
Abstract
Objective:
Lebanon has historically maintained high immunization coverage rates for most routine vaccines. However, an increase in poverty rates coupled with an influx of over a million refugees posed significant challenges to the national immunization program. In response, an accelerated immunization activities (AIA) program, encompassing community-based outreach and referral activities, was launched to increase the demand for childhood vaccination through the public healthcare system. Despite this effort, uptake among refugee and host community households remained low, resulting in pockets of low immunization coverage rates. This study investigates the barriers that prevent households in low coverage areas from vaccinating their children, and evaluates a behavior change intervention designed to overcome the identified social, perceptual, and cognitive barriers.
Methods:
Households with un- or under-vaccinated children were recruited from seven cadastres with low immunization coverage rates. A mixed methods approach, including stakeholder interviews and field observations, was employed to identify the main barriers to vaccination. Thereafter, a cluster randomized trial was conducted to evaluate the impact of a visual planning aid comprising five behavior change techniques (nudges) on vaccine uptake.
Results:
A total of 12,332 un- or under-vaccinated children from 6160 households (3045 (49.4%) control households; 3115 (50.6%) treated households) were reached during the trial. The observed vaccination rates were 13.5% and 20.2% for control and treated households, respectively. This represents a 6.7 percentage points increase in the likelihood of a treated household to vaccinate at least one child, compared to the control group. At least 390 additional children benefited from life-saving vaccines due to the behavioral intervention.
Conclusions:
This study highlights the importance of integrating behavioral insights into vaccination campaigns and programs, especially in low resource settings, to ensure that more children can benefit from life-saving vaccines.
Introduction
Childhood vaccination is one of the most cost-effective public health interventions available, averting 2.5 million deaths from preventable diseases every year.1,2 Even though routine vaccines are widely accepted among parents, many children in low- and middle-income countries (LMICs) remain un- or under-vaccinated. 3 Particularly vulnerable are crisis-affected and refugee hosting LMICs in the Middle East and North Africa (MENA) region, 4 including Lebanon which has the highest per capita intake of refugees, comprising 21.8% of its population. 5
Lebanon has generally maintained high immunization coverage rates, nearing 90% for most routine vaccines (Diptheria, Tetanus, Pertussis (DTaP), Hepatitis B, Oral Polivirus Vaccine (OPV), and Haemophilus influenzae type B (HiB)). 6 However, a rise in poverty levels, coupled with an influx of more than a million refugee in 2011—many of whom were missing routine vaccines 7 posed significant challenges to the national immunization program, which provides vaccination to more than half the children residing in Lebanon.
Evidence of weakening immunization coverage rates was first detected following a measles outbreak in 2013, and a drastic rise in the cases of mumps in 2015. 8 This was validated by a district-based cluster survey conducted in 2016. The survey revealed pockets of low immunization coverage rates in several districts, among both refugee and host community households. 9
As a strengthening strategy to the national immunization program, the Ministry of Public Health (MoPH) Lebanon, in collaboration with United Nations Children’s Fund (UNICEF), launched an accelerated immunization activities (AIA) program in November 2017 to provide free quality immunization services for every child through the primary healthcare system. 10 In addition to the support offered to primary healthcare centers (PHCs), the program employed a community-based outreach approach to (a) identify un- or under-vaccinated children, (b) educate and raise awareness of caregivers on the importance of childhood vaccination, (c) collect children’s vaccination records, (d) refer children missing vaccines to the nearest participating healthcare center, and (e) follow-up with caregivers to ensure that full immunization is achieved. Figure 1 provides an overview of the AIA conceptual framework and theory of change.

AIA conceptual framework and theory of change. 10
Raising awareness, strengthening public healthcare system, and providing access to free quality services are necessary prerequisites to facilitate and enable the uptake of childhood vaccination. However, these measures are seldom enough to ensure sufficient demand from beneficiaries. 11 Despite caregivers’ best intentions, evidence from years of research in psychology and the behavioral sciences on vaccine uptake point to the presence of decision biases and social influences (henceforth behavioral barriers) that impact the motivation to vaccinate.12–14 Identifying these behavioral barriers and addressing them using the appropriate behavior change techniques 15 is critical for the success of any campaign or activity seeking to boost national immunization rates.
