
Abstract
Craniosynostosis, marked by premature cranial suture fusion, necessitates prompt intervention to avert developmental, neurological, and aesthetic issues. While high-income countries have advanced in managing this condition, low- and middle-income countries grapple with substantial healthcare access disparities. This narrative review explores current craniosynostosis management in low- and middle-income countries. The review focused on studies published between 2008 and 2023. The focus was neurosurgical outcomes, and the search utilised databases like PubMed, EMBASE, Google Scholar, the Cochrane Library and Scopus, incorporating specific keywords and phrases. An in-depth analysis of 21 included studies reveals noteworthy positive outcomes, including low mortality, successful corrections and sustained efficacy. These advancements stem from enhanced pre-operative strategies, surgical techniques and postoperative care. Nonetheless, challenges persist, encompassing complications, mortality, reoperations, and treatment disparities, particularly in low- and middle-income countries constrained by financial and expertise limitations. The enhancement of clinical practice and the formulation of effective policies in the future entail several key strategies. These include the reinforcement of specialised healthcare infrastructure and diagnostic capabilities, the ongoing training and retention of neurosurgeons, the improvement of funding mechanisms, and the promotion of equitable access. Additionally, a crucial focus is placed on fortifying paediatric neurosurgical care in low- and middle-income countries. The recommendations underscore the importance of collaborative initiatives, the development of specialised healthcare infrastructure, and the implementation of strategic policies to not only advance pediatric neurosurgical care but also to address existing gaps in management.
Keywords
Background
Craniosynostosis is a congenital disorder characterised by the premature fusion of one or more cranial sutures. This fusion results in an abnormal head shape and may precipitate various developmental and neurological complications. Its aetiology can be attributed to both genetic and environmental factors1,2 and can be classified as ‘simple’, with the involvement of a single suture, or ‘complex’, where multiple sutures are affected (Figure 1). Further classifications divide the disorder into ‘syndromic’ forms (e.g. Apert, Crouzon and Pfeiffer) and ‘non-syndromic’, with approximately 75% of cases being non-syndromic in nature, while 25% are syndromic. 1
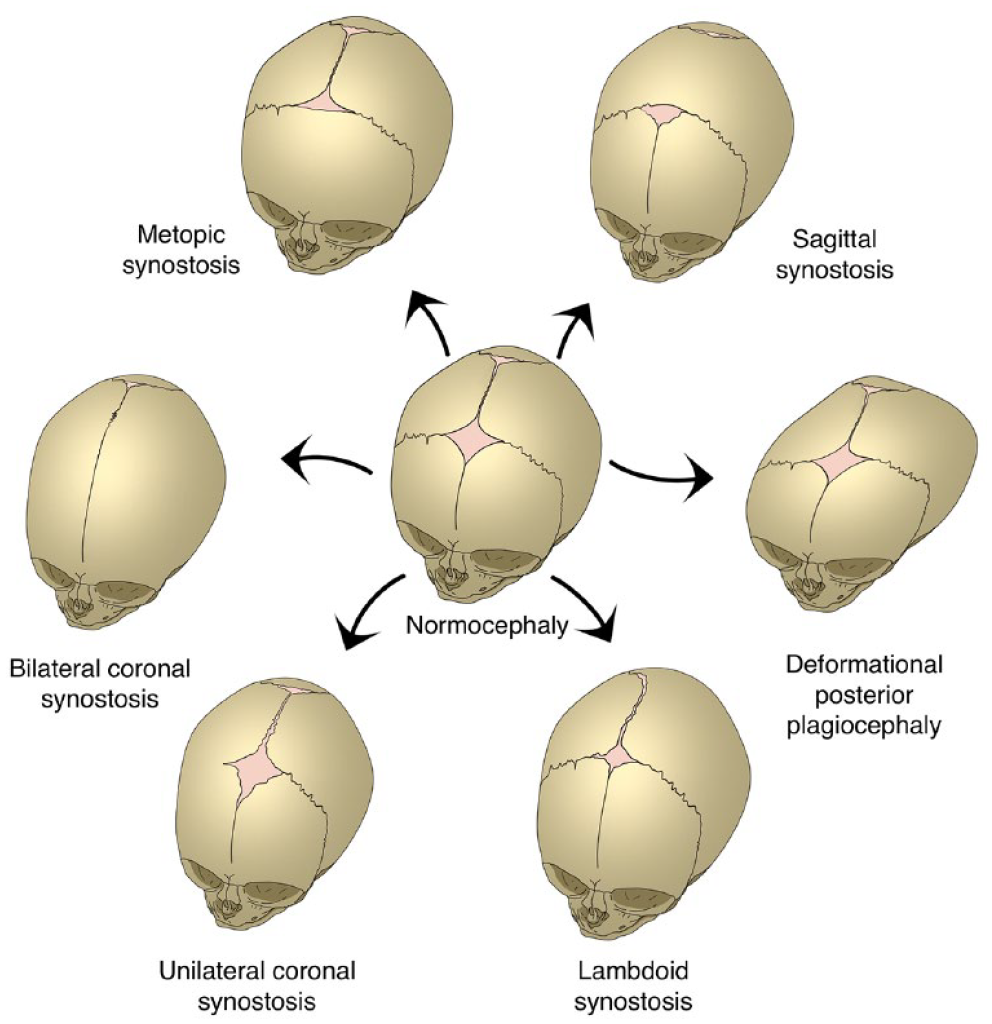
An illustration depicting the various manifestations of craniosynostosis based on the abnormal fusion of different sutures.
