
Abstract
Introduction:
We aimed to compare clinical features of older age group and young and middle-aged patients with COVID-19 and analyze mortality predictors.
Methods:
Retrospective analysis of ongoing collection of prespecified data, on a single institution, including patients hospitalized consecutively due to COVID-19 infection, from March to June 2020.
Results:
Of 195 patients, 56.9% were ⩾65 years (older age group). Older age group had multimorbidity (p < 0.001). At admission Early Warning Score-2 (p < 0.001), C-reactive protein, D-dimer, creatinine, anemia and lymphopenia were higher in older age group, as well as median time of hospitalization (14 vs 10 days, p = 0.004). Complications were more common in older age group, but there were no significant differences in admission to intensive care. There were 18 deaths, 16 in older age group. Modified Early Warning Score at admission (odds ratio = 1.60, 95% confidence interval = 1.07–1.37, p = 0.021) and C-reactive protein >5 mg/dL (odds ratio = 2.12, 95% confidence interval = 1.13–26.26, p = 0.034) were independent predictors of inhospital mortality in older age group but not in young and middle-aged.
Conclusion:
Older age group was at higher risk for complications and inhospital mortality. Identification of specific scores of severity for this population is essential to ensure that best care is provided.
Introduction
COVID-19 is a respiratory disease caused by a newly discovered coronavirus, SARS-CoV-2 virus, identified in the city of Wuhan, Hubei Province, China, in December 2019. World Health Organization (WHO) declared the official name as COVID-19 in February 2020. On 11 March 2020, WHO announced the disease as a pandemic, based on its spread to 118,000 cases in 114 countries. 1 In line with the WHO COVID-19 dashboard globally, at 23 June 2020, 8,993,659 confirmed cases of COVID-19, including 469,587 deaths, were reported. At the same time in Portugal, according to Portuguese General Health Directorate (DGS), there were 39,737 confirmed cases of COVID-19, 12,093 in 60-year old people or elder. There were 1540 deaths in Portugal due to this disease, 95.5% (1471) in 60 years old patients or older. 2
This virus can lead to the appearance of respiratory tract infections in the patients ranging from mild to fatal illnesses as pneumonia and acute respiratory distress syndrome (ARDS).3,4 The majority of patients will develop mild to moderate respiratory illness and recover with supportive treatment, with no special care requirements. 1 Nonetheless, patients with comorbidities like diabetes, cardiovascular disease, renal insufficiency, chronic respiratory disorders, cancer, immunodeficiency and other chronic disorders will be more prone to develop serious pathological issues related to COVID-19. 1
Geriatric patients are reported to be more vulnerable to severe illness and thus being admitted to the intensive care unit (ICU), the mortality of these patients is higher. The purpose of this study was to compare the clinical features of older age group (OAG) and young and middle-aged (YMA) patients with COVID-19 and identify mortality predictors in our Portuguese population.
Patients and methods
Study population
All adults consecutively admitted to the internal medicine ward and infectious diseases ward of a central tertiary hospital, between 13 March 2020 and 15 June 2020 were analyzed. Participants were eligible for enrollment if they were aged 18 years or older and had a positive real-time fluorescent reverse transcription polymerase chain reaction (RT-PCR) for SARS-CoV-2 of nasopharyngeal or oropharyngeal swab specimens obtained during their hospitalizations. Patients were excluded if there was lack of recorded medical data. Written informed consent was obtained from all subjects or their legally authorized representatives, prior to study initiation.
Study design
This was an observational, descriptive, retrospective analysis of ongoing collection of prespecified data, performed in a single institution. From medical files, demographic and clinical data were extracted which included age, gender, ethnic group and previous known comorbidities. Patients were organized in two cohorts, based on age: OAG (⩾65 years) and YMA group (<65 years old). A subgroup was also specifically analyzed among the OAG, typically addressed as the elder population (⩾80 years). After reviewing the existing literature,5–7 we have calculated that a total sample of 116 patients would provide 90% power to detect a 30% difference of severity between the two cohorts, with a two-sided log-rank test at an alpha level of 0.05.