This study investigates the behavioral barriers diminishing the demand for childhood vaccination among households targeted by the AIA program, and assesses the impact of a behavior change intervention designed to address the perceptual, social, and cognitive barriers that were identified. The intervention consisted of a visual planning aid in the form of a calendar comprising five behavior change techniques (nudges). 16 It was evaluated using a clustered randomized controlled trial in three districts.
This is the first study investigating the effectiveness of nudging and behavioral insights to increase the demand for childhood vaccination among refugee and marginalized host community households in LMICs across the MENA region. 17
Methods
Setting
This study was implemented in seven cadastres within three urban districts in Lebanon: Beirut, Baabda and Matn—refer to Table 3. It took place between August 2018 and March 2019.
The shortlisted cadastres were chosen in coordination with the MoPH and UNICEF based on the following criteria: (a) high population density with a mix of Lebanese and non-Lebanese households; (b) high vulnerability with low immunization coverage rates; and (c) proximity to participating healthcare centers.
Design
Following weeks of extensive fieldwork, including stakeholder interviews and field observations (refer to Table 1 for details), several behavioral barriers were identified. Among these barriers, the most prevalent were forgetfulness and neglect as most beneficiaries lived in poverty, and therefore had diverted priorities. 18
Overview of the stakeholder interviews and field observations investigating the behavioral barriers to vaccination.

To offset these barriers, a visual planning aid in the form of a calendar was designed. The planning aid consisted of five nudges identified from the MINDSPACE framework. 19 It included factual statements about the uptake of vaccination by other beneficiaries (norms/social proof); a non-binding pledge by parents to vaccinate their children (commitment); an implementation intention plan, 20 whereby parents would specify the date and location in which they will vaccinate their children (implementation intentions); the MoPH’s guarantee of the quality and effectiveness of the vaccines (messenger); and a request to place the calendar somewhere visible (salience). Table 2 summarizes the identified behavioral barriers and nudges used to offset them.
Summary of the behavioral barriers and nudges.

Figures 2 and 3 below present the prototype and the final design of the visual planning aid.

Prototype of the visual planning aid.

Final design of the visual planning aid.
Participants
The target sample consisted of households with children aged 0–16 years who were falling behind their routine vaccination schedule according to Lebanon’s national immunization calendar. 23 Since the AIA program predated the intervention, many households in the target areas were being visited for the second time by outreach teams. Accordingly, the sample included households that were previously referred to a healthcare center but failed to maintain their children’s vaccination up to date (follow-up visits), as well as newly identified households with un- or under-vaccinated children (outreach visits). Households with children who were up to date with their vaccination were excluded from the trial.
It was estimated that a total of 7500 eligible households could be reached between December 2018 and January 2019, enough to detect a 5-percentage point increase in the likelihood of a treated household to vaccinate at least one child (Assuming statistical significance at 5%, statistical power of 80%, a standard deviation of 0.5 and an intra-cluster correlation of 1.5%). The sample size of 7500 was determined based on the capacity of each outreach team (n = 37) to complete six household visits each day for a period of 7 weeks, assuming four working hours per day, 5 days per week excluding public holidays. All outreach activities, including follow-up visits, were concluded by 31 January 2019.
Ethical approval
This study was not subject to a formal ethical review by an Institutional review board or ethics committee as this requirement was waived by UNICEF and the MoPH Lebanon for the following reasons:
A comprehensive review of the study was undertaken by the Primary Healthcare Department at the MoPH Lebanon to ensure that appropriate measures were taken to protect the rights, safety, and welfare of participants.
The study was conducted as part of an existing and ongoing outreach and referral activity which was already approved by UNICEF and the MoPH Lebanon.
The intervention was judged to be low risk to beneficiaries and of high priority due to a measles outbreak in Lebanon at the time, and therefore expediting the process was necessary to maximize uptake.
Informed consent
A verbal informed consent to participate in the outreach and referral activity of the AIA program was obtained by the outreach teams from the children’s legally authorized representatives during their home visits. The representatives were first informed about the objectives of the program and their right to opt out before their children’s demographic and vaccination status data were collected. Those who did not offer consent were excluded from the program as well as the behavioral intervention.