Non-syndromic craniosynostosis primarily manifests as an irregular head shape and asymmetry, with the potential for developmental delays stemming from restricted brain growth. 3 Conversely, syndromic craniosynostosis encompasses a broader spectrum of craniofacial abnormalities. Specific syndromes exhibit distinct traits: for instance, Apert syndrome features syndactyly, Crouzon’s is associated with cervical vertebral fusion, and Pfeiffer’s is characterised by broad thumbs and toes. Other distinctions include Muenke’s association with macrocephaly and Kleeblattschädel’s tri-lobar head shape and hydrocephalus1,4 (Figure 2). Intellectual disabilities may be present in certain syndromes, such as Apert’s, whereas others, such as Crouzon’s, typically have normal intelligence.1,4 Without timely intervention, craniosynostosis can result in significant complications, encompassing developmental delays, facial deformities, sensory and respiratory dysfunctions, neurological deficits, ocular abnormalities and concomitant psychological disorders. 3

An overview of the spectrum of signs and phenotypes present in syndromic and non-syndromic craniosynostosis.
Given these challenges, the need for prompt diagnosis and a comprehensive treatment approach is evident. 3 Surgical treatments, including suterectomies and craniotomies, are central to craniosynostosis management. These interventions primarily aim to expand the cranial vault space to support appropriate brain growth 1 and to improve the patient’s aesthetic appearance.
In high-income countries (HICs), significant progress has been made in understanding and addressing this condition. However, low- and middle-income countries (LMICs) face substantial disparities in healthcare access and resource distribution. 5 While there is a growing body of literature advocating early intervention’s role in mitigating the consequences of craniosynostosis, the implementation of these guidelines in LMICs is restricted. A comprehensive review of current studies highlights a research gap regarding craniosynostosis presentation, treatment and long-term results in LMICs. 5 A geographical distribution analysis identified 9 (37.5%) from Europe, 8 (33.3%) from the Americas, 4 (16.7%) from the Western Pacific, 2 (8.3%) from Africa, and 1 (4.2%) from the Eastern Mediterranean. 5 Only 4% of these studies originated from low-income nations. Moreover, the variability in socio-economic, cultural, and infrastructural aspects in LMICs contributes to a heterogeneous landscape of craniosynostosis management practices. 6 Factors such as limited financial resources, infrastructural constraints, and a shortage of specialised healthcare professionals impede the disease’s precise diagnosis and timely interventions in LMICs.7–10
This review endeavours to conduct a comprehensive examination of the literature pertaining to craniosynostosis in LMICs. The review aims to shed light on the specific challenges prevalent in LMICs that contribute to the observed global disparities in the management of craniosynostosis, and highlight avenues for improved care outcomes in LMICs. To uphold a standard of high quality, this narrative review has consistently utilised the Scale for the Assessment of Narrative Review Articles (SANRA) scale throughout the manuscript. 11
Methodology
The narrative review methodology involved a comprehensive search of published studies reporting facility-based outcomes or mortality for patients who underwent management procedures for craniosynostosis presentations in LMICs based on the World Bank Income Groups. 12 This includes low-income, lower middle-income, and upper middle-income countries. The application of the SANRA scale has been employed to ensure the rigorous quality of this narrative review.11,13
The study inclusion criteria covered various designs such as descriptive, case-control, cohort, observational, and randomised controlled trials, focusing on both syndromic and non-syndromic craniosynostosis. Eligible studies included comorbidity and previous pharmacological or surgical treatments across both paediatric and adult populations. Only full-text articles in English, published from 2008 to 2023, reflecting current neurosurgical practices in LMICs for managing craniosynostosis were chosen. The review emphasised neurosurgical outcomes in LMICs, excluding studies not reporting outcomes or those not focusing on cerebral or cranial areas (e.g. ocular outcomes of craniosynostosis (CS) treatment).
