
Abstract
Objective:
Coffee holds a cherished place in Ethiopian culture, its consumption among students raises concerns despite its perceived benefits for alertness and productivity. Moderate caffeine intake remains unproblematic, but exceeding 400 mg daily can trigger detrimental health effects such as fatigue, memory impairment, and even attention-deficit disorder. Research on problematic coffee use among young adults, specifically Ethiopian students, remains limited, hindering our understanding of its potential scope and impact. To address this knowledge gap, researchers at Dilla University, Ethiopia, undertook a comprehensive study in 2022, focusing on the university’s student population. This investigation holds significant potential to unveil the previously obscured landscape of excessive coffee consumption in this demographic and inform future research and potential interventions.
Methodology:
An institutional-based cross-sectional study design was conducted in August–July, 2022. To measure problematic coffee use, this study used the Diagnostic Statistical Manual five criteria for substance use disorder. Those who scored >2 out of 11 criteria were considered to have problematic coffee use. To measure a significant association between the outcome and independent variable, a multivariable logistic regression analysis at p < 0.05 and 95% confidence interval was employed.
Result:
This study included 414 respondents. More than half of the respondents, 347 (59.7%) were male. Out of all respondents, 182 (44.0%) had a boy/girlfriend. Nearly half of the respondents, 218 (52.7%) were orthodox, Christian religion followers. According to this study’s findings, 137 (33.1%) respondents were considered to have problematic coffee use. Multivariable logistic regression analysis showed that 5–10 years duration of coffee use (AOR = 4.62, 95% CI: 2.96–7.85; p = 0.001), start to use coffee before joining university (AOR = 2.977, 95% CI: 1.332–6.653; p = 0.008) and 6–9 cups of daily coffee use (AOR = 3.26, 95% CI: 2.14–5.89; p = 0.00) were associated with problematic coffee use.
Conclusion:
This study showed that one-third of the respondents had problematic coffee use. The starting point, duration, and amount of use had a strong association with problematic coffee use. Hence, focusing on addressing the mental health challenges associated with problematic/excessive coffee consumption among higher education students is advisable. Additionally, promoting awareness of problematic/excessive coffee use and its potential remedies is recommended.
Introduction
Coffee is a beverage made from the roasted coffee seeds and beans of the coffee plant family. 1 It is dark, bitter, a little acidic, and stimulates people mostly because it contains caffeine. It is one of the most consumed beverages worldwide. 1
In Western Europe, particularly in England and Germany, coffee shops began to emerge in the late 17th century. Coffee’s religious overtones have persisted throughout the Horn of Africa and the Middle East, and the ritualistic practices there continue to be sophisticated and deliberate. 2
Coffee is a traditional beverage that is usually consumed early morning and in the daily social rituals of most Ethiopians. Even after relocating to the USA, Ethiopians and Eritreans carried out the coffee ceremonies. About half of Ethiopia’s yearly coffee harvest is consumed domestically and the remainder is exported. 3 Although coffee has certain cognitive benefits, such as increasing alertness, energy, and feelings of well-being, excessive consumption can have several negative side effects, such as disrupted sleep, jitters, irritability, and gastrointestinal distress. 4
The caffeine contents in coffee ranges from 50 to 143 mg/177 ml. 5 The caffeine content of coffee is influenced by various coffee preparation methods. 5 Caffeine has a 6-h half-life, which means it takes 6 h for the chemical to be obliterated by the body. Evidence suggests that consumption of ⩽400 mg caffeine/day in healthy adults is not associated with adverse cardiovascular, behavioral, reproductive, acute, or bone status effects. 6 When consumed in excess dose, coffee has a particularly negative psycho-physiological effect on the human body that promotes insomnia, anxiety, nervousness, restlessness, and rambling thoughts and is linked to several harmful health effects.7–9
The amount of coffee used up to five cups or equivalent to 500 mg doses of caffeine may increase alternates, agitation, insomnia, and heart rate. 10 Students have consumed coffee in many higher educational institutions around the world. For instance, high intake is reported among students in 92% of students in the United States, 11 98% of the Bahrain population, 12 and 58% in Saudi Arabia. 13
