
Abstract
Objective:
The present research evaluated and compared effectiveness between nitrofurantoin and double antibiotic paste in alleviating post-operative pain in patients suffering from symptomatic irreversible pulpitis.
Methods:
There were 60 subjects enrolled who were allotted among three groups: Group 1 – Nitrofurantoin, Group 2 – double antibiotic paste, and Group 3 – Control. Succeeding access opening and chemo mechanical preparation, intracanal medicament was placed in the root canals. Using a numerical pain scale, pain scores were measured at the following time intervals: preoperative, 12, 24, 48, and 72 h. One-way ANOVA and post hoc statistical analysis were conducted, with a p-value of ⩽ considered as statistically significant.
Results:
Preoperatively, most patients experienced moderate to severe pain. The patients in groups 1 and 2 reported considerable reduction in their pain scores (p ⩽ 0.001) on each time interval. However, patients in group 3 experienced a higher level of pain even at 72 h. No considerable distinction was found among participant’s pain scores of groups 1 and 2 (p = 0.193).
Conclusion:
For effective pain-relieving, both nitrofurantoin and double antibiotic paste can be successfully used in patients suffering from symptomatic irreversible pulpitis. However, when calcium hydroxide was used, patients experience high levels of pain.
Introduction
Symptomatic irreversible pulpitis is one of the most commonly encountered dental pathologies, which is associated with various causes, the commonest amongst which is dental caries. 1 Dental caries is a bacterial disease that initially does not involve the pulp. However, if left untreated, it may involve the pulp leading to symptomatic periapical periodontitis. Patients who suffer from this pathology report symptoms such as severe and radiating pain toward the head, jaws, and neck with pain increased on biting and increased pain sensation whilst sleeping. 2 To treat this disease, the most commonly selected endodontic treatment by dentists is root canal therapy (also called pulpectomy). The primary goal of pulpectomy is extirpation of the infected pulpal tissue, followed by cleaning with shaping canals, and finally obturating the canals with inert filling material and sealing it off. 3
At times it has been suggested that canals prepared by chemo mechanical preparation is alone not completely efficient in removing microorganisms which are primarily responsible for the pathology. 4 Incomplete removal of the microorganisms increases the chances of occurrence of post-treatment disease which is characterized by the failed primary treatment of the tooth which further hampers the prognosis of the affected tooth. 5 Different studies suggest the primary cause of pain after initial treatment is the failure of proper disinfection of the canals.6,7 Calcium hydroxide, which is currently asserted as the gold standard, is among commonly utilized intracanal dressing agents. 8 A wide range of antibacterial properties are offered by Calcium hydroxide against the most habitual culprits of endodontic and periapical pathologies such as Enterococcus faecalis (E. faecalis). 9 A recent systematic review has reported that calcium hydroxide has been effective in the reduction of postoperative pain as compared to using no intracanal medicament. 10 However, in terms of eradicating E. faecalis, calcium hydroxide has limited effectiveness against E. faecalis, which is listed as the most common bacteria found in endodontic lesions and in retreatment cases. 11 Therefore, other intracanal medicaments have been studied to overcome such limitations.