Clinical presentation features of SARS-CoV-2 infection were also collected as well as serum levels of C-reactive protein (CRP), hemoglobin, platelets, absolute count of leucocytes, neutrophils and lymphocytes, D-dimer, hypersensitive cardiac troponin I (hs-cTnI) creatinine and ferritin at presentation. Cut-off values were defined based on previously published data from large cohorts.8–10
Severity scores were analyzed. Due to timely changes of internal protocols, Modified Early Warning Score (MEWS) 11 was gradually replaced by the National Early Warning Score 2 (NEWS 2),12,13 which adds to MEWS parameters (respiratory rate, temperature, systolic blood pressure, consciousness and heart rate) supplemental oxygen and hypercapnic respiratory failure.
We have also collected data regarding exposure to hydroxychloroquine as well as anti-viral lopinavir/ritonavir (LPV/r). Patients who developed complications from SARS-CoV-2 infection and specifically the need for oxygen therapy, antibiotics or dialysis during hospitalization were assessed, as well as admission in ICU. Death by any cause during hospitalization was also analyzed.
Statistical analysis
Analysis of normality was undertaken using the Shapiro–Wilk test. Data analysis was performed to compare the study groups, with the Mann–Whitney Wilcoxon test used for continuous variables and the χ 2 test of independence for categorical variables. Pearson’s correlation was used for weight assessments. Logistic regression models were performed to study the effect of explanatory variables on outcome, with a stepwise approach for multivariate analysis. For each variable, the adjusted odds ratio (OR) and 95% confidence interval (CI) were calculated using maximum likelihood estimation. All analyses were performed using the Stata 15.1 software (StataCorp LLC). A p-value less than 0.05 was considered statistically significant.
Results
There were 195 patients hospitalized with COVID-19 confirmed infection. The demographic and clinical characteristics of the population studied are shown in Table 1. Table 2 presents initial laboratory findings, severity scores and hospitalization recorded variables, according to age groups.
Baseline demographic and disease characteristics, according to age groups.
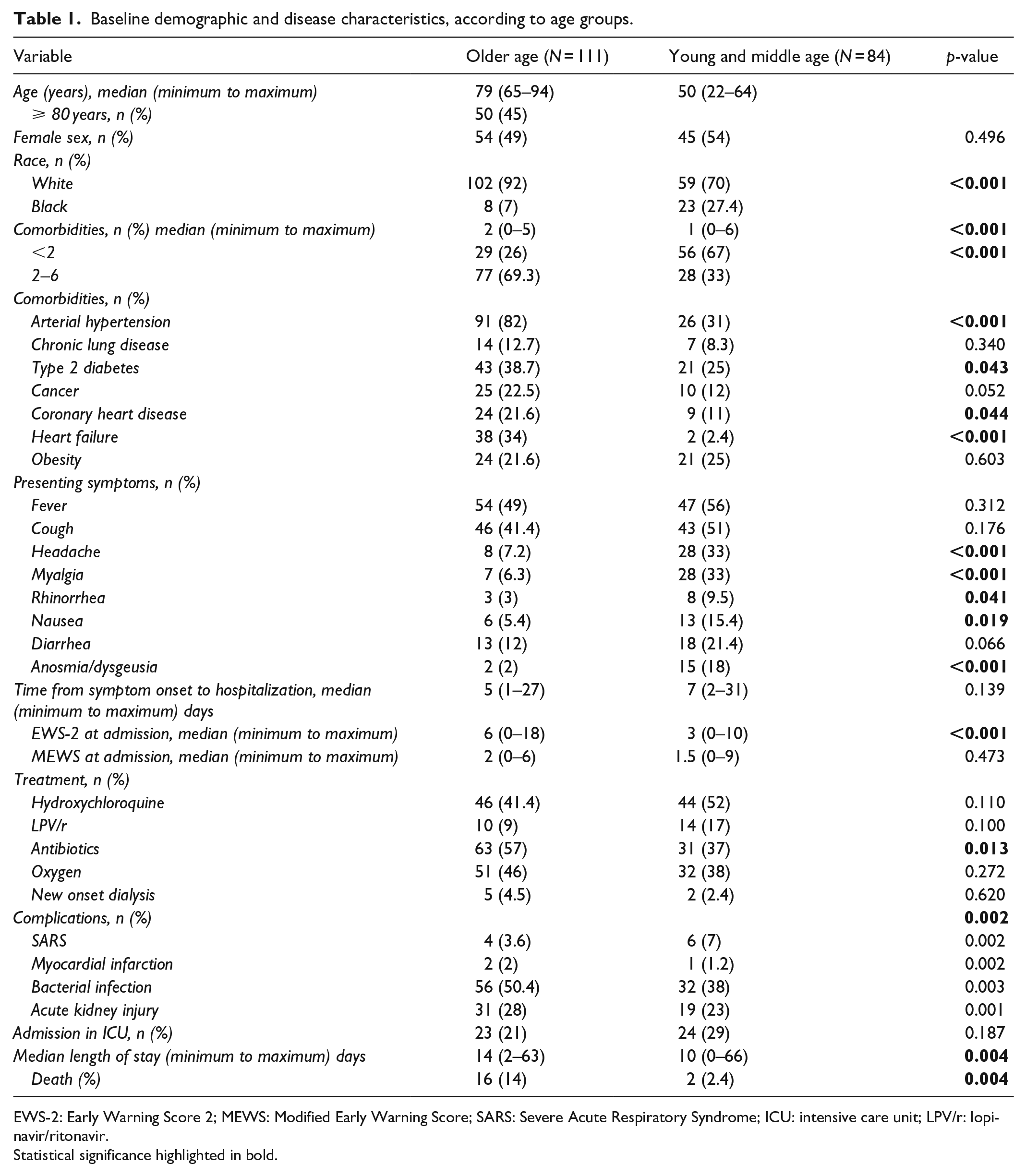
EWS-2: Early Warning Score 2; MEWS: Modified Early Warning Score; SARS: Severe Acute Respiratory Syndrome; ICU: intensive care unit; LPV/r: lopinavir/ritonavir.