Common withdrawal symptoms after consuming coffee include headache, exhaustion, trouble concentrating, and dysphoric mood. In these cases, the neurotransmitter Gamma-aminobutyric acid (GABA), which helps control anxiety, appears to be depleted, and the impacts of our two main stress hormones, cortisol, and adrenaline, are amplified. 14 Most people can safely consume low-to-moderate amounts of coffee, but those who are more susceptible to cardiovascular problems and pregnancy complications should avoid consuming more coffee. 15 Caffeinated drinks like coffee are used as a stimulant that enhances wakefulness. It is used widely in Ethiopia among college students. 16 Medicine and health science students had a higher course load as compared with other disciplined studies as a result they drink coffee for study purposes.17,18 The university is situated close to a significant coffee trading hub. One of the top coffee brands exported to several Western nations is Yirga Cheffe. 19
Several studies suggest among university students males consume more caffeine when compared to females.20–22 Most students use coffee during times of academic stress and excessive caffeine consumption results in irritability, fatigue, poor sleep, and subsequently affects academic performance.12,20–22 Furthermore, another study done in Saudi Arabia suggested that factors like being male, young adults, unmarried, poor sleep patterns, and smokers were highly likely to influence patterns of coffee use. 23 Coffee is consumed in different social worlds, ethnic and religious backgrounds. 24 Furthermore, the patterns of use might be influenced by religious practices. 25
There have not been numerous studies done on excessive coffee consumption despite the negative impact it has on people’s physical and mental health in the young adult population. Therefore, the purpose of this study was to evaluate problematic coffee use and its contributing factors among students of medicine and health sciences at Dilla University.
Methodology
Study area and period
The study was done at Dilla University, located in the southern part of Ethiopia. Dilla University has an estimated 30,108 students enrolled. The university has 51 undergraduate and 21 graduate departments, which provide regular, extension, and summer courses at the BA/BSc, Bed, MA/MSc, and PhD levels. Students from medicine and health at Dilla University participated in the study. The research was carried out in 2022 between July and August.
Study design
This study was an institutional-based cross-sectional study design.
Source population
All students who attend Dilla University, college of Medicine and Health Science in the study period.
Inclusion and exclusion criteria
The inclusion criterion for this study was all students who have been consuming coffee for the past 3 months and those with physical or mental illness were excluded from the study.
Outcome variable
Problematic coffee use.
Independent variables of the study
Sex, religion, monthly pocket money, residence, relationship status, department, year of student, average grade, duration of use, starting period, comorbid substance use, and family history of substance use.
Sample size determination, sampling techniques, and procedures
The sample size was calculated using the formula for population proportion at confidence interval CI = 95%, at 95% + 1.96, the estimate of the population proportion, p = 50 since no study was conducted on the study area and margin of error, W = 5% or 0.05 then the required sample of the study will be calculated as follows; n = (zα/2)2 p (1−p)/d2 = 384, For possible non-response during the survey, the final sample size is increased by 10% to n = 384 + 10% which is 38.4 = 422.
All the eight departments (medicine, Health officers, midwifery, clinical nurse, psychiatry, anesthesia, environmental health, and pharmacy) under medicine and health science with their level of academic years (batches) were included in this study. The study was carried out in a multi-stage sampling technique for recruiting study participants. Students were stratified based on their batch/academic year and the sample size was distributed using probability proportional to size. Consequently, the final sample size was allocated proportionally based on the number of students in each department based on the number of students with the level of academic years (batches). Finally, a simple random sampling technique was used to select participants by using their identity card number as a sampling frame (see Figure 1).
