
Abstract
Introduction:
Health care workers are at the frontline of the response against the COVID-19 outbreak. Poor preparedness and infection prevention practices among health care workers compound the hazard and occurrence of COVID-19 hospital transmission. Thus, the study aimed to assess preparedness toward COVID-19 pandemics and associated factors among health care workers in Hospitals of Eastern Ethiopia.
Methods:
Facility-based cross-sectional study was conducted from 20 June to July 10 2020. A simple random sampling technique was used to select 423 health care workers. Data were collected using a structured self-administered questionnaire and analyzed using SPSS Version 23. Bivariate and multivariable logistic regression was conducted to identify factors associated with the outcome variable, and statistical significance was declared at a p-value less than 0.05.
Results:
This study revealed that the proportion of health care workers’ preparedness toward the COVID-19 pandemic was 40.9% (95% CI: 36.2–45.9). Working in a public hospital (AOR = 2.7, 95% CI: 1.6–4.3), being unafraid of transmitting COVID-19 to patients (Adjusted odds ratio/AOR = 4.6, 95% CI: 2.2–10.0), feeling safe at the workplace (AOR = 3.3, 95% CI: 1.7–6.4)), satisfied with the infection control policy (AOR = 6.0, 95% CI: 2.3–15.0), and not feeling anxious about the likelihood of COVID-19 spread (AOR = 2.1, 95% CI: 1.3–3.4) were significantly associated with COVID-19 preparedness.
Conclusion:
The majority of the health care workers were not prepared for COVID-19 pandemics. Feeling safe at the workplace scared of transmitting COVID-19 to patients, satisfied with the infection control policy, and feeling anxious concerning the likelihood of COVID-19 were factors associated with health care workers’ preparedness to COVID-19. The current awareness creation training, including motivational and psychological preparation for all health care workers, is mandatory, regardless of their profession or working place.
Introduction
COVID-19 has first emerged as a group of mysterious cases of pneumonia in Wuhan, China1,2 and it was declared as a pandemic disease by World Health Organization (WHO) on 11 March 2020 after it was declared first as a public health emergency disease back in the start of March 2020. 3
COVID-19, which has never been detected previously in humans, is capable of transmitting both from human-to-human and animal-to-human.1–5 Even though the major route of transmission of the COVID-19 is through the respiratory route (sneezing and coughing), it can also be transmitted by touching already infected objects and surfaces, which indicates that the virus can live in many places.3,5,6
The clinical features of COVID-19 range from asymptomatic to symptomatic by showing severe respiratory impairments.7–9 However, the most common symptom of the virus is mainly respiratory, including shortness of breath, cough, and fever,4,6–8,10 and the rare ones include the inability to smell and taste, diarrhea, muscle pain, headache, sore throat, and hemoptysis.9–11
The COVID-19 pandemic has amplified the already existed problem of the world about the economic predicament, morbidity, and mortality.2,12,13 Globally, the last updated, from 3 October 2020, confirmed cases of COVID-19: 34,838,209, deaths: 1,033,356, and recovered: 25,898,926 were reported.2,12
In Ethiopia, the first reported case of COVID-19 was from Addis Ababa on 31 March 2020 and currently there are 289,962 confirmed cases and 4489 deaths from COVID-19 pandemic.14,15 With the predominant upsetting problem of COVID-19, different kinds of measures were taken by countries around the globe to prevent its continuous worldwide spread, including complete lockdown, quarantine service for suspected persons, avoidance of crowding, and closing of transport and education services.16,17
According to the Amnesty analysis, worldwide there were more than 17,000 health care workers (HCWs) have died because of this pandemic. According to Amnesty, as of figures compiled by Friday, at least 3507 HCWs died from COVID-19 in the United States, with the number of 3371 in Mexico, 1143 in Brazil, 1131 in Russia, and 931 in the United Kingdom. Unsafe working conditions and a lack of personal protective equipment (PPE) have been some of the main issues faced by health workers worldwide throughout the pandemic, especially in the early phases. 18
In Ethiopia, the total deaths due to nosocomial infections (NIs) are estimated to account for 691,000 individuals (30%). 12 This study aimed to fill the current information gap by assessing preparedness toward the COVID-19 pandemic and its factors affecting HCWs in Dire Dawa health facilities, Eastern Ethiopia. The questions that we have tried to answer to this study were as follows: To what extent do HCWs have prepared toward COVID-19 pandemics? And which predictors have a significant (major) effect on preparedness among frontline HCWs?