Databases such as PubMed, EMBASE, Google Scholar, the Cochrane Library and Scopus are used. The search term employed included keywords such as ‘craniosynostosis’, ‘neurosurgery outcomes’ and ‘management’. These terms were combined with phrases such as ‘low and middle-income country’, ‘LMICs’, ‘developing country’ and ‘resource-limited state’ to understand the review in the context of LMICs. Moreover, a manual search was conducted to include references from recently published procedure-specific reviews. Stand-alone abstracts and unpublished studies were excluded from the review.
The review did not impose a strict sample size requirement to ensure the inclusion of literature from smaller centres with lower numbers of admissions of craniosynostosis cases. Only studies providing raw data were included, while those with estimated or modelled numerator or denominator values were excluded.
This review aims to provide a high-quality academic assessment of the management of craniosynostosis in LMICs through a rigorous approach to synthesising data. A summary of the methodology is illustrated in Table 1.
Summary of the methodology.

LMICs: low- and middle-income countries.
Surgical management outcomes of craniosynostosis in LMICs
The studies reviewed provide valuable insights into the positive and negative outcomes of various surgical interventions for craniosynostosis in various LMICs. These findings provide a thorough understanding of the relevant presentations, diagnostic methods, management procedures and challenges of surgical approaches in LMICs. Twenty-one studies from various countries were meticulously analysed, shedding light on the geographical distribution of research efforts on the neurosurgical management of craniosynostosis, as illustrated in Figure 3. Notably, India emerges as a focal point, contributing the most studies, totalling four. Three of these studies use a retrospective design, while one uses a prospective design.

A map depicting the geographical distribution of the included studies.
Positive outcomes
Absence of mortality
The absence of fatalities in craniosynostosis surgeries underscores the safety of this neurosurgical correction. Exploring this outcome is critical for identifying the factors underpinning secure procedures and enabling their application across various healthcare contexts. Several studies corroborate the lack of fatalities associated with this intervention.14–27 This safety pattern emerges from a combination of factors, including improved surgical methods and advancements in both pre- and post-operative care. This mortality rate reflects effective complication management, which improves patient outcomes and ensures their wellbeing during the surgical procedure.
Variation in surgical procedures and their efficacy
Evaluating the success rates of craniosynostosis correction is critical to assessing the effectiveness of various surgical methodologies. Such evaluation paves the way for advocating the most efficacious techniques and technologies, resulting in optimal patient outcomes. Notable advancements in craniosynostosis corrective procedures are evidenced by their successful application in the field.14,15,28–32 For instance, metopic synostosis treatment often involves a bifrontal craniotomy followed by subsequent bifrontoparietal bone graft remodelling.14,29 Additionally, sagittal synostosis interventions commonly entail supraperiosteal dissection, strategic burr-hole placements, and craniotomies, further incorporating occiput and bifrontal fragment remodelling and frontal and parietal bone resection.15,30 Coronal synostosis is addressed by bifrontal craniotomy, rongeuring of the greater wing of the sphenoid, dural plication as necessary and frontal bone remodelling.28,31 Lambdoid synostosis treatments include barrel stave osteotomy with craniotomy and cranial bone strut placement. 32 A unilateral frontal craniotomy, followed by the application of a pericranial flap for coverage and drainage, was another effective procedure observed. 29
Minimal complications
Examining complications arising from surgical interventions is essential for evaluating the overall quality of these procedures. Through this analysis, one can identify factors mitigating complications, thus shaping guidelines to improve patient care. The studies reviewed consistently denote successful surgical outcomes with limited complications.14,15,21,22,28–32 When specified, complications are infrequent, encompassing instances like postoperative wound infections, intraoperative durotomies, scar revisions, dural tears and transient focal neurological deficits.
Positive outcomes with long-term follow-up
The sustained success of surgical procedures is vital for assessing the long-term efficacy of craniosynostosis management and aiding in refining ongoing care practices. Several studies present robust evidence of the enduring efficacy of surgical interventions, consistently reporting favourable outcomes during extended follow-ups.18–20,27 The capacity to maintain these positive outcomes over an extended period of time underscores these procedures’ effectiveness in addressing craniosynostosis’s complex challenges. Furthermore, the reliable outcomes seen during extended follow-ups accentuate the reliability and durability of the surgical strategies employed in craniosynostosis management.
Negative outcomes
Surgical complications
Examining the complications of craniosynostosis surgeries elucidates potential risks and challenges. Several studies have identified concerns, including intraoperative durotomy, postoperative infections, and unforeseen fractures.14,17,21,29 Postoperative complications such as infections, significant blood loss, and the subsequent need for interventions have also been reported.21,28,30 These findings underscore the necessity for thorough risk assessments, precise procedure execution and vigilant post-operative care. By proactively addressing these concerns, clinicians can refine their techniques, leading to improved patient care and enhanced clinical outcomes.