Statistical significance highlighted in bold.
Laboratory findings of hospitalized patients due to COVID-19, at admission, according to age groups.

Statistical significance highlighted in bold.
In the analyzed population, 111 (56.9%) patients had ⩾65 years (OAG) of which 45% had ⩾80 years; 84 (43.1%) were YMA. Overall, OAG had significantly more multimorbidity, specifically arterial hypertension, type 2 diabetes, heart failure and coronary heart disease (p < 0.001). Regarding presenting symptoms of COVID-19 infection, OAG more typically presented with common symptoms, like cough and fever, when compared with YMA, that more often presented with headache, myalgias, rhinorrhea, nausea and anosmia/dysgeusia (p < 0.001).
Outcomes, univariate and multivariate analysis for mortality predictors
During hospitalization, there were 18 deaths (mortality rate 9.2%), 16 in OAG, 13 of which (81%) among very old population versus two deaths in the YMA group (p = 0.004).
Regarding potential prognostic biomarkers and scores, MEWS was calculated in 186 patients while EWS-2 in 176 patients. EWS-2 at admission was significantly higher in the OAG (p < 0.001). Univariate analysis also showed higher baseline CRP, D-dimer and creatinine as well as more pronounced anemia and lymphopenia in this group. Length of stay was significantly higher in OAG (14 vs 10 days, p = 0.004). Complications were more common in OAG, specifically bacterial infection and acute kidney injury. There were no significant differences in admission to ICU according to age groups.
To assess predictors of inhospital death, a multivariate model was built with variables obtained from univariate analysis. MEWS at admission (OR = 1.60, 95% CI = 1.07–1.37, p = 0.021) as well as a baseline CRP above 5 mg/dL (OR = 2.12, 95% CI = 1.13–26.26, p = 0.034) were independent predictors of death in OAG but not among YMA group (Table 3).
Multivariate logistic regression for death during hospitalization.

MEWS: Modified Early Warning Score; CRP: C-reactive protein; hs-cTnI: highly sensitive cardiac troponin I.
Statistical significance highlighted in bold.
Discussion
Our results reflect the heterogeneity between the two study cohorts, with significant differences on comorbidities, symptom presentation, complications, laboratory findings and prognosis, according to age.