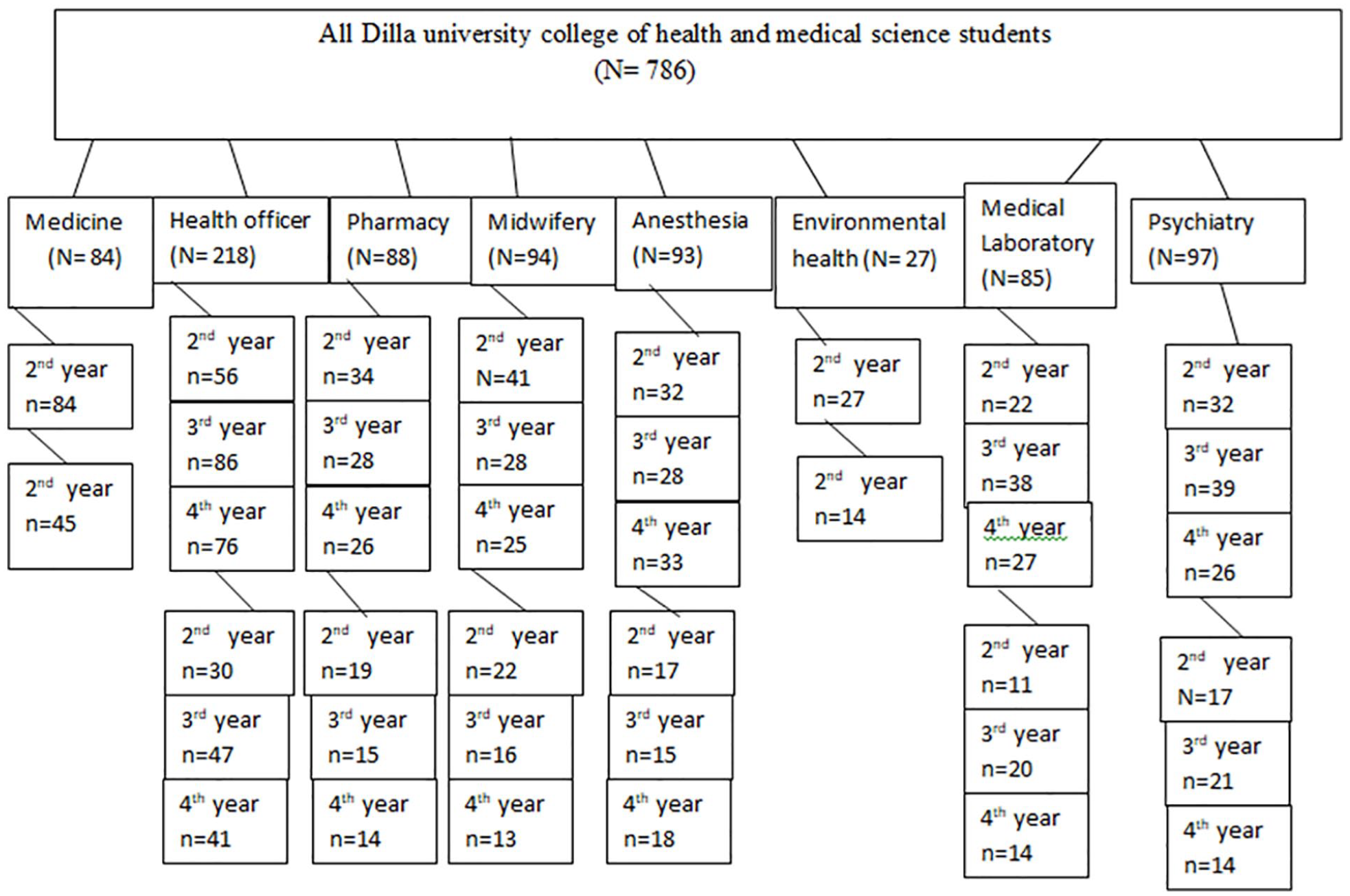
Graphic illustration of a proportional allocation sampling procedure among respondents at Dilla university, Ethiopia (N = 422).