Mortality
The analysis of mortality rates in craniosynostosis surgeries aids in comprehending the nuances of patient selection, procedural execution and postoperative care. This is critical to improving intervention safety and mitigating fatality rates. Some studies have reported mortality instances both intra- and postoperatively within their research cohorts.18,33 Further investigating these instances is pivotal for understanding the broader context of craniosynostosis neurosurgical interventions, setting the stage for improved safety measures and understanding.
Need for reoperations
The requirement for reoperations in craniosynostosis management emphasises the condition’s complex nature. Understanding the reasons for such reoperations can lead to improved surgical techniques, pre-operative planning, and specialised aftercare. Several studies reported the need for additional surgeries after the initial procedures.14,17,21,22,30 Most of these were due to postoperative complications and suboptimal postoperative outcomes. The recurrent need for surgeries underscores the condition’s multifaceted challenges, highlighting the importance of continuous monitoring, flexible treatment regimens and effective management of unforeseen complications.
Persistent symptoms
Assessing persistent symptoms after craniosynostosis surgeries enables the refinement of treatment modalities, aiming for superior long-term patient quality of life. Bansal et al. 15 and Liu et al. 31 identified cases with persistent symptoms, such as elevated intracranial pressure (ICP), necessitating further intervention. Identifying these instances underscores the condition’s nuanced complexity and requires a comprehensive exploration of factors contributing to these enduring symptoms. Such recognitions promote a deeper understanding, potentially paving the way for more proficient treatments and patient care. The craniosynostosis neurosurgical management types and outcomes in our study have been summarised in Table 2.
Outcomes and types of neurosurgical management for craniosynostosis with variable presentations in low- and middle-income countries.

CT: computed tomography; MRI: magnetic resonance imaging; CS: craniosynostosis; VPS: ventriculoperitoneal shunt; MDCT: multidetector computed tomography; GA: general anaesthesia; ICP: intracranial pressure; EVD: external ventricular drainage; SSI: surgical site infection; mL: millilitres; Post-op: postoperative; PVDO: posterior vault distraction osteogenesis; RAMD: robot assisted midface distraction; RAFFA: robot assisted frontofacial advancement.
Discussing the gaps in LMIC paediatric neurosurgery capacity for craniosynostosis management
Limited accessibility to specialised healthcare infrastructure
The provision of specialised healthcare facilities, particularly advanced neurosurgery units, is critical for effectively addressing complex congenital conditions such as craniosynostosis. A significant number of LMICs face a shortfall in these resources, complicating the management of craniosynostosis and other paediatric anomalies.
Over three-quarters of patients in LMICs struggle with accessing adequate neurosurgical care, often travelling more than 2 h for emergency neurosurgical interventions. 7 Despite over 60% of Africa’s population residing in rural areas, 90% of its paediatric surgeons are based in urban centres. 35 This urban concentration requires rural patients to undertake long journeys to cities, a challenge exacerbated by the region’s underdeveloped transportation networks. 36
The financial constraints of LMICs further complicate the acquisition and maintenance of modern neurosurgical tools such as operational microscopes, neuro-navigation systems, and stereotactic devices.9,10 In low-income countries (LICs), there is a significant dearth of basic neurosurgical equipment, with several countries highlighting a critical need for microscopes, microinstruments and drills. 7
Furthermore, essential imaging equipment, such as MRI and CT scanners, vital for diagnosis and pre-surgical evaluations, is limited or subpar. 37 A study in Afghanistan reported that of 16 surveyed hospitals, only ten possessed CT scanners, predominantly in private or military institutions. 38 A mere six reported having MRI facilities, with a majority again being from the private or military sectors, underscoring a significant deficit in vital diagnostic resources in the public healthcare domain. 38
Beyond the immediate financial considerations, the maintenance of these complex tools presents challenges due to a lack of experienced technicians. The absence of established protocols for the use and sterilisation of such devices, combined with suboptimal monitoring, increases the risk of surgical site infections, compromising patient safety.
Concurrently, the challenge of developing and maintaining dependable electronic medical records impedes continuity of care. 39 Many LMICs still depend on manual record-keeping, increasing the risk of data inaccuracies or omissions. 40 Collectively, these issues pose significant barriers to neurosurgical care delivery in LMICs, emphasising the urgency for a collaborative approach to address these multifaceted challenges.