The findings from this study will be expected to provide manifold benefits to HCWs through awareness creation stressing on the consistent use of PPEs, how to protect them from other factors that contribute to a risk of getting a disease (nCov-19). As this study is the first in Dire Dawa Administration, eastern part of Ethiopia that tried to identify the associated factors toward COVID-19 preparedness, by revealing major threats felt out by HCWs and availing such pertinent data, will be used by the government in its effort by designing cope up mechanisms to be delivered as means of encouragement for HCWs prevention and control of COVID-19 in the study area.
This study will have paramount importance to Dire Dawa Regional Health Bureau for better management of frontline HCWs, now and for the future. It will be used as a baseline to further research areas untouched.
Methods and materials
Study area and period
The study was conducted in Dire Dawa administration hospitals from 20 June 2020 to 10 July 2020. Dire Dawa is found 515 km east of Addis Ababa, the capital city of Ethiopia. According to 2020, population projection, Dire Dawa has a total population of 466,000 of which females account for 51.6%. There are 9 urban and 38 rural kebeles. There are 2 public hospitals, 15 health centers (HCs), 16 private clinics, and 4 private hospitals. As of October 2020, the Dire Dawa Regional Laboratory has performed the COVID-19 test for a total of 22,110 suspected cases, of these 2133 were confirmed cases, 70 active cases were found, 28 death recorded, and 2063 were recovered including HCWs.
Study design and populations
A facility-based cross-sectional study was employed among HCWs working in Dire Dawa Hospitals. All health professionals working at public and private health institutions in Dire Dawa city during the data collection period were included in the study while part-time health professional workers were excluded.
Sample size determination and sampling procedure
The sample size was determined using a single population proportion formula (Zα/2)2 pq/d2 based on the following assumptions: 95% confidence level, P (50%) proportion of preparedness as there is no previous study conducted, 5% of margin of error; and adding 10% for non-response rate gives the final sample size of 423.
The two public and four private hospitals were selected purposively. The study participants were then allocated to the six hospitals proportionally according to their number of health care professionals (Figure 1). The study subjects were selected using a simple random sampling technique.

Magnitude of preparedness toward COVID-19 among frontline HCWs working in public and private hospitals of Dire Dawa, Eastern Ethiopia, 2020 (n = 423).
Variables
Operational definitions
Data collection tools and procedures
Data were collected using a structured and pre-tested self-administered questionnaire which was adopted from WHO. 19 This questionnaire provides detailed information on socio-demographic, behavioral, and organizational variables useful for this study. Five data collectors and supervisors were assigned as interviewer and supervision, respectively. Background information and exposure status useful for the study were asked and collected in a form of a questionnaire.
Data quality control
To ensure the quality of the data, intensive training was given to all supervisors and data collectors. The data collection process was undertaken with frequent monitoring and supervision. The completeness and consistency of the data were monitored daily. Before the actual data collection period, 5% of the questionnaire was pre-tested and modified accordingly. Finally, double data entry was done to check the consistency of the data and minimize the entry errors.
Statistical analysis
First, data were entered into Epi Data Version 3.1 and exported to SPSS Version 23 for analysis. Descriptive statistics, binary, and multivariable logistic regression analysis were conducted to identify the association between the outcome and independent variables. All variables with a p-value less than or equal to 0.25 were taken into the multivariable model to control for all possible confounders. Those variables which were candidates for multivariable regression model were satisfied with the infection control policy (ICP): those are feel anxious, working department, current workplace, feel safe, and afraid of transmission, and also these variables were significant in the final mode. Hosmer–Lemeshow and Omnibus tests were done for model fitness. Multicollinearity was checked to see the linear correlation among the independent variables using variance inflation factor and standard error. Variables with variance inflation factor > 10 and standard error of > 2 were dropped from the multivariable analysis. The adjusted odds ratio (AOR) with the corresponding 95% confidence interval (CI) was calculated to see the strength of the association, and a p-value of less than 0.05 was declared to be statistically significant.
Results
Socio-demographic characteristics
All 423 HCW were enrolled in the study giving a response rate of 100%. The respondents’ mean age was 35.9 (± 7.9 SD) years with a majority (53.4%) of the respondents were females while 234 (55.3%) of them were working in private hospitals. Regarding the working department, 94 (22.2%) of them were working in a medical unit (Table 1).