Data collection instruments
A Diagnostic Statistical Manual-5 criterion (DSM-5) of substance use disorder was used to measure caffeine use disorder. According to the DSM-5 criteria, a diagnosis of substance use disorder is based on evidence of impaired control, social impairment, risky use, and pharmacological criteria. 26 Problematic coffee use is diagnosed when a maladaptive pattern of substance use leads to clinically significant impairment or distress, as manifested >2/11 occurring at any time in the 12-month period. 27 Several evidence proposed to use the same criteria as substance use disorder to assess caffeine use disorder. There is need for future research to that encourages the validity, and prevalence of caffeine use disorder. 28 The reliability of DSM-5 criteria for coffee use disorder assessed in our study was Cronbach’s α of 0.80.
In this study students’ coffee use was measured based on a subjective response to a cup of coffee they used on a daily basis.
The alcohol, Smoking, and Substance Involvement Screening Test (ASSIST-3.0) was used to evaluate the individuals’ current alcohol, tobacco, chewing gum, and cannabis use. It was created by the World Health Organization to identify the use of psychoactive substances and associated issues in patients receiving primary care.29,30 The scale has sensitivity and specificity 97% and 90% respectively. 31 The average reliability of the ASSIST with Cronbach’s α range of 0.58–0.90 and has good validity tested in various countries. 29
Participants were classified as current substance users if they had used any psychoactive substance in the last 3 months. 32
Current comorbid substance use was assessed using a subjective response to respondents’ additional psychoactive substance use such as khat, cigarettes, and alcohol simultaneously with coffee for the last 3 months period. 33
Current family history of substance use: Based on respondents’ subjective responses, it was determined whether their immediate family members had used alcohol, cigarettes, khat, or any other psychoactive substance within the previous 3 months. 34
Data collection procedures
To ensure its accuracy, the questionnaire was first written in English, translated into the Amharic-speaking area’s language, and then returned to English. At Bulle Horra University, 5% of the estimated sample participated in pretesting of the questionnaire. Based on the feedback from the pre-test, the questions were modified. Both the supervisors and data collectors received 2 days of training. The data collectors explained the goals of the study to the study participants. The participants were given enough time to complete the questionnaire. The data collection was completed timely.
Statistical analysis and interpretation
The collected data was coded, entered into EPi-data version 3.1 and exported to SPSS version 24 for analysis. EPI-data version 3.1 is an open-source software developed by the Open Science Collaboration (https://github.com/HardNorth/github-version-generate), while SPSS version 24 is a commercial software produced by IBM (https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-24) A logistic regression analysis was performed to identify associated risk factors for problematic coffee use and presented as odds ratios (OR) with 95% confidence intervals (95% CI). Bivariate logistic regression analysis was used to assess the correlates of independent factors with problematic coffee use with a p-value of <0.25 were considered as candidates for multivariable logistic regressions. Variables with a p-value less than 0.05 were considered statistically significant associations between independent factors and problematic coffee use.
Results
Sociodemographic characteristics
This study sample size was 422 with a 98% response rate. The respondents included in the study are 414. According to this study result, more than half of the respondents 247 (59.7%) were males and the mean age of respondents was 22.1 (±2.5) ranging from 19 to 25 years old. Among the respondents, the department of pharmacy had the highest concentration with 88 students (21.3%), followed by second-year students with 152 (36.7%). Nearly half (44.9%) had a GPA between 3.5 and 4.0, while 41.1% came from western Ethiopia (see Table 1).
The sociodemographic characteristics of respondents at Dilla University, Ethiopia (n = 414).