Scarcity of specialised paediatric neurosurgeons and multidisciplinary teams
In LMICs, the availability of specialised neurosurgeons, particularly those focused on paediatric care, is limited.9,41 For context, approximately 330 paediatric neurosurgeons are responsible for the care of 1.2 billion children within LMICs. 7 This disparity is more pronounced in low-income African countries, with a density of approximately one paediatric neurosurgeon for every 30 million children. 7 Illustrating this demand, a tertiary health facility in southwest Nigeria reported paediatric neurosurgical diseases constituting a fifth of the overall neurosurgical workload. 42
Beyond the numbers of neurosurgeons available, the quality of care and expertise also pose a challenge. The lack of specialised training institutions, combined with insufficient investment in continuous professional development, impedes the growth of the neurosurgical workforce.10,38,43 Moreover, comprehensive neurosurgical care for complex conditions, such as craniosynostosis, requires an integrated approach involving various healthcare professionals: paediatric reconstructive surgeons, plastic surgeons, surgical nurses, radiologists, and others. Absent or inadequate collaboration among these professionals can compromise patient care. 36 To further illustrate the severity, a marked shortage of plastic surgeons exists in 16 LICs, suggesting an estimated 229 million individuals, including 82.6 million children, may lack access to these critical healthcare services. 44
Socio-economic barriers to paediatric neurosurgical care
Socio-economic determinants significantly influence the accessibility and standard of paediatric neurosurgical care in LMICs. An estimated 5 million individuals in LMICs require, yet remain deprived of, neurosurgical interventions annually due to limited capacities and resources. 45 The substantial financial burden associated with consultations, surgical procedures, post-operative care, and pharmaceuticals often presents insurmountable challenges for families, especially in the absence of robust public health frameworks. 46 Consequently, children may experience prolonged delays in accessing neurosurgical care or, in certain cases, might not receive the required interventions.
Misconceptions and societal stigmas associated with neurological ailments can result in treatment delays or outright refusal of treatment from patients without sufficient background information. 6 In certain contexts, cultural convictions may prioritise traditional remedial practices over contemporary medical interventions, further distancing these communities from potentially critical neurosurgical procedures. 47 Additionally, families with limited educational backgrounds may lack awareness of certain neurosurgical disorders, notably congenital anomalies. Such unawareness can cause deferred diagnosis, hindering prompt and efficient treatments. 48 Resultantly, this complex interplay of socio-economic factors underscores the need for comprehensive, targeted interventions to promote equitable paediatric neurosurgical care accessibility in LMICs.
Research gaps on craniosynostosis and paediatric neurosurgery in LMICs
The advancement of neurosurgical care, particularly within the realm of craniosynostosis, relies upon the dynamic intersection of academic research and clinical execution. This synergy is vital not just for enhancing patient prognosis but also for improving the overall quality of life for those affected by this complex condition. Existing research literature makes it abundantly clear that there is a conspicuous paucity of scholarly data and clinical narratives concerning craniosynostosis and its related surgical interventions in many LMICs,21,30 with this under-representation of LMICs leading to a discourse on understanding craniosynostosis care.
The optimal process of recording academic achievements for the betterment of patient care, particularly its potential assimilation within LMICs, is met with considerable challenges. These hurdles mainly include the stark variation in symptom manifestation and the type of craniosynostosis under investigation, a limited understanding of prognosis prediction based on clinical variables, and a lack of extensive studies involving larger cohorts of patient interventions.21,30
Furthermore, the research landscape in LMICs is frequently hampered by financial constraints. The stark reality of financial constraints inside diverse healthcare systems severely impedes the progress of critical research undertakings. 30 This financial insecurity adds to the widening knowledge gap about craniosynostosis treatment options and outcomes.
This review also highlights the considerable scarcity of information on craniosynostosis neurosurgical management outcomes in most LMIC settings, particularly Sub-Saharan Africa. This massive research gap is a substantial impediment to a full global understanding and study of craniosynostosis surgical procedures. A lack of region-specific data and insights hinders successful plans and treatments since it does not account for the local results, problems, and demography. As a result, it underlines the significance of academic research and clinical documentation from all geographic regions in achieving a high level of understanding in the field of craniosynostosis surgical care from a global perspective.
Improving paediatric neurosurgery capacity for effective craniosynostosis management in LMICs: Efforts made and future prospects
Strengthening specialised healthcare infrastructure and diagnostic capabilities
In LMICs, the surgical management of craniosynostosis can make significant augmentations through the development of well-equipped, specialised neurosurgical infrastructure. The need for specialised tools and technologies can be overcome through international collaborations, governmental backing, and concentrated investments. Strategies such as the World Federation of Neurosurgical Societies (WFNS) initiative, which has been a cornerstone in improving the quality and variety of neurosurgical undertakings in LMICs through specialised equipment donation, 49 can be undertaken to enable LMICs to acquire essential neurosurgical instruments tailored for paediatric neurosurgical care.