Socio-demographic characteristics of HCWs in public and private hospitals of Dire Dawa, Eastern Ethiopia, 2020 (n = 423).

Knowledge about the virus, adherence to safety measures, and institutional protocol
When we see a safe source of information about COVID-19, 225 (53.2%) of the participants have got the information from social media. Regarding HCWs awareness on the route of COVID-19 transmission majority, 239 (56.5%) of them responded airborne while 86 (20.3%) of them responded through contact. Concerning the potential methods for prevention of transmission COVID-19, 210 (49.6%) of the participants responded by hand hygiene while 61 (14.4%) of the participants by avoiding the crowded area. Among all the respondents, 240 (56.7%) of the respondents always wear all PPE during the provision of health care to a COVID-19 patient, while the majority 365 (86.3%) of the respondents said PPE is always available at their institution (Table 2).
Knowledge about the virus, adherence to safety measure, and institutional protocol of frontline HCWs in public and private hospitals in Dire Dawa, Eastern Ethiopia, 2020 (n = 423).

PPE: personal protective equipment.
Psychological interaction
From the total of 423 participants, the majority, 278 (65.7%) of the respondents were feeling safe at their workplace with the existing safety precautions, whereas 293 (69.3%) of the respondents were afraid as they feel they could transmit the COVID-19 to their families, and the majority 286 (67.6%) of the respondents do not feel that infection prevention practice that exists at their hospital/clinic will decrease the risk of contracting COVID-19 for themselves and their colleagues (Table 3).
Psychological preparedness frontline HCW at public and private hospitals of Dire Dawa, Eastern Ethiopia (n = 423).

HCW: Health care worker.
Activities are done by HCW for patients with COVID-19
From the total participants, majority, 292 (69%) of them gave direct patient care and 407 (96.2%) of them had face-to-face contact (in the range of 1 m) with patients with COVID-19. Besides, 233 (55.1%) of the respondents had no incidental contact with respiratory/body fluid secretions while giving care to COVID-19 patients (Table 4).