The OAG had more comorbidities, especially hypertension, diabetes, coronary heart disease and heart failure, when compared with YMA group, reflecting the disease burden associated with age, which confers to this group a higher frailty, decreased organ function and susceptibility to complications, including severe illness and death.14–16
Two studies, one of 1099 and another of 4021 patients with confirmed COVID-19 found the mortality rate of patients aged 60 years and over is significantly higher than that of patients under 60 years.15–17 Our results on mortality are on line with these authors, confirming significant higher mortality in OAG. However, the great majority of deaths occurred in patients over 80 years (72% of deaths).
According to WHO, most developed world countries have accepted the chronological age of 65 years as a definition of “elderly” or older person. However, there is no general agreement on the age at which a person becomes old and this cut-off is many times associated with the age at which a person can begin to receive pension benefits. In this study, we used the cut-off of 65 years old to define the older age population. In our country, the increasing life expectancy (80.9 years in 2018) 18 has led to very positive consequences for health and the well-being of older people making the majority of people aged 65 hardly consider themselves old.
Thus, it is important to emphasize that, although, and as expected, mortality was higher among the OAG,19,20 the major slice of these events happened among the eldest population (+80 years). Our results indeed, and as previously suggested,21,22 prompt us to argue for the incorporation of systematic comorbidity assessment in routine evaluation of older adults hospitalized due to COVID-19 infection. 23 Undeniably, in the geriatric setting, it is becoming evident that the accrual of biologic dysfunctions in multiple organ systems deeply affects the health status of this population. Indeed, aging is associated with increased vulnerability to chronic health problems, which tend to accumulate and increase the complexity of and elder person’s health condition and well-being.24,25
Reducing mortality of critically ill patients with COVID-19 depends on early medical intervention, which requires emergency clinicians to quickly select degrees of severity among a large number of patients. The Modified Early Warning Score (MEWS), although still needing accuracy improvement, has an acceptable prognostic value for application in the emergency department.13,26 In our data, MEWS at admission proved to be an independent predictor of mortality, when adjusting for possible confounders, supporting its use in baseline assessment of severity of OAG patients. Interesting, MEWS performed better than EWS-2 in terms of predicting prognosis, although no direct comparison of the 2 scores has, to our knowledge, been already performed in the literature.
Other possible predictor of severity in patients with COVID-19 is CRP. One study evaluated 209 adult patients with confirmed COVID-19, diagnosed as non-severe and compared clinical characteristics of aggravated patients with those that remained non-severe, and analyzed the possible factors associated with progression. The authors demonstrated the prognostic value of CRP in the progression of mild COVID-19 patients. 8 Also, in our multivariate analysis of prognostic biomarkers for OAG patients, CRP >5 mg/dL proved to accurately and independently predict mortality among this group, which has already been stated as a risk factor, with applicability among the older age population.27,28
Together, these data support the discussion for the definition of a combined score of severity for the older age population, to be used as a prognostic tool. The establishment of such instrument would be crucial to better, and in due course, define adequate interventions and individualized approaches, in a population where frailty, comorbidities and thus potential complications can lead not only to higher mortality, but also to higher disability, with obvious consequences for health, health systems, workforces and their funds.
Limitations of this study include its retrospective design, and thus all limitations related to retrospective studies. Single-center study is also a limitation. Collection of clinical data from medical records limits the access to certain information and can question the accuracy of the information. Also, although several comorbidities were extensively collected and included in the statistical analysis, additional relevant past diagnosis and medication were not included and the authors recognize that some could affect the study outcomes. Finally, the short follow-up of these patients might be a limitation to our findings, potentially underestimating mortality. A longer follow-up will also allow for analyses of other relevant outcomes, particularly in this population, as disability and need for transfer to non-acute care facilities.
Conclusion
To our knowledge, this is the first comprehensive descriptive study in hospitalized Portuguese patients with COVID-19 infection, aimed at specifically addressing age-dependent risk factors and prognostic biomarkers, specifically in the older age population. Older age does not imply dependence but vulnerability should be taken in account when defining strategies to deliver person-centered approached to older populations and their more complex needs, in the time of COVID-19’s outbreak.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Ethics Committee and Hospital Administration Board, and complies with all national and international standards for research practice and reporting. It was conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects or their legally authorized representatives, prior to study initiation.