with almost a third (29%) of all births likely to occur via cesarean section by 2030. 6 Operative vaginal birth is beneficial for women because it avoids cesarean birth and its associated morbidities. The short-term risks of cesarean birth include hemorrhage, infection, prolonged healing time, and increased cost. The long-term morbidities associated with cesarean birth include the high likelihood of repeat cesarean birth, the complications that can occur with labor after cesarean birth, and the risks of placental abnormalities such as placenta accreta. For the fetus showing signs of possible compromise, successful operative vaginal birth can shorten the exposure to additional labor and reduce or prevent the effect of intrapartum insults. 14 WHO has indicated that higher cesarean section rates do not reduce maternal and newborn deaths and recommends that higher rates of cesarean section range from 10% to 15%. However, figures in Indonesia have exceeded this range. Cesarean deliveries increased from 12% in 2012 to 17% in 2017, and Jakarta had the highest rate (31.1%). 15 In other countries, such as Korea, there was an increase in the frequency of cesarean deliveries from 4.9% in 1970 to 39.1% in 2015. This trend is related to maternal age, increasing rates of induced labor, and an increasing incidence of obesity among women. 16 Childbirth at a young (i.e., ⩽19 years old) or advanced maternal age (i.e., ⩾35 years old) is associated with an increased risk of adverse maternal perinatal outcomes, such as postpartum hemorrhage (PPH), eclampsia, and cephalopelvic disproportion, as well as adverse infant outcomes including preterm birth, poor fetal growth, low birth weight, and neonatal mortality. 17 Induction of labor is associated with less maternal satisfaction and potentially increased rates of instrumental delivery and cesarean section compared with spontaneous vaginal delivery. The medications used to induce labor—oxytocin or prostaglandin—might cause abnormal or excessive contractions, which can lessen fetal oxygen supply and lower fetal heart rate. 18 Women who are overweight have longer labors than women of normal weight. It can be harder to monitor the fetus during labor. For these reasons, obesity during pregnancy increases the likelihood of having a cesarean birth. 19
In response to the increasing number of cesarean deliveries and the morbidity associated with cesarean deliveries, the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists recently held a workshop to address the prevention of primary cesarean deliveries. Although the use of cesarean sections has grown rapidly and is considered safe, vaginal delivery has major advantages in reducing complications associated with the operation, such as death, PPH, surgical site infections and injuries, venous thromboembolism, recovery time, costs, and subsequent repeat cesarean sections. 20 The assumption that vaginal delivery, especially if it must be performed by an assisted instrument, is better than cesarean delivery is based on peripartum risks. The consideration in using a vacuum is the increased risk of complications in the baby, such as retinal hemorrhages and cephalhematoma. If vacuum delivery fails, the mother will most likely have to undergo a cesarean section, which also increases the risk of complications because a trial vacuum delivery has previously been carried out. While the use of forceps can result in various types of injuries to the mother’s birth canal and injuries to the baby, in infants, forceps can cause facial lacerations, eye and retinal injuries, skull fractures, nerve injuries, and even death. Women who deliver with forceps are at risk for pelvic organ prolapse, extended perineal tears, and vaginal lacerations. Although doctors can repair the tear, it causes the mother to have a longer recovery time than usual, resulting in pain and discomfort. 21 Concerns over neonatal and maternal safety have been a major factor in this trend, as fewer doctors trained in using forceps and able to teach residents. Professional responsibilities also have an impact, as birth injuries associated with delayed cesarean sections and difficult operative deliveries are common causes of obstetric malpractice claims. These risks can be minimized with the skills of a trained and experienced obstetrician. Require hundreds of deliveries by forceps and vacuum extraction to prevent or manage maternal or fetal complications. 4 According to ACOG Guideline 2020, Operative vaginal birth is used to achieve or expedite safe vaginal birth for maternal or fetal indications. Examples include maternal exhaustion and an inability to push effectively; medical indications such as maternal cardiac disease and a need to avoid pushing in the second stage of labor; the prolonged second stage of labor, arrest of descent, or rotation of the fetal head; and non-reassuring fetal heart rate patterns in the second stage of labor. Operative vaginal birth is beneficial for women because it avoids cesarean birth and its associated morbidities. The short-term risks of cesarean birth include hemorrhage, infection, prolonged healing time, and increased cost. The long-term morbidities associated with cesarean birth include the high likelihood of repeat cesarean birth, the complications that can occur with labor after cesarean birth, and the risks of placental abnormalities such as placenta accreta. For the fetus showing signs of possible compromise, successful operative vaginal birth can shorten the exposure to additional labor and reduce or prevent the effect of intrapartum insults. Often, operative vaginal birth can be safely accomplished more quickly than cesarean birth. The American College of Obstetrics and Gynecology (2020) recommends forceps and vacuum extractors have a low risk of complications and are acceptable for operative vaginal delivery. According to RCOG guideline 2020, Assisted vaginal birth should be performed by, or in the presence of, an operator who has the knowledge, skills, and experience necessary to assess the woman, complete the procedure, and manage any complications that arise. Assisted vaginal births that have a higher risk of failure should be considered a trial and be attempted in a place where immediate recourse to cesarean birth can be undertaken. 10
Regulation of the Indonesian Medical Council Number 86 of 2020 concerning Professional Education Standards for Obstetrics and Gynecology Specialists stipulates that vacuum extraction and forceps are still a skill list with competency level 4 (does), namely being able to do it independently. Obstetrics and Gynecology specialist graduates can demonstrate these skills by mastering all theories, principles, indications, steps on how to perform, complications, and complications control. Apart from having done it under supervision, testing ability level 4 skills using work-based assessments, for example, mini-CEX, portfolio, logbook, etc. 7
The decline in cases of operative vaginal delivery in practice, especially in teaching hospitals, is not beneficial for obstetrician medicine education because many residents are not comfortable and confident using forceps and vacuums. In the study of Feeley et al., 22 the obstacles that residents experience are proactive teaching, special training, and supervision, exposure to opportunities to gain experience, the attitudes and beliefs of mentors, and training programs. Additional barriers related to a lack of opportunities, such as staff preferences and specific hospital norms, negatively influence clinical learning opportunities (e.g., “choice of instrument is largely institution dependent”). Mannella et al. 23 stated that operative vaginal delivery simulation training significantly improved technical skills (Figure 3), increased success rates, and reduced the time required to complete the procedure. This simulation study was conducted on a mannequin. In all, 35 obstetrics and gynecology residents of the University of Pisa, Italy, were recruited and evaluated on a technical skills assessment scale from 0 to 55 points. They performed various simulations of operative vaginal delivery under vacuum and were evaluated by a tutor. After 8 weeks, the simulation training was repeated, and the trainees were re-evaluated by the same tutor. After 8 weeks from the first simulation session, trainees have been shown to improve their technical skills (46.27 ± 4.6 with a p-value < 0.0001) and their successful application rate (85.71% with a p-value 0.0161) and reduced time to complete the procedure (86.2 ± 29.9 s with a p-value of 0.0001). Mannella et al. 23 stated that operative vaginal delivery simulation training significantly improved technical skills, increased success rates, and reduced the time required to complete the procedure. According to this finding, perhaps new forms of teaching could be considered.
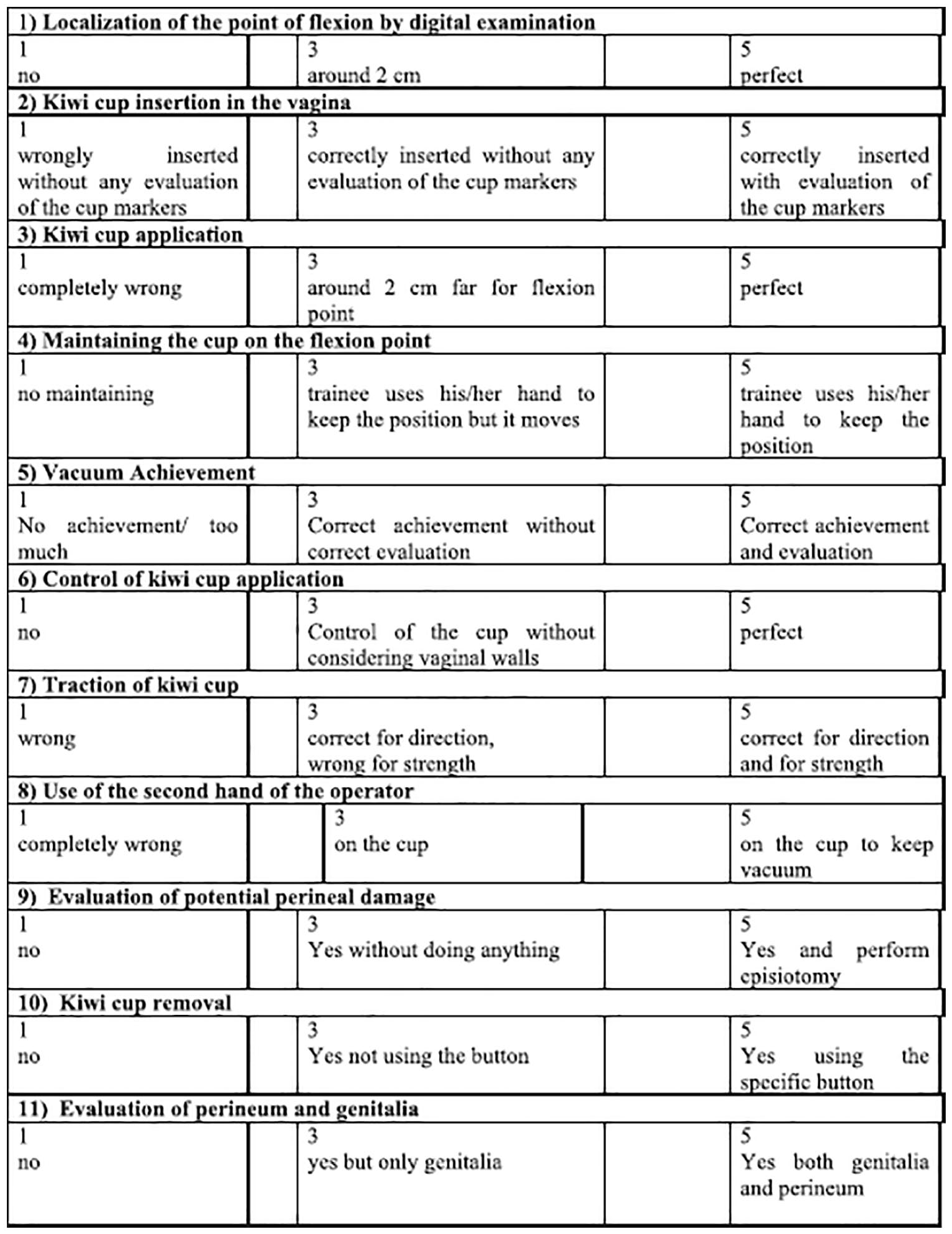
Assessment of technical skills to evaluation scale for kiwi-cup application. 23
This study has limitations in that it does not explain why there has been a decline in the use of vaginal delivery operations. This research is a retrospective study; important variables such as sociodemographic status, maternal body mass index, and instrument use were sequentially not addressed in this study. This research was conducted in the Bandung area, but it still does not represent West Java, Indonesia as a whole. Further research studying how educational interventions improve operative delivery skills might be considered.
Conclusion
This research shows the inadequacy of cases of vacuum extraction and forceps deliveries in teaching hospitals and AHS in West Java to meet the clinical skills standards of students, so it is suggested that there is a need for a metamorphosis of skills so that vacuum and forceps extraction skills can still be achieved.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
Khishotul Hayati wrote the proposal, gave training on data collection, analyzed the data, and drafted the paper. Mulyanusa Amarullah Ritonga and Tono Djuwantono approved the proposal with some revisions and participated in data analysis and manuscript writing. All authors read and approved the final manuscript.
Data availability statement
Data, models, and code supporting this study’s findings are available from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The department issued a letter of ethical approval on 10th May 2023, with reference no. LB.02.01/X.6.5/156/2023 by the chairman of the Research Ethics Committee of Dr. Hasan Sadikin General Hospital Bandung, West Java, Indonesia.
Informed consent
This research is a retrospective study that uses medical records, so there is no written or verbal informed consent; however, the ethical approval states that patient data will be kept confidential.
Consent form
Not applicable, because secondary data of discharged patients were collected from medical records with the approval of the ethical committee.
Trial registration
Not applicable.
Patient consent
Not required.