A combination of different antibiotics has been studied to increase the scope of antibacterial coverage. One of the most commonly used combination antibiotics is double antibiotic paste (DAP). DAP is an intracanal medicament that is a combination of metronidazole and ciprofloxacin. DAP is known to be impactful against various microorganisms in the endodontic and periapical regions.12,13 One study has reported that the use of DAP resulted in a greater reduction in postoperative pain scores in patients as compared to calcium hydroxide. 14 Although minocycline has been shown to be effective, tooth discoloration associated with it led to increased use of DAP which shows similar results. 15 Despite the associated benefits of DAP, its use has been shown to result in a decrease in stem cells of apical papilla that can decrease regeneration capabilities. 16 Another intracanal medicament, although less frequently used, is triple antibiotic paste (TAP). TAP consists of metronidazole, ciprofloxacin, and minocycline combination, which has been less preferred now primarily due to its crown discoloration. 17 Therefore, such limitations are overcome by DAP as it not only eradicates endodontic pathogens, it does not discolor the crown. 17
Nitrofurantoin is a synthetic heterocyclic compound that causes the formation of nitrofurans. The effects of nitrofurantoin on E. faecalis have been studied in various studies.18–20 Primarily, nitrofurantoin is equipped to treat urinary tract infections since E. faecalis is one of the prime suspects in such pathologies. 21 Since bacterial resistance is encountered against commonly used penicillins, the use of nitrofurantoin in such cases overcomes the limitation of bacterial resistance. In dentistry, the uses of nitrofurantoin have been studied to a limited extent. One study reports that nitrofurantoin was effective in reducing the pain scores of patients suffering from symptomatic irreversible pulpitis when used as an intracanal medicament. 22 Moreover, positive results have been obtained by eradication of E. faecalis by nitrofurantoin but limitations were found in terms of trans-dentinal movement of the medication. 23 Furthermore, one study experimented with the use of nitrofurantoin for the eradication of E. faecalis with the conclusion of successful results. 24
Currently, very few studies have explored the uses of nitrofurantoin in dentistry with few studies reporting its use as an intracanal medicament.22,24 Literature suggests the presence of bacteria in symptomatic irreversible pulpitis of vital teeth; therefore, we conducted our study on that purpose. 25 Only one study up till now has made the comparison of nitrofurantoin with calcium hydroxide as an intracanal medicament. As nitrofurantoin offers greater coverage against anaerobic bacteria, its application in endodontic lesions can be of benefit. Hence, the present study aimed to evaluate the impact of nitrofurantoin and DAP for mitigating pain experienced by subjects suffering from symptomatic irreversible pulpitis.
Materials and methods
Present clinical trial commenced at Altamash Institute of Dental Medicine, Pakistan at the Department of Operative Dentistry and Endodontics. Upon being granted ethical approval (AIDM/ERC/01/2022/02) from the ethics review committee of the institute according to the conduct of the Declaration of Helsinki, this clinical trial was executed. All participants in the research provided written informed consent. The clinical trial has been registered on the date of 31 October 2022 in the publicly available registry of Clinicaltrials.gov (NCT05600023), with duration from August 2022 to October 2022. We have followed the CONSORT guidelines when preparing the manuscript; Supplemental Table 1. For sample size calculation, we used OpenEpi software with the values used for calculation: confidence interval at 95%, a margin of error at 5, and desired percentile at 50. Calculated sample size was 28 (14 subjects in one group). 26 To follow the eligibility criteria, the non-probability convenience sampling method was utilized. 27
Eligibility criteria
Inclusion criteria
Adults of 18 years and above
Patients falling in Class 1 of the American Society of Anesthesiologists
Body Mass Index (BMI) ranging from 18.5 up to 24.9 (Height: 5–6 feet and weight: 50–70 kg)
Suffering from Symptomatic Irreversible Pulpitis as confirmed by Electric pulp test (response or no response) along with clinical (sensitivity to cold indicated by lingering pain after removal of stimulus) and radiographical examination
Single-rooted teeth (Single canal confirmed based on X-ray with same lingual and opposite buccal (SLOB)technique)
Voluntary participation
Exclusion criteria
Patients below the age of 18 years
BMI less than 18.5 and above 24.9
Patients with systemic diseases
Multi-rooted teeth
Declining participation in the study
Randomization and groups allocation
For the purpose of random distribution of participants in one of three groups, drawing lots method was used. The patients were then allocated to any of the three groups: Group 1 – Nitrofurantoin; Group 2 – DAP; Group 3 – Control group with calcium hydroxide. According to eligibility criteria, the study excluded participants who did not meet the inclusion requirements. Thorough information about nature and purpose of the clinical trial was briefed to participants. Patients’ written consent was collected to ensure that participation was voluntary. For privacy purposes, collected data of the patients were kept confidential throughout the entire duration of the study.