HCW activities performed on COVID-19 patients in public and private hospitals of Dire Dawa, Eastern Ethiopia, 2020 (n = 423).
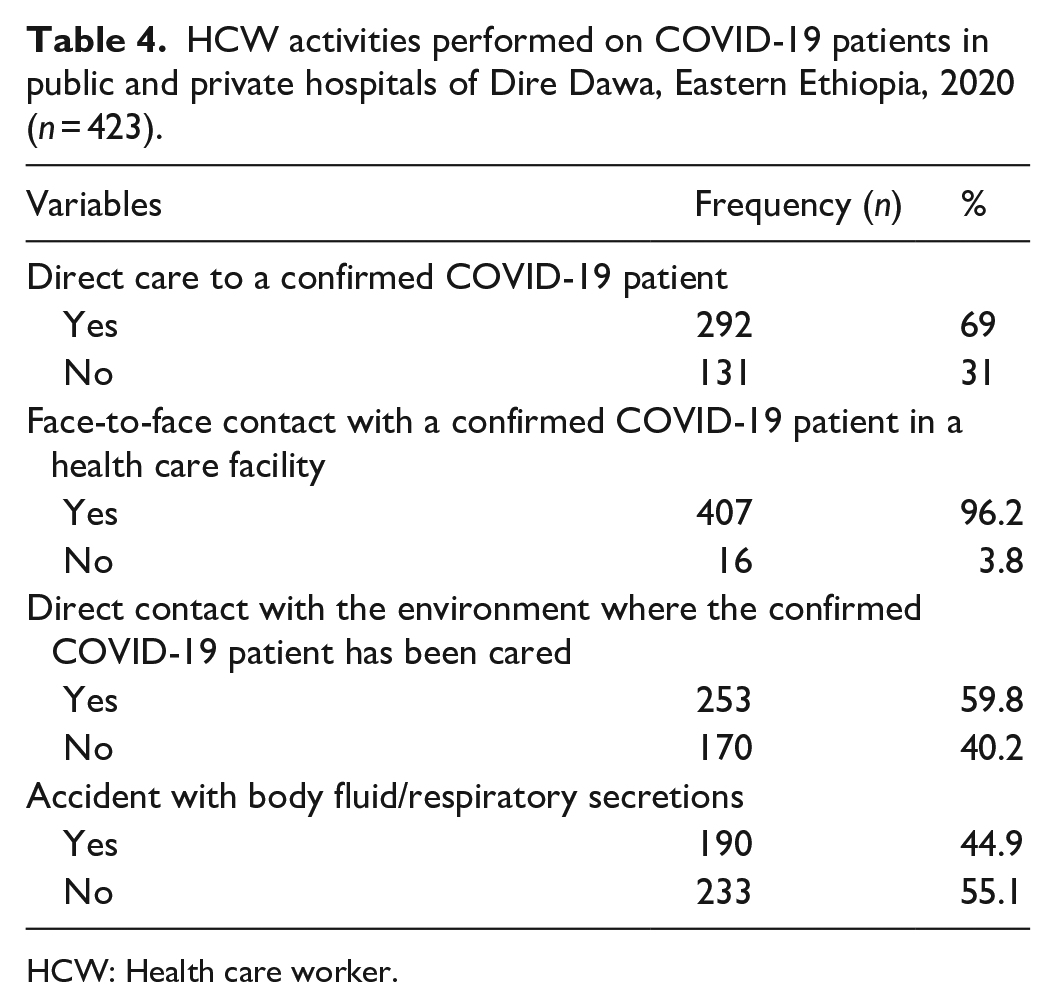
HCW: Health care worker.
Preparedness of HCW toward COVID-19 pandemic
This study revealed that only 173 (40.9%) participants had prepared for COVID-19, but the majority of 250 (59.1%) HCWs responded unprepared to COVID-19 pandemic (Figure 1).
Factors affecting preparedness of HCW toward COVID-19
The binary and multivariable logistic regression analyses showed that hospital type, feeling safe at the workplace with the existing safety measures, being afraid of transmitting the COVID-19 to patients, satisfied with the ICP at their institution, and feeling anxious concerning the likelihood of COVID-19 spread were found to be significantly associated with the preparedness of frontline HCW.
Those HCW working in public hospitals were almost three times more likely to be prepared for COVID-19 than those working in private hospitals (AOR = 2.7, 95% CI: 1.6–4.3).
Those HCWs, who were feeling safe at their workplace with the existing safety measures, were 3.3 times more likely to be prepared to COVID-19 than those who were not (AOR = 3.3, 95% CI: 1.7–6.4). Whereas, those HCWs, who were not scared of transmitting COVID-19 to patients, were 4.6 times more prepared than their counterparts (AOR = 4.6, 95% CI: 2.2–10.0).
HCWs, who were satisfied with the ICP at their institution, were six times more likely to be prepared for COVID-19 than their counterparts (AOR = 6.0, 95% CI: 2.3–15.0). In addition, those HCWs, who were not feeling anxious concerning the likelihood of COVID-19 spread, were two times more likely to be prepared to COVID-19 than those who were anxious (AOR = 2.1, 95% CI: 1.3–3.4) (Table 5).
Factors associated with preparedness toward COVID-19 among frontline HCWs working in public and private hospitals of Dire Dawa, Eastern Ethiopia, 2020 (n = 423).