Furthermore, private healthcare initiatives tailored to enhance neurosurgical care as well as global paediatric neurosurgical care in LMICs through strengthening surgical infrastructure for the purposes of more effective and efficient craniosynostosis care hold great promise. Initiatives in other fields have seen great success, as in Indonesia, where it supported the expansion of neurosurgery centres from one to across 40 islands, thus providing a large scope for care and practice. 50 The same paradigm in Pakistan has led to the investments made by Alliance Healthcare to bolster regional infrastructure for neurosurgical care. 50
Electronic Health Record (EHR) systems, now ubiquitously deployed across global healthcare facilities, have been empirically shown to augment patient care quality through standardising medical documentation and enhancing inter-team communication, thereby reducing medical errors. These systems also confer institutional benefits, such as integrating patients’ protected health information, reducing expenses, and facilitating research in the surgical management of craniosynostosis. 51 In Dhaka, Bangladesh, for example, implementing a robust EHR system exemplifies transformative impacts on paediatric neurosurgery, with marked improvements in patient tracking, hospital discharge procedures, and outpatient follow-ups. 52 The consolidated patient record provided by the Electronic Medical Record system, linking disparate visit data, underpins this efficiency, underscoring its role in streamlining patient care, including within paediatric populations. Furthermore, the prospects for international collaboration, as evidenced by Smile Train’s development and distribution of the specialised EHR system called Smile Train Express (STX) to partner institutions in LMICs, 39 illuminates a pathway for innovation and strategic collaboration, offering promising avenues for refining craniosynostosis diagnostic and therapeutic strategies, especially in regions with limited resources.
In addition, harnessing the power of telemedicine emerges as a potent strategy for diminishing geographical barriers. By facilitating remote consultations, diagnostics, and post-operative care, telemedicine not only extends the reach of specialised neurosurgical guidance but also reduces the need for patients to undertake arduous journeys for crucial medical attention. 53 Particularly, parents of children undergoing craniosynostosis demonstrated high satisfaction with the standard of care on virtual follow-up. 54
Finally, LMICS embracing novel technological advancements for neurosurgery practice could improve the treatment outcomes of craniosynostosis. For instance, the integration of three-dimensional computed tomography imaging technologies (3D CT) has made significant progress towards addressing the challenges related to craniosynostosis. 3D CT scans offer a revolutionary approach to diagnostic evaluation and treatment planning in the management of craniosynostosis. 55 A full and detailed view of the cranial anatomy can be obtained by a 3D CT scan, allowing precise evaluation of abnormal sutures and skull shape anomalies as well as their association with craniofacial features. This detailed three-dimensional view guides practitioners in the development of individual treatment strategies as it helps to accurately identify a specific type of craniosynostosis. 55
Training and maintaining neurosurgeons and other specialised multidisciplinary teams
In LMICs, nurturing a proficient cohort of paediatric neurosurgeons emerges as a challenge that hinges on allocating substantial educational investments. This imperative is a matter of medical education and a testament to the broader commitment to improving healthcare access and quality within these resource-constrained settings. 56 The journey towards achieving this ambitious goal gains substantial traction through concerted and collaborative initiatives spearheaded by national and regional organisations. A pivotal component of this advancement is the collaboration between LMICs and established medical institutions. This partnership fosters knowledge exchange, mentorship, telemedicine, and research, allowing LMICs to harness the expertise of established institutions and bridge the gap in paediatric neurosurgery proficiency. This collaborative spirit serves as the foundation for a continuous learning trajectory among professionals in the field.
Central to the effectiveness of these initiatives is the establishment of stringent benchmarks that span training and certification. The collaborative efforts encompass the development of educational frameworks that cater to the specific needs of LMICs, acknowledging the unique challenges and opportunities that arise within their healthcare ecosystems. Continuing Medical Education initiatives, including seminars and workshops, play a pivotal role in sustaining expertise progression. 57 These proactive educational avenues ensure practitioners remain updated on the latest advancements, refining their skill set to deliver optimal paediatric neurosurgical care. 57 A pivotal example of such dedication to raising the bar of paediatric neurosurgical care is evident through the American Board of Medical Specialties and its pioneering initiative, the American Board Of Neurological Surgery Maintenance of Certification (ABNS MOC) programme. 58 This programme epitomises the unwavering commitment of diplomates affiliated with the ABNS towards the pursuit of excellence within the intricate realm of neurosurgical practice 58 The ABNS MOC programme’s impact reverberates globally, resonating particularly strongly within LMICs.