Collection of data
This was a double-blind study, as both the principal investigator and patients were kept blind, as the syringe in which the intracanal medicaments were placed were covered with colored tape. A single dentist administered the treatment to all the patients that were part of this study. Most of the patients who underwent treatment reported their chief complaint as moderate to severe pain. Furthermore, many patients reported pain and sensitivity on intake of hot and cold foods. The teeth of most patients were not tender to percussion; however, pain and discomfort was experienced by palpation. The periapical condition of the teeth was evaluated using periapical X-ray to examine for any periapical radiolucencies if present. Radiographic findings included carious lesions invading the pulp chamber, with periodontal ligament (PDL) widening in some cases. After local anesthesia (Septodent- 2% Lidocaine, epinephrine 1:100,000©), complete isolation was achieved using rubber dam on the tooth under treatment. The carious lesion was removed by the use of a high-speed handpiece, which was followed by gaining access to the pulp chamber (Access Opening). The hand K-files (Mani- K Files©) were utilized for locating the canals, followed by performing pulpectomy to remove infected pulpal tissue. As per the radiograph and apex locator (Eighteeth E-pex Pro Apex Locator©), the working length of the canals was determined and noted. Next, in the same appointment, chemo mechanical preparation was undertaken utilizing crown down technique with conventional manual filing system that includes widening of canal orifices with gates glidden (GG) burs, manual filing from larger to smaller files to remove pulp from coronal to apical direction with no pressure. 3% Sodium hypochlorite solution in a syringe (Tehnodent -Antiseptic Liquid -Sodium Hypochlorite©) was used for irrigation. Next, 17% ethylenediamine tetraacetic acid (EDTA; PD -EDTA 17% Gel©) was used for the removal of the smear layer. Prior to placing the intracanal medicament, canals were dried by paper points (Meta BioMed -Absorbent Paper Points©). Lastly, root canals were filled with intracanal medicament. The confirmation of intracanal medicament reaching the apex was done by delivering into the root canals utilizing a syringe delivery system. Keeping the tip of the syringe 1mm short of the working length, the medicament was delivered into the canal by expressing the medicament until the medicament was seen flowing in the pulp chamber. The patient was dismissed after the placement of a cotton pallet and temporary filling material (3M- Cavit G Temporary Filling Material©) and recalled after 2 weeks for second appointment. The patients were prescribed with Ibuprofen and Acetaminophen in case of severe pain. On the second visit, the temporary filling material was removed along with the cotton pellet, and canals were thoroughly flushed with sodium hypochlorite solution. Now, canal was prepared until F2 preparation as compared to initial F1 preparation for the complete removal of the intracanal medicament.
Preparation of intracanal medicament
The participants assigned in group 1 received nitrofurantoin intracanal medicament. Nitrofurantoin was formulated in powder form, which was then stirred in normal saline to prepare a formulation of 100 mg/ml paste. Now, the paste was placed inside the root canals using Lentilospiral. Patients who were allocated to group 2 were provided with DAP. When preparing DAP, a 1:1 ratio of metronidazole and ciprofloxacin powder was dissolved in normal saline to create a paste. This paste was then placed into the root canals using Lentilospiral.
Measurement of the pain scores
For evaluation of the pain scores of the patients, the time intervals to note the pain was as follows after the first session of treatment: Preoperatively, followed by postoperatively at 12, 24, 48, and 72 h. The pain scores were recorded using a numeric scale, with 0 signifying no pain and 10 representing the most intense pain. 28 The scale was divided into the following categories: According to Figure 1, 0 indicates no pain, 1–3 indicate mild pain, 4–6 indicate moderate pain, and 7–10 indicate severe pain. Patients were instructed for registering their pain ratings on the pain scale at each interval in order to properly record the scores and to bring the scale with them to their subsequent appointment.

Numerical pain scale.
Statistical analysis
SPSS (Statistical Package for Social Sciences) version 25.0 (IBM Company, Chicago, IL, USA) was used to analyze the data. For age, mean and standard deviation values were calculated. ANOVA test was performed to compare the pain scores of the various groups. The post hoc test was applied to further highlight the disparities in the three groups’ pain scores. A p-value of ⩽0.05 was deemed statistically significant.
Results
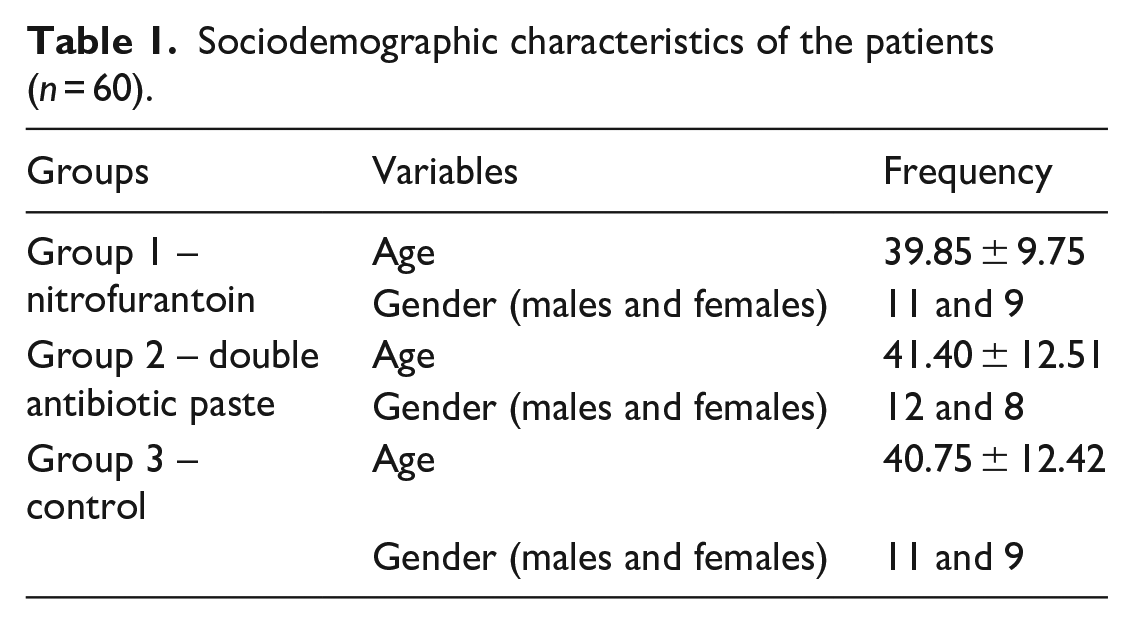
As shown in Figure 2, 60 patients were included in this study. About demographic characteristics, the patients’ mean age in Group 1 – Nitrofurantoin was 39.85 ± 9.75, Group 2 – DAP: 41.40 ± 12.51, and Group 3 – Control: 40.75 ± 12.42. The gender distribution was as follows: Group 1 – Nitrofurantoin: 11 males and 9 females, Group 2 – DAP: 12 males and 8 females, and Group 3 – Control: 11 males and 9 females, illustrated in Table 1.

CONSORT flow diagram of patient selection.
Sociodemographic characteristics of the patients (n = 60).
Following are the patient’s mean postoperative pain scores for each of the 3 groups: Group 1 – Nitrofurantoin: 4.02 ± 0.91, Group 2 – DAP: 3.55 ± 0.55, and Group 3 – Control: 6.21 ± 1.01, as presented in Figure 3. Table 2 represents the pain scores of patients among the three groups at different pre-determined time intervals. There was no statistically significant difference between the groups in terms of preoperative pain values (p = 0.552).

Distribution of mean pain scores of patients among the three groups.
Pain scores at different time intervals among the three groups (n = 60).

For patients belonging to group 1, most of the 17 (85%) patients at 12 h post-operatively had moderate levels of pain with few experiencing severe pain. Furthermore, at 24 h post-operatively, majority of the 14 (70%) patients had moderate levels of pain with few patients experiencing mild pain. Additionally, the majority of the patient’s pain scores dropped to mild level of pain at 48 h. Twelve patients (60%) reported mild pain at 72 h.