Substance-related factors
Out of the 11 items used to measure problematic coffee use, 305 (73.7%) of respondents said yes to the item “Experiencing intense cravings or urges using the substance.” On the contrary, 14 (3.4%) of them responded yes to the item “Continuing to use even when it causes relationship problems.” After summing up the total items of a substance use disorder, 137 (33.1%) of them scored >2/11 and were considered problematic coffee use (see Table 2).
The distribution of Dsm-5 items for problematic coffee use among medical and health science students of Dilla university, Ethiopia (N = 414).

Psychosocial variable results
More than half of the respondents, 236 (57%) of them had <5 years history of coffee use. Nearly half of the participants, 210 (51.8%) had started to use coffee after joining the university (see Table 3).
The distribution of psychosocial factors for problematic coffee use among medicine and health science students of Dilla university, Ethiopia (N = 414).

Comorbid: Additional use of a substance (khat, cigarette, alcohol).
Logistic regression analysis data
From all variables entered into logistic regression analysis, coffee use starting time and duration of coffee use were statistically significant with the outcome variable. During multivariable logistic regression analysis, 5–10 years duration of coffee use (AOR = 4.62, 95% CI: 2.96–7.85; p = 0.001), start to use coffee before joining university (AOR = 2.977, 95% CI: 1.332–6.653; p = 0.008) and 6–9 cups of daily coffee use (AOR = 3.26, 95% CI: 2.14–5.89; p = 0.01) were variables associated with problematic coffee use (see Table 4). This study found that participants with prior coffee use before joining college had three times the odds of problematic coffee use compared to those with no past use history (AOR = 2.977, 95% CI: 1.332–6.653; p = 0.08). The respondents who used coffee for 5–10 years had five times the odds of having problematic coffee use (AOR = 4.62, 95% CI: 2.96–7.85; p = 0.001) than those who used coffee for less than 5 years. Furthermore, this study found that the respondents who used 6–9 cups of daily coffee had four times the odds of having problematic coffee use (AOR = 3.26, 95% CI: 2.14–5.89; p = 0.01) than those who used <1–3 cups coffee.
Multivariable logistic regression analysis of problematic coffee use among medical and health science students at Dilla University, Ethiopia (N = 414).

Comorbid: Additional use of substance (khat, cigarette, alcohol). *P value less than 0.05 and statistically significant.
Discussion
The pervasiveness of coffee in Ethiopia’s southern region extends beyond simple beverage preference, as evidenced by research revealing a concerning prevalence of problematic coffee use (33.1%). This multi-variable logistic regression analysis identified a significant association between duration and intensity of coffee consumption, with individuals consuming coffee for 5–10 years five times more likely to exhibit problematic behaviors than those with shorter histories. Furthermore, pre-existing coffee consumption prior to college enrolment tripled the odds of developing problematic habits among students, suggesting a potential link between long-term habitual use and unhealthy patterns. This study found that 137 (33.1%) of them developed problematic coffee use which was lower than the study done in the United States, 92%, 11 Bahrain population, 98%, 12 and Saudi Arabia, 58%. 13 This might be because European and Asian students had more laid-back lifestyles, experienced colder winters in Europe, enjoyed the hospitality of Arab people, frequently consumed caffeinated drinks, candies, and gum, and had more disposable income. 35
This study found that the respondents who used coffee for 5–10 years had five times the odds of having problematic coffee use than those who used coffee for less than 5 years. This was a similar finding to a study in France 36 and Singapore. 37 It might be because, following prolonged drug use, the brain starts to adjust to dopamine spikes. Drug users may subsequently experience exceptionally low levels of dopamine in the reward circuit of their brain, which limits their ability to experience any pleasure.38,39
This study found that the respondents who used 6–9 cups of daily coffee had four times the odds of having problematic coffee use than those who used <1–3 cups of coffee. Most recent reports European Food Safety Authority suggest that daily caffeine intakes from all sources up to 400 mg per day (4 cups) do not raise safety concerns for adults, except for pregnant women. 40 Other studies suggest risks of cardiovascular mortality and disease with intakes of more than three to four cups a day when compared to those taking none. 41 In addition, excessive coffee consumption can cause symptoms such as anxiety, agitation, insomnia, and gastrointestinal disorders. 42 Evidence suggests that negative effects of coffee tend to emerge with excessive drinking (more than 2–3 cups or 300 mg/day) so it is best to avoid heavy coffee intake. 43 On the contrary, a lot of evidence suggests that coffee consumption is also beneficial for wide a range of health outcomes except pregnancy. The researchers suggested that it has risk reduction for many health outcomes at three to four cups a day, and has benefit to health than harm. 41 Even though still there is contradicting evidence this might be due to the strength of the study. Most studies are observational rather than RCT. 41 This might also be quite different from the finding of our study that probes for further investigation.