Furthermore, some sub-Saharan African nations’ strategies offer insight into bolstering paediatric neurosurgery. 59 An example of such a collaboration is CURE hospital in Uganda, having an international collaboration with American-based neurosurgeons dedicated to addressing the neurosurgical needs of East African children. The hospital also serves as a very resourceful teaching centre for African surgeons through these international collaborations. Additionally, the Neurosurgery Education and Development programme aims to teach endoscopic techniques for treating hydrocephalus and establish neurosurgery as a specialty in Kenya and Zanzibar. 60
Also, local neurosurgical training programmes, such as the one in Yogyakarta, Indonesia, addresses craniosynostosis care disparities by emphasising microsurgical techniques and simulations. 61 These programmes demonstrate the importance of cross-border collaboration and specialised training efforts in strengthening paediatric neurosurgery practices. Dedicated neurosurgical labs with advanced tools and virtual reality simulators help to refine skills.62,63 Local research and innovation are simultaneously reshaping LMIC paediatric neurosurgery. 42 Collaborations between researchers, engineers, and healthcare experts result in tailored solutions that improve healthcare and strengthen practices in LMICs. Indigenous expertise converges to create customised interventions that take into account regional nuances. This comprehensive strategy integrates education, innovation, and collaboration to address LMIC healthcare challenges holistically. These fantastic collaborations can be widely adopted by other LMICs to improve paediatric neurosurgical care.
Improving funding and providing equitable access to neurosurgical care
Advancing funding and equitable access to craniosynostosis care represents a central imperative in the comprehensive and effective treatment within the healthcare systems of LMICs. The complexity of craniosynostosis requires an innovative approach to funding and resource distribution. These can be achieved through leveraging transformative models such as public–private partnerships and synergistic philanthropic collaborations; healthcare systems can infuse essential resources into the treatment framework. 64 Such a model can prove beneficial if specifically tailored to craniosynostosis care, as more than a mere financial contribution, these strategies can support the unification of diverse expertise, thereby addressing the existing funding gaps while fostering optimal resource allocation. 64
Additionally, investing in human capital through comprehensive training programmes is another strategy that could positively impact craniosynostosis care by promoting equitable access. Initiatives of this kind nurture a locally skilled workforce, cultivating expertise and reducing the dependency on external support for complex cases. 57 Furthermore, innovative approaches such as mobile neurosurgical units for craniosynostosis care can prove to be indispensable in extending care to remote and underserved areas, as similar units are with essential surgical facilities while acting as a nimble and responsive platform, catering to urgent surgical interventions and emergency care needs. 65 By adopting a roving presence in underserved regions, mobile neurosurgical units for craniosynostosis care can proactively mitigate access challenges and bring critically needed services closer to communities.
The variable outcomes observed in terms of mortality and surgical efficacy in LMICs highlight the existing disparities in healthcare access for patients. While certain studies report no mortality and limited complications,14–27 others indicate fatalities and persistent complications and symptoms.31,33 This underscores the imperative for global collaborations grounded in knowledge sharing and expertise exchange to strive for more equitable craniosynostosis care. HICs, equipped with advanced practices and cutting-edge technology, can play a pivotal role in supporting developing nations by sharing best practices, facilitating training opportunities, and even donating essential medical equipment. 66 Moreover, LMICs facing higher mortality and complication rates can benefit from learning from those with no mortality and limited complications. This knowledge exchange presents a valuable opportunity for LMICs to understand how their counterparts effectively utilise limited resources to achieve better outcomes for patients. These partnerships not only enhance the technical capabilities of local healthcare practitioners but also stimulate collaborative research initiatives that drive innovation, potentially leading to breakthroughs in neurosurgical techniques for craniosynostosis care in LMICs.
Introducing and adapting policies to strengthen paediatric neurosurgical care in LMICs
Providing quality paediatric neurosurgical care in LMICs remains a challenge. Establishing and implementing policies to strengthen care are essential to bridging this gap.
In order to develop effective policies, a thorough evaluation of the existing landscape, identification of key areas of focus, and tailoring of strategies to address specific challenges are needed. For instance, the Disease Control Priorities, Third Edition (DCP-3), is an initiative that offers evidence-based recommendations for resource allocation to achieve optimal health outcomes. In the field of paediatric neurosurgery, the DCP-3 initiative’s significance revolves around providing evidence-based recommendations for impactful and efficient neurosurgical interventions. By following these recommendations, policymakers can optimise resource allocation while addressing the specific needs of patients.66-68
Additionally, the National Surgical, Obstetrics, and Anaesthesia Plans (NSOAPs) play an imperative role in enhancing surgical and anaesthesia infrastructure.45,69 The shortage of essential neurosurgical equipment, such as drills, microscopes, and microinstruments, can be lessened by prioritising the provision of these tools through NSOAPs. Furthermore, solutions for the maintenance and sterilisation challenges of these essential infrastructures can also be achieved by following NSOAPs. NSOAPs also foster multidisciplinary collaboration by involving various specialists, including paediatric reconstructive surgeons, surgical nurses, and radiologists, in the surgical workforce. This approach aligns well with the requirements of paediatric neurosurgical care, where patient management heavily relies on a multidisciplinary team of experts for comprehensive care.45,70
Moreover, it is of utmost importance to foster collaborations between international organisations like the WFNS and the World Health Organisation, non-governmental organisations, and academic institutions. These collaborations play a crucial role in terms of shaping the policies with regards to knowledge exchange, capacity building, and resource mobilisation.68,70 By incorporating the shared best practices into specific local plans and guidelines, LMICs could benefit from significant upskilling of existing neurosurgeons and enhanced overall quality of care.
LMICs are encouraged to learn and adopt from the Organisation of Provincial Neurosurgery Ontario (PNO), where a multi-stakeholder partnership was established to improve access and delivery of neurosurgical services. 71 PNO worked on establishing guidelines for patient transfer among national hospitals as well as out-of-country patient transfers, formed neurosurgical disease subgroups, and established a tele-radiology system called Emergency Neurosurgery Image Transfer System where patients’ radiological imaging is uploaded to a central server and made accessible for neurosurgeons and hospitals all over the country. 71 Moreover, funding and logistical initiatives were established, aiding in lowering the cost of care. 71
The findings of this review underscore the challenges associated with craniosynostosis management in LMICs, revealing a notable incidence of reoperations and persistent complications attributed to the intricate nature of the condition.14,17,21,22,30 Consequently, future research endeavours should prioritise investigating the underlying causes for these reoperations and persistent complications.15,31 Conducting meaningful research in this domain is crucial, as it serves as a foundational step in providing valuable insights for policymakers and clinical governance. This, in turn, can inform strategic interventions aimed at enhancing surgical techniques, refining pre-operative planning processes, and tailoring specialised aftercare initiatives. Policymakers are encouraged to consider implementing guidelines that emphasise the significance of continuous monitoring, adaptable treatment regimens, and effective management of unforeseen complications to optimise craniosynostosis care in LMICs.
Lastly, a strong monitoring and assessment mechanism is crucial for the effectiveness of policy implementation. The regular assessments provide policymakers with the opportunity to assess the impact of interventions as well as identify areas for improvement and adjustments. Countries are able to ensure the successful implementation of policies with a view to increasing access to care, improving performance, and narrowing inequalities by measuring results against established benchmarks. 70 A summary of the future prospects of improving paediatric neurosurgical care has been illustrated in Figure 4.

A summary of the future prospects for enhancing paediatric neurosurgery care to effectively manage craniosynostosis.
Limitations of the study
Several limitations should be acknowledged in this review. To begin with, the literature survey was confined to a specific set of prominent databases, including PubMed, EMBASE, Google Scholar, the Cochrane Library and Scopus. A focus on these major databases could introduce a risk of omission, as relevant research from alternative sources could be inadvertently overlooked. Furthermore, the decision to exclude non-English publications may contribute to a language bias in the analysis. This exclusion criterion potentially overlooks significant works and insights published in languages other than English, thereby introducing the risk of missing essential information. Such a bias may ultimately limit the comprehensiveness and generalisability of the review’s conclusions.
Additionally, a heavy emphasis was placed on research pertaining exclusively to neurosurgery. This could consequently lead to vital information being overlooked in studies recording findings from a mixture of surgical specialties. These limitations are further compounded by the absence of literature from Sub-Saharan Africa, resulting in a decrease in the effectiveness of this review in providing a global understanding regarding the study of surgical procedures for craniosynostosis.
Conclusion
Craniosynostosis presents distinct challenges in LMICs. Examining the neurosurgical outcomes of this condition is crucial for comprehending the dynamic landscape of the disease’s management in LMICs. In an environment where healthcare resources might be limited, the management of craniosynostosis requires a delicate balance of innovative surgical techniques, vigilant postoperative care, and comprehensive risk assessment. Recent studies offer promising insights into both positive and negative outcomes of various surgical interventions applied in LMICs. On the positive side, advancements in surgical procedures have led to successful corrections, minimal complications, and enduring efficacy of the treatments, enhancing patient well-being. Yet, these achievements are not without their complexities and setbacks. Instances of complications, mortality, the need for reoperations, and persistent symptoms are reminders of the intricate nature of this condition and the imperative to continually strive for optimization in patient care.
Footnotes
Acknowledgements
We acknowledge Sharanya Kaushik, MBBS, for helping with figure illustrations of our manuscript. We also acknowledge Icormed Research Collaborative for the facilitation of this project.
Author contributions
Wireko Andrew Awuah, Arjun Ahluwalia, Syed Hasham Ali and Muhammad Hamza Shah: Conceptualisation, Data curation, Formal analysis. Writing – original draft, Writing – review and editing. All Authors: Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review and editing. Saibaba Guggilapu, Tomas Ferreira and Sumitaksha Banerjee: Visualisation. All Authors: Approval of final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable.
Informed consent
Not applicable.
Data availability statement
No data available.