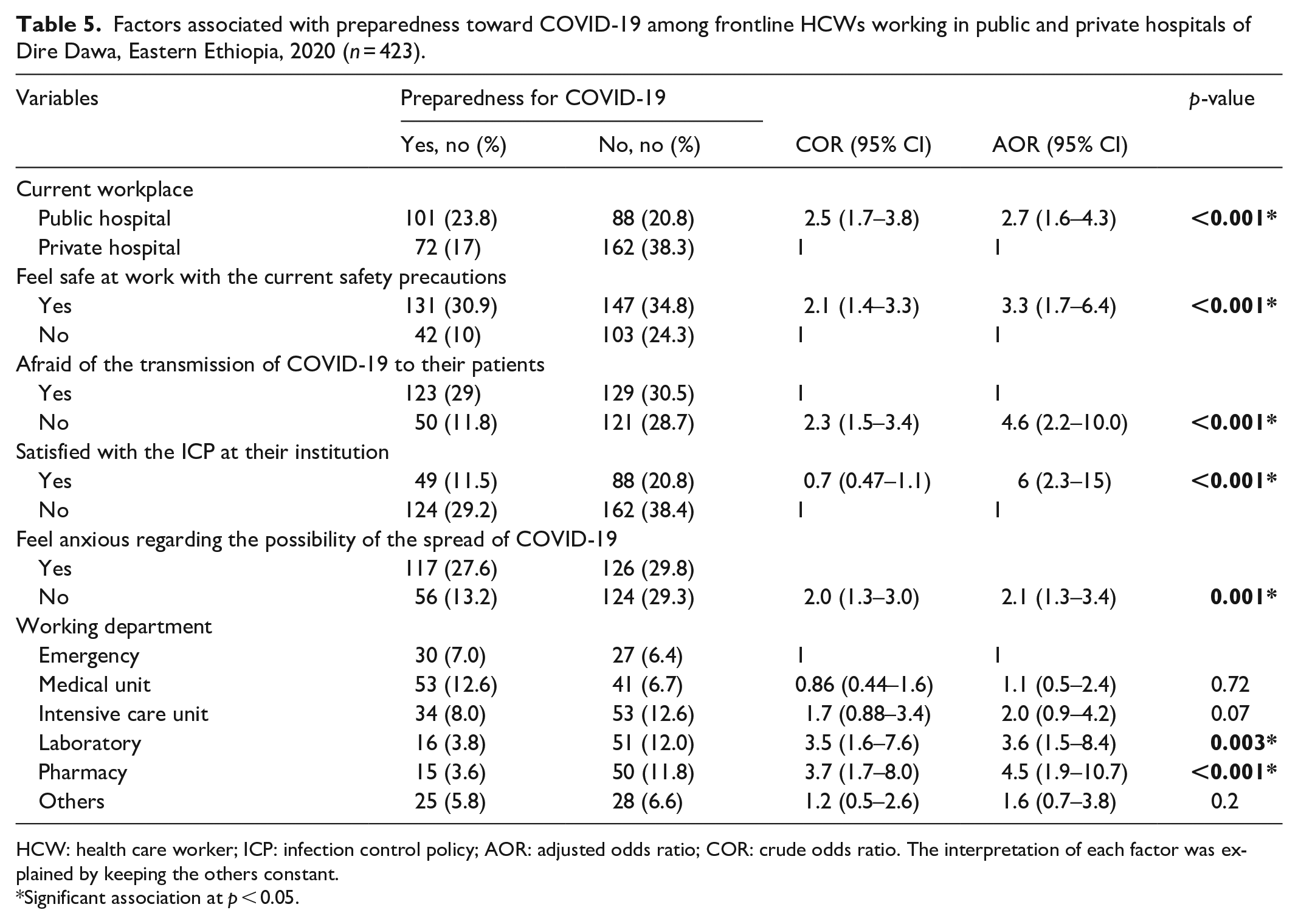
HCW: health care worker; ICP: infection control policy; AOR: adjusted odds ratio; COR: crude odds ratio. The interpretation of each factor was explained by keeping the others constant.
Significant association at p < 0.05.
Discussion
In this study, we tried to assess the level of HCWs’ preparedness and its associated factors toward COVID-19 pandemics in Eastern Ethiopia. Accordingly, it was found that only 40.9% (95% CI: 36.2–45.9) of HCWs have prepared for the COVID-19 pandemic. This study was almost similar with study conducted in North West of Ethiopia (41.3%). 20
In this study, we tried to look compared HCWs’ preparedness between public and private health facilities and it was found that HCWs in the public hospital were 2.7 times prepared for COVID-19 than those who were working in private hospitals. This is contradict with the study conducted in Palestine where governmental hospitals were significantly less likely to have all appropriate PPE than non-governmental institutions (p = 0.001). The difference might be due to the lack of accesses of PPE equipment in Ethiopia to distribute for private health facilities. In addition, this could be because of the availability and accessibility of PPE and hygiene materials within public hospitals/HCs, as support from governmental and non-governmental organizations prioritize to private health facilities. 21
This study also identified a significant association between HCW’s preparedness and satisfaction with the infection prevention strategy at their hospital. Accordingly, those satisfied HCWs were 6.0 times more likely to be prepared to COVID-19 than those who were not. This finding is congruent with a similar study conducted in Ethiopia. 22 This could satisfy health professionals to have a good psychological and physical readiness to combat COVID-19 infection.