The decision to obtain verbal consent was made by the AIA program teams at UNICEF and the MoPH Lebanon before the research team got involved. To minimize disruption, the research team, along with UNICEF and the MoPH Lebanon, decided to maintain the same consent procedure. Acquiring verbal consent is a standard practice in door-to-door outreach activities and research involving refugee or marginalized population groups in Lebanon due to their low levels of literacy. 6
Additional consent was obtained from the legally authorized representatives of children who were eligible to participate in the behavioral intervention study. Representatives who agreed to be included in the study were asked to tick a checkbox and sign their name on a data collection slip, consenting to be part of the behavioral study, and to receive further communications from the MoPH Lebanon. Participants were provided with the ministry’s phone number in case they wanted to further enquire about the study or file a complaint.
Trial registration
AEA RCT Registry: AEARCTR-0003680. Registered 21 October 2019. https://doi.org/10.1257/rct.3680-1.0
Randomization
The intervention was implemented in seven cadastres located within three districts, with the help of 74 outreach workers, 12 supervisors and four field coordinators who were trained to deliver the behavioral intervention along with the standard AIA outreach activities. The cadastres were further divided into 12 zones, with two to four outreach teams and a supervisor assigned to each zone depending on the size of the target population within the zone. Table 3 shows the distribution of outreach teams across cadastres and study arms.
Distribution of outreach teams by cadastres and study arms.

The intervention was evaluated using a clustered randomized controlled trial at the level of outreach teams. A total of 37 trained teams consisting of two individuals each were randomly assigned to control (n = 17) and treatment groups (n = 20). A stratified randomization approach was employed to assess treatment effects within cadastres. Consequently, half of the teams within each cadastre were assigned to the control group, while the other half was assigned to the treatment group. Assignment to the treatment group was prioritized in cadastres with an odd number of outreach teams to maximize the number of households benefiting from the behavioral intervention.
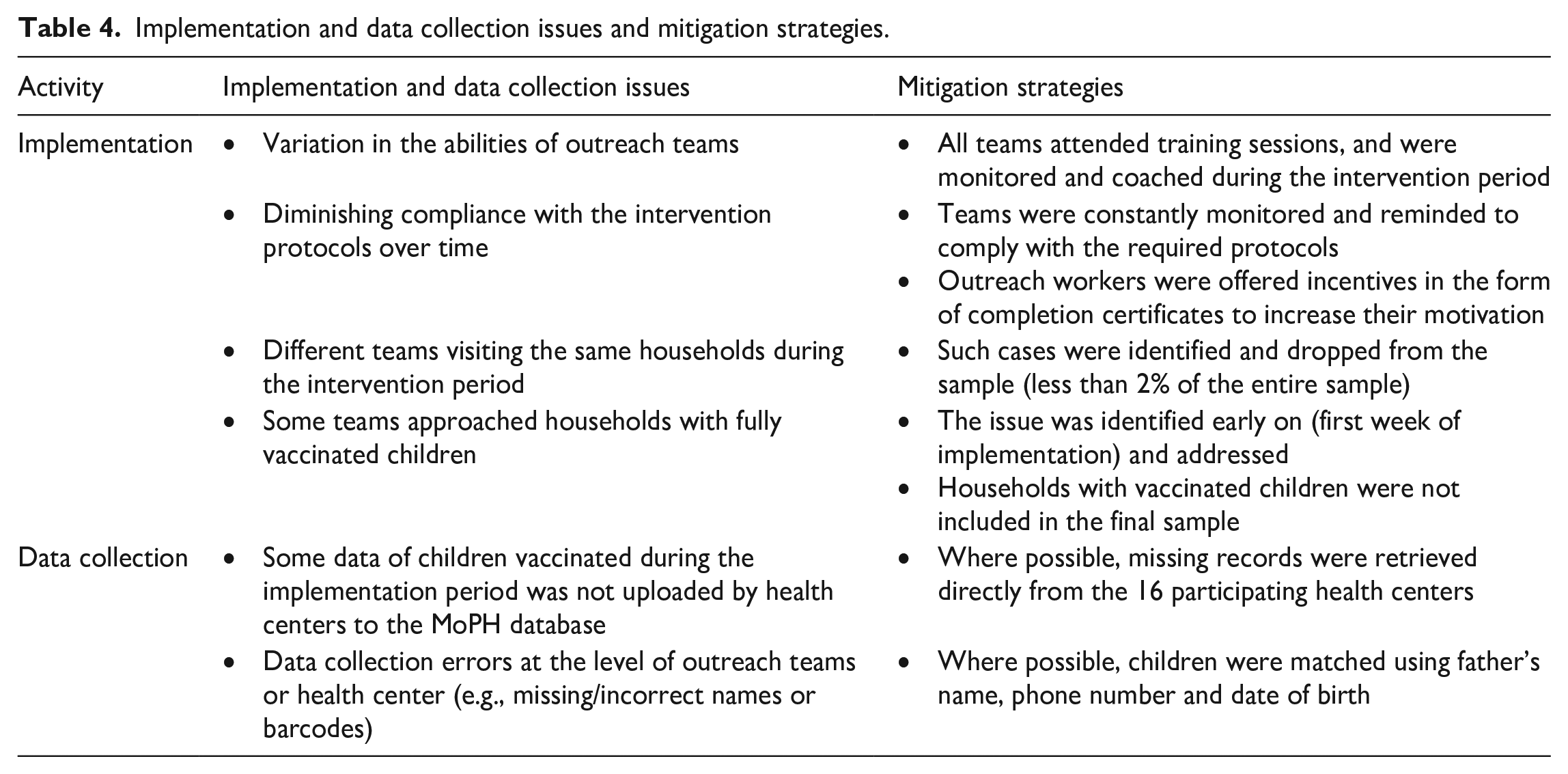
Outreach teams assigned to the treatment group were given copies of the calendar to distribute to eligible households alongside their standard outreach activities. Meanwhile, the control group continued to use the standard outreach approach. Each group completed separate training sessions to remind them about the AIA implementation protocols, introduce them to the new procedures required by the intervention, and run mock outreach activities. Additionally, the teams were spot-checked during the implementation period to identify and mitigate implementation and data collection issues. Table 4 lists the implementation and data collection issues that were identified, along with the measures taken to mitigate these issues.