For participants belonging to group 2, the majority of the 18 (90%), moderate level of pain scores were reported at 12 h postoperatively. At 24 h, just over half of the patients reported mild pain with the remaining patients reporting moderate pain. Furthermore, at 48 h, almost all of the patients experienced a mild level of pain. Moreover, at 72 h, 70% of the patients were pain-free.
For patients belonging to group 3, majority of the participants reported suffering moderate pain levels, alongside only 2 patients being pain-free at 72 h postoperatively. About the comparison of values of mean pain scores using one-way ANOVA, the three groups showed a statistically significant relationship (p ⩽ 0.001). Additionally, considerable relationship between mean postoperative pain scores of groups 1 and 3 and groups 2 and 3 was found using post hoc analysis (p = 0.001), illustrated in Table 3.
Comparison of pain scores among the three groups.

The mean difference is significant at the 0.05 level.
Discussion
For the treatment of symptomatic irreversible pulpitis, various options are presented to the patient such as root canal treatment and extraction, out of which, root canal treatment is the most preferred. The patient’s reported level of pain to dentist is often severe in nature that requires prompt management to relieve the pain of the patient. Since intracanal medicaments offer superior pain-relieving action as compared to oral antibiotics, they are more beneficial to the patient. 29
Depending on the clinical and radiographic examination, most of the time, the tooth under treatment can be saved by root canal treatment. However, at times prognosis is not favorable for such teeth rendering them unsalvageable, therefore, mandating their extraction. 6 Symptomatic irreversible pulpitis causes excruciating pain; therefore, dentists should counsel the patient regarding how the root canal treatment will subside their pain. Eliminating bacteria from infected root canals is one of the most crucial factors in determining whether root canal treatment is successful. 30 Along with the chemo mechanical preparation, at times it is necessary placing antibiotics within canals for prompt removal of bacteria and alleviation of the pain of the patients. 31
Although calcium hydroxide is considered the gold standard intracanal medicament, different medicaments are frequently used which successfully results in the elimination of the bacteria. There are certain shortcomings to using calcium hydroxide as an intracanal medication, including a higher risk of root fracture, fewer antibacterial capabilities, weak cohesive strength, increased solubility, and marginal leakage.32,33
Traditionally, nitrofurantoin has been used to successfully treat urinary tract infections due to the presence of anaerobic bacteria in the renal tract. 34 The use of nitrofurantoin can be demonstrated to be advantageous for patients since the predominant flora of the infected root canal is composed of anaerobic bacteria. 35 In our study, nitrofurantoin was applied in the root canal of patients with symptomatic irreversible pulpitis. Majority of the patients reported a decrease in their pain scores at different time intervals with over half of the patients being pain-free at 72 h. Abbasi et al. 22 reported a significant relief in pain scores of the patients when nitrofurantoin was used as an intracanal medicament. E. faecalis, has been shown to be successfully eliminated by nitrofurantoin.36,37 Elimination of E. faecalis in infected canal by nitrofurantoin can suggest the relief of pain experienced by the patients. Furthermore, patients who had nitrofurantoin placed into their root canals did not experience any adverse effects upon the use of this medication.
One of the most commonly used intracanal medicaments is DAP. Ciprofloxacin and metronidazole, two antibiotics, are combined to form DAP. DAP offers a wide range of antimicrobial coverage mainly because of the presence of two antibiotics. Patients who were a part of group 2 in this trial received DAP as an intracanal medication. In our study, most of the patients experienced a decrease in their pain scores at different time intervals with the majority being pain-free at 72 h. Such results correspond with different studies in the literature that report significant pain-relieving characteristics of DAP. 38 However, a study by Abouelenien et al. 14 concludes that postoperative pain of patients does reduce regardless of whether intracanal medicament is used or not. These findings suggest that different microflora is present in the endodontic lesions, so the effectiveness of such medicaments does vary from patient to patient. In addition, Deepak et al.’s 39 study states that DAP has been shown to be effective against E. faecalis. Other than the use of DAP in cases of symptomatic irreversible pulpitis, DAP has been frequently recommended for the treatment of external inflammatory root resorption.
Other than the use of DAP and Nitrofurantoin as an intracanal medicament, various other options are available. Minocycline, metronidazole, and ciprofloxacin are three commonly used intracanal medications that are combined to form TAP. Another use of Chlorhexidine is being used as a root canal dressing as it offers antibacterial coverage such as gram-positive and gram-negative bacteria like E. faecalis.40,41 Finally, yet importantly, calcium hydroxide is the most widely used intracanal medication and the gold standard.
Despite the fact that the study’s findings suggest nitrofurantoin can be utilized as an intracanal medication, future clinical trials should further explore the uses and applications of nitrofurantoin in dentistry. Moreover, comparisons should be made with other intracanal medicaments as well as noting any adverse effects associated with its use.
As per the findings of our study, nitrofurantoin along with DAP can be successfully used as an intracanal medicament to treat patients who are suffering from symptomatic irreversible pulpitis. Regarding the strengths of this study, firstly, a reliable pain scale was used to measure the pain scores of the patient, and lastly, a proper record of the follow-up of the patients was kept. First, limited sample size was kept for this clinical trial, which is a restriction. Secondly, the patients might have taken painkillers before visiting the clinic, therefore that may have an impact on their preoperative pain scores values and postoperatively as well. Lastly, the possibility of biases in the study’s participant selection is the final concern.
Currently, very few studies have explored the uses of nitrofurantoin in dentistry with few studies reporting its use as an intracanal medicament. Only one study until now has made the comparison of nitrofurantoin with calcium hydroxide as an intracanal medicament. The currently used root canal medicaments face bacterial resistance to a variable degree; this makes it necessary to explore other medicaments that can be introduced to treat patients. As nitrofurantoin offers greater coverage against anaerobic bacteria, its application in endodontic lesions can be of benefit. Hence, this study evaluated and compared impact of nitrofurantoin and DAP for mitigating pain scores of subjects suffering from symptomatic irreversible pulpitis.
Conclusion
The pain experienced by patients of symptomatic irreversible pulpitis is severe which mandates prompt treatment. The use of intracanal medicaments nitrofurantoin and DAP can be successfully carried out according to the results of the study as it significantly reduces the pain levels of the patients.
Supplemental Material
sj-doc-1-smo-10.1177_20503121231220794 – Supplemental material for The effectiveness of single antibiotic paste nitrofurantoin V/S double antibiotic paste in alleviation of post-operative pain of patients suffering from symptomatic irreversible pulpitis—A randomized controlled trial
Supplemental material, sj-doc-1-smo-10.1177_20503121231220794 for The effectiveness of single antibiotic paste nitrofurantoin V/S double antibiotic paste in alleviation of post-operative pain of patients suffering from symptomatic irreversible pulpitis—A randomized controlled trial by Hira Abbasi, Muhammad Saqib, Afsheen Maqsood, Rizwan Jouhar, Haroon Rashid, Naseer Ahmed, Mohmed Isaqali Karobari and Artak Heboyan in SAGE Open Medicine
Footnotes
Acknowledgements
The authors want to take this opportunity to express their appreciation to the patients who accepted to participate in this study. The authors are grateful to the Research development and review cell of Altamash Institute of Dental Medicine Karachi, Pakistan for guidance and support in this study. The author’s team are also grateful to the Yerevan State Medical University after Mkhitar Heratsi, Yerevan, Armenia, for supporting this project.
Author’s contribution
Conceptualization: HA, NA, and MIK. Methodology: HA and NA. Formal analysis and investigation: HA, MS, AM, RJ, HR, and AH. Writing—original draft preparation: HA, MS, and NA. Writing—review, and editing: AH and MIK. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current investigation are accessible on reasonable request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The research trial was carried out in compliance with the Helsinki Declaration and was authorized by the Ethics Review Committee of Altamash Institute of Dental Medicine (AIDM/ERC/01/2022/02).
Informed consent
All participants in the research provided written informed consent.
Consent for publication
None.
Clinical trail registration
This clinical trial has been registered on the date of 31 October 2022 in the publicly available registry of Clinicaltrials.gov (NCT05600023).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.