A previous study that was done in Jordan, 2020 21 showed a significant association between HCW’s preparedness and is not anxiety about the likelihood of COVID-19 spread and the shooting up of cases, and this was in line with the current study finding where HCWs, who were unanxious about the spread of COVID-19 and surge of positive cases, were 2.1 times more likely to be prepared to COVID-19 (95% CI: 1.3–3.4) when compared to their counterpart.
In this study, those HCWs, who were unafraid of transmitting COVID-19 to patients, were 4.6 times more likely to be prepared to COVID-19 than those who were scared. This finding could indirectly suggest a difference in self-assurance developed in advance among HCWs which has to do with confidence while doing their routines, either learned or gained knowledge and experiences; this means that unprepared HCWs are scared to transmit their patients. This finding was inconsistent with the studies done in African countries. 23 The difference might be personal belief/thinking that means scared to transmit disease.
In the current study, a sense of safety or security/ feeling safe at their workplace with the existing safety measures showed significant association with preparedness toward COVID-19. Accordingly, HCWs having a sense of safety or feeling of security were 3.3 times more likely to prepare than those who do not feel safe. The possible reason for the observed association could be the positive impression of HCWs possesses on their work environment, intellectual perception, or conscious awareness. In action to this, those HCWs, who feel safe at the workplace, could have enough confidence about their preparedness compared to their counterparts. This finding is supported by the study conducted in India. 13
Although feeling safe about their colleagues with the existing safety measures, concerned about dealing with COVID-19 patients and age was previously reported to have a significant effect on preparedness to COVID-19,24,25 none of them showed such effect in our study.24,25
Since the study was cross-sectional, it did not establish a possible temporal relationship. Also, the scarcity of similar studies makes it difficult to compare our findings with other findings. Finally, our search strategy found limited studies, especially no studies from our country.
Conclusion
Only two-fifths of HCWs were prepared for COVID-19 pandemic. Working in public hospitals, having a sense of safety or security/ at the workplace with the existing safety measures, being unafraid transmitting the COVID-19 to patients, satisfaction with the ICP at their institution, and being unanxious about the likelihood of COVID-19 spread were found to be positively associated with the preparedness of frontline HCWs. Therefore, intensive training focused on the emotional and psychological preparation of HCWs should be given regardless of their profession or working place. Moreover, stakeholders should work hard to increase HCWs’ preparedness in both private and public health facilities through regular inspection, supervision, and provision of PPE. We strongly recommend that intensive work should be done to create a safe and conducive work environment in emergency units for both private and public health facilities.
Supplemental Material
sj-doc-1-smo-10.1177_20503121211054970 – Supplemental material for Preparedness toward COVID-19 pandemics and associated factors among health care workers in Dire Dawa Hospitals, Eastern Ethiopia: A facility-based cross-sectional study
Supplemental material, sj-doc-1-smo-10.1177_20503121211054970 for Preparedness toward COVID-19 pandemics and associated factors among health care workers in Dire Dawa Hospitals, Eastern Ethiopia: A facility-based cross-sectional study by Tameru Menberu, Robel Mekonnen, Yibekal Manaye, Mesfin Kebede, Yonatan Solomon, Alekaw Sema, Bekele Yazie and Agumas Fentahun Ayalew in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank Dire Dawa Universities for their financial and unreserved technical support. They also thank the study participants for their willingness to take part in the study and all data collectors for their active participation. Last but not the least they thank friends for their wonderful feedback on the scientific content of the article.
Author Contributions
T.M., A.F.A., and Y.M. conceived the review topic and objectives; T.M., Y.S., R.M., M.K., and B.Y. participated in the study selection, data extraction, and analysis; T.M., Y.S., A.S., and Y.M. reviewed the article critically for its scientific content; all authors reviewed and approved the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethical clearance was obtained from the Research and Technology Interchange (RTI) of Dire Dawa University with Ref No: DDU/RTI/1912/2020. Following approval, a written official letter of cooperation was distributed to each health facilities. Informed written consent was obtained from all subjects before the study. Confidentiality was assured throughout the process. The names and addresses of the participants were not recorded in the questionnaire. Furthermore, all the basic principles of human research ethics (respect of persons, beneficence, voluntary participation, confidentiality, and justice) were respected.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed written consent was obtained from all subjects before the study. Confidentiality was assured throughout the process.
Data availability
All related data have been presented within the article. The dataset supporting the conclusions of this article is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.