Implementation and data collection issues and mitigation strategies.
Primary outcome
The primary outcome was a binary (yes/no) decision of an eligible household to vaccinate at least one child. Measuring uptake at the household level, as opposed to the child level was judged to be more robust since (a) the choice to vaccinate a child is usually taken by the parents who act as proxy decision makers for the child, 24 and (b) the decision to vaccinate a child and his/her siblings is likely to be highly correlated since the additional cost of vaccinating an extra child (transportation cost, waiting time, etc.) is relatively low.
The vaccination status of children reached during the intervention period was retrieved from the MoPH database using barcodes preassigned to each child. Missing records of vaccinated children that were not uploaded to the MoPH database at the time of data collection were retrieved directly from the 16 participating health centers. Out of the 1726 records of vaccinated children retrieved during the study, around 5% (n = 83) were obtained from the health centers, while the rest (n = 1643) were extracted from the MoPH database. Figure 4 illustrates the data collection protocol that was implemented.

Data collection protocol.
The cutoff date for data collection was 28 February 2019. Once collected, the child level data were collapsed into the household level by means of a deterministic record matching method, 25 using the child’s family name, father’s name, and household phone number.
We also collected data about the visit type (outreach or follow-up) and date, the outreach team conducting the visit, the household location, the referral health center, and the vaccination date, as well as children’s gender, nationality, and date of birth.
Data analysis
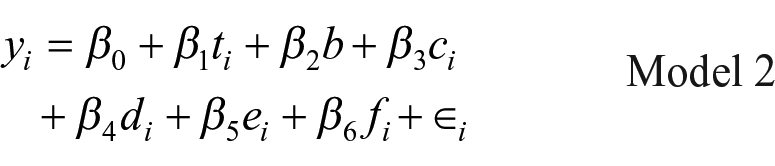
The primary analysis assessed the impact of the calendar on vaccination uptake among treated households, relative to the control group. As such, our primary model regressed each household’s (i) vaccination status (y) on a treatment dummy (t) while controlling for our stratification variable (b) corresponding to the seven cadastres. The effect of the calendar is represented by the treatment coefficient (

In addition to the primary analysis, we investigated the potential effects of the following covariates: (a) number of children missing vaccines per household to assess economies of scale; (b) number of boys to girls missing vaccines within each household to assess gender bias; (c) household nationality (Lebanese versus non-Lebanese); and (d) the type of household visit (outreach versus follow-up).