This study finding showed that participants with prior coffee use before joining college had three times the odds of problematic coffee use compared to those with no past use history. This study finding was similar to the study done in Harar, Ethiopia. 44 It can be because drugs take time to cause physiological and psychological dependency. Recent evidence elaborates that prolonged substance use in adolescents shows that abnormality in brain functioning. These abnormalities ranged from brain structure volume, white matter quality, and cognitive tasks all of which contribute to psych-physiological dependence. 45 Coffee is a popular beverage in the southern region of Ethiopia. 3 Students consume coffee in many higher educational institutions in Ethiopia because of its high availability. 16 The reason for not including the other sources of caffeine intake in this study is because coffee is the main caffeine source among university students. Since it did not take into account other sources of caffeine use the finding should be interpreted taking this into account.
Limitations of study
This study’s findings, while insightful, must be considered within its limitations. Focusing only on young university students at a single institution limits generalizability. Additionally, assessing only recent, not lifetime, occurrences of problematic coffee use and excluding other caffeine sources and coffee types restricts the picture. Future research should address these gaps by evaluating long-term health impacts, academic performance effects, potential detrimental health consequences, and psychological implications of problematic coffee use. This broader focus would paint a more comprehensive picture of this issue in the Ethiopian student population.
Conclusion
This study identified a concerning pattern of coffee consumption among a significant proportion of students, characterized by intense cravings and a positive correlation between early initiation, high intake, and negative outcomes. These findings suggest a potentially troubling association between student coffee habits and psychiatric concerns, highlighting the need for targeted counseling and awareness initiatives within higher education settings. To ensure student well-being, it is crucial to address the mental health implications of coffee use patterns within this population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241235455 – Supplemental material for Problematic coffee use and associated factors among medical and health science students in Dilla University, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121241235455 for Problematic coffee use and associated factors among medical and health science students in Dilla University, Ethiopia by Chalachew Kassaw, Rediet Regasa, Misrak Negash, Amare Alemwork, Lulu Abebe, Solomon Yimer, Tamrat Anbesaw and Selamawit Alemayehu in SAGE Open Medicine
Footnotes
Acknowledgements
Our heartfelt appreciation goes out to Dilla University’s student service director and registrar’s office for their invaluable assistance in acquiring crucial data about the study area. We extend our warmest gratitude to the dedicated participants who volunteered their time and insight to this research.
Author contributions
In a collaborative effort, all authors conceived the study, gathered and analyzed data, drafted and revised the report, and equally contributed to design and statistical analysis.
Availability of data and materials
All data generated or analyzed during this study is included in this published article. The data set of the current study is available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participation
Ethical approval was obtained from the Institutional Review Board (IRB) of Dilla University College of Health Sciences and medicine (Ref No: duirb/112/22-05). After the purpose and objectives of the study had been informed, oral and written consent was obtained from each study participant before the start of the data collection. All necessary methods were carried out following the guidelines of the institutional and Declaration of Helsinki.
Informed consent
Verbal and written informed consent was obtained from all subjects before the study.
Consent for publication
Not applicable.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.