The analyses were conducted using a linear probability model (LPM) with adjusted standard errors using the variance-covariance estimator function in Stata/MP 17.0 to account for the clustered randomization design at the outreach team level.26,27 The use of LPM to estimate the causal effect of experimental treatments on binary outcomes has been shown to yield similar estimates to logistic regressions, with the benefit of being easier to implement and interpret.28,29 Average marginal effects from a logistic regression were estimated and compared to the LPM model to ensure the robustness of results.
Results
Main results
The sample consisted of 12,332 children from 6160 households. The distribution between treatment and control groups was evenly split with 3045 (49.4%) control households versus 3115 (50.6%) treated households. On average, each household had two children missing vaccines, with a standard deviation of 1.24. The average male-to-female ratio within households was approximately one, indicating an equal distribution of boys and girls. The average child age was approximately 7 years, with a standard deviation of 4 years.
The majority of households reached were Syrian (69%), while Lebanese households comprised most of the remaining sample (28%). Around 47% of the households were previously referred to a health center, while the rest were visited for the first time. Most households were concentrated in four cadastres: Chiyah (58%), Bir Hassan (15%), Mrayjeh (9.5%) and Mazraa (7.5%). Each of the remaining cadastres comprised less than 5% of the households reached.
The treatment and control groups were balanced based on the covariates and key sample characteristics as shown in Table 5.
Sample characteristics and randomization checks.

A summary of the analysis is presented in Table 6. Compared to the control group, treated household were 6.7 percentage points (pp) more likely to vaccinate at least one child (Adjusted 95% CI: (1.5 pp, 11.9 pp), p < 0.05). The average uptake among households receiving the calendar was 20.2% versus 13.5% in the control group. This effect was robust to the addition of covariates.
Analysis of the impact on vaccination uptake.

Note: Adjusted 95% CI refer to design effect adjusted confidence intervals used to account for intra-class correlation due to randomization at the outreach team level. The excluded cadastre (stratum) is Bir Hassan.
The average age of vaccinated children was 6.8 years, with a standard deviation of 4 years. Vaccinated children in the control group were, on average, 8 months younger than those in the treatment group with a mean age of 6.4 years (SD = 4.1 years) versus 7.05 years (SD = 3.9 years) in the treatment group, p < 0.01.
Additional results: Interval between household visits and vaccination dates
Overall, vaccinated children reported to a health center within 13.5 days (SD = 11.6 days) following a household visit. Treated children were on average 1.6 days earlier to vaccinate compared to those in the control group, averaging 13.0 days (SD = 10.85) compared to 14.6 days (SD = 12.8), respectively (95% CI: (0.20 days, 3.0 days), p < 0.01). Figures 5 and 6 show the number and cumulative proportion of vaccinated children by days between the household visit and vaccination date, respectively.
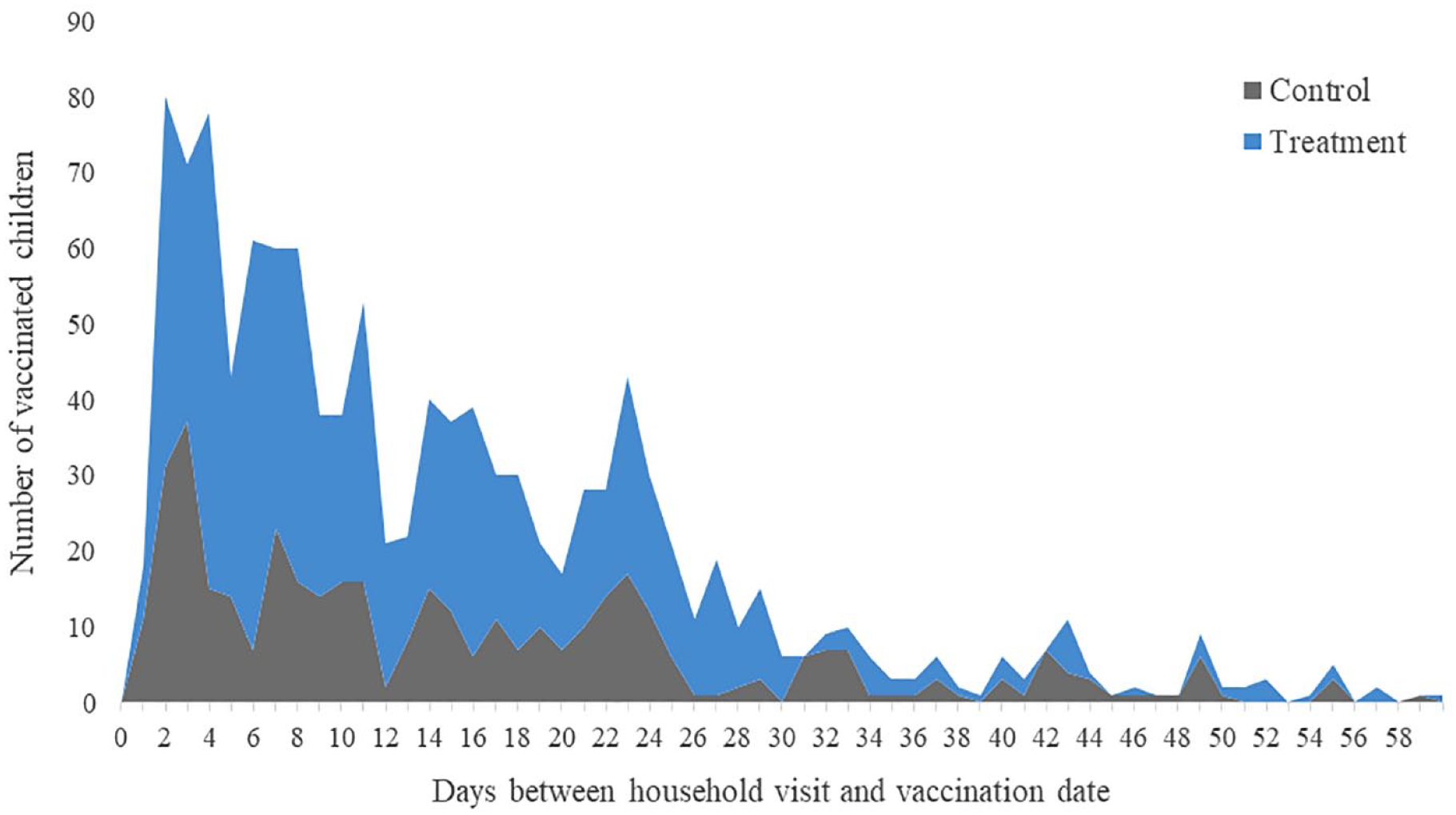
Number of vaccinated children by days between the household visit and vaccination date.

Cumulative proportion of vaccinated children by days between the household visit and vaccination date.
It should be noted that the vaccination dates for 550 out of 1726 vaccinated children (circa 32%) were missing, with the majority of missing records (>80%) coming from 6 out of the 16 healthcare centers.
Additional results: Covariates
Nationality was a significant determinant of overall uptake, such that Lebanese households were 3.1 pp less likely to demand vaccination relative to non-Lebanese households (95% CI: (−5.0 pp, −1.0 pp), p < 0.01). However, we find no significant difference in the treatment effect between Lebanese and non-Lebanese households (χ2 = 0.766, p = 0.381).
The demand for vaccination increased 1.8 pp for every additional unvaccinated child in the household (Adjusted 95% CI: (0.6 pp, 2.9 pp), p < 0.01).
Overall, the type of visit (outreach versus follow-up) had no significant impact on the uptake (−0.4 pp, Adjusted 95% CI: (−3.4 pp, 2.5 pp), p = 0.772). Likewise, there was no significant gender effect such that households were equally likely to vaccinate boys and girls (0.009 pp, 95% CI: (−0.5 pp, 2.2 pp), p = 0.212).
Table 7 shows the estimates means and 95% confidence interval of the main covariates included in the analysis.
Estimated means and confidence interval of the main covariates.
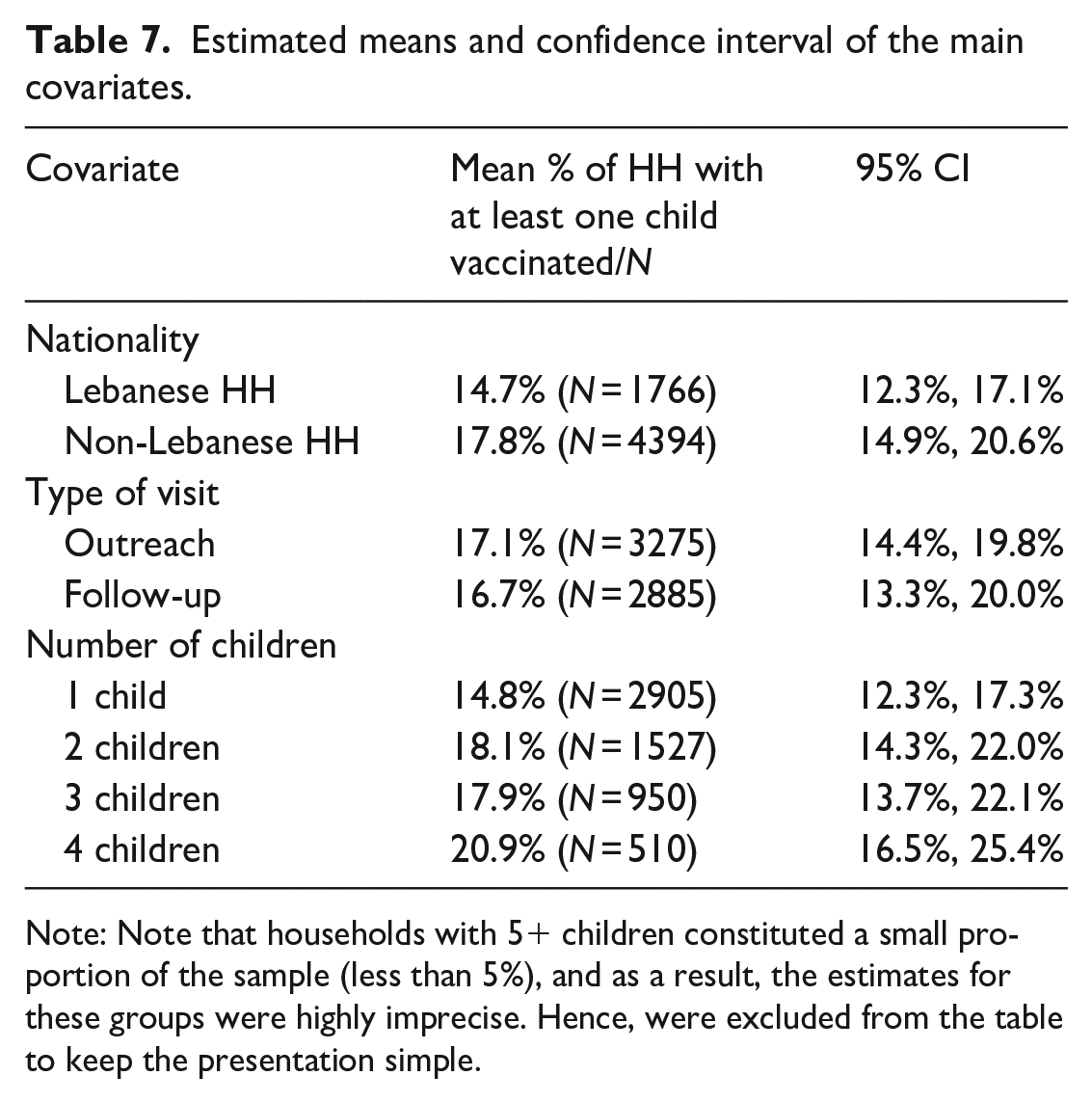
Note: Note that households with 5+ children constituted a small proportion of the sample (less than 5%), and as a result, the estimates for these groups were highly imprecise. Hence, were excluded from the table to keep the presentation simple.
Additional results: Cadastres
Breaking down the result to the level of cadastres revealed positive effects in six out of the seven target areas. However, these effects were only significant in three cadastres (p < 0.05) – refer to Figure 7 for an overview of the cadastre-level treatment effects.

Treatment effects by cadastre.
Discussion
The research concerning the effectiveness of nudging on vaccination uptake is mixed, with outcomes varying based on the context of the intervention. Studies that offered incentives, increased the salience of information, or used trusted messengers have shown the most promising results. 30 However, most of these studies have been implemented in high-income countries, and therefore may not generalize to LMICs where the demand for vaccination is affected by different factors and barriers. Additionally, many of the existing studies suffer from methodological limitations, such as relying on self-reported attitudes and intentions rather than directly observing vaccination behavior, as well as employing non-randomized evaluation methods to assess impact. 30
The current study investigates the perceptual, social, and cognitive barriers to childhood vaccination, and evaluates the impact of a behavioral intervention comprising a visual planning aid featuring five nudges. It was integrated into an ongoing community-based outreach program aimed at raising awareness and referring un- or under-vaccinated children to primary healthcare centers across low coverage areas in Lebanon.
This study makes significant contributions to the existing body of research on the efficacy of nudging in the context of vaccination. One, it targets a particularly challenging demographic encompassing refugee and marginalized host community households in a resource-constrained LMIC. Two, this study employs a robust clustered randomized trial to rigorously evaluate the impact of the behavioral intervention on the demand for vaccination. Three, it departs from the reliance on self-reported intentions by directly observing vaccination behavior.
The results show that households provided with the visual planning aid were 6.8 percentage points more likely to vaccinate their children compared to those receiving the standard outreach approach. This result was statistically significant and practically meaningful, with at least 220 additional households (390 additional children) receiving life-saving vaccines as a result of the intervention (outreach + visual planning aid). Additionally, the duration between the household visit and vaccination date was 1.6 days shorter for treated households, suggesting that the intervention may have encouraged parents to act faster.
These findings are consistent with previous research on the effectiveness of visual nudges to improve health outcomes in resource-constrained settings. For instance, in Lebanon, a study using visual self-assessment cards increased mental health patients’ follow-up attendance by 9%, with new patients showing a 15% increase compared to a control group. 31 In Pakistan, a redesigned immunization card with prominent reminders led to a 25% increase in Diphtheria, Pertussis and Tetanus vaccine (DPT3) completion rates among treated children, compared to a control group. 32
Additional results
In addition to the main results, our study revealed important insights regarding the impact of locality, nationality, and number of children missing vaccines. With respect to locality, we find large variations in the average uptake rates between cadastres, ranging from a low of 3.2% to a high of 24.6%. One district, El Matn, comprised the two cadastres (Borj Hammoud and Sed El Bouchrieh) with the lowest uptake rates, averaging 7.4% versus 16.9% across the entire sample. While this is highly speculative, we hypothesize that the lack of real integration of Syrian refugees in the aforementioned district, 33 coupled with lower quality of outreach observed in those districts, may have contributed to the lower uptake rates.
Nationality played a significant role, with non-Lebanese households, namely Syrian households, recording higher uptake rates, on average, than Lebanese households. This is not surprising given that Syrian beneficiaries are in general more likely to utilize the services of primary healthcare centers, while Lebanese beneficiaries prefer to seek private care. 34
The probability of household demanding vaccination increased with the number of un- or under-vaccination children, likely because of the “economies of scale” as the marginal cost of vaccination (effort, time, inconvenience, etc.) was smaller for every additional child, while the benefits per child remained the same.
Finally, in line with previous findings from Lebanon, 6 the child’s gender was not a significant predictor of vaccination uptake, with households equally likely to vaccinate boys and girls.
Limitations
This study has several limitations which may have diminished the observed effects. First, the intervention was introduced during the last phase of the AIA program implementation, thereby limiting the data collection period to 12 weeks only. Therefore, it was not possible to evaluate the long-term effects of the calendar, and to assess whether the positive effects on vaccination uptake were sustained in the long run. Two, even though the beneficiaries were always referred to one of the participating primary healthcare centers, some of them, namely Lebanese, may have opted to vaccinate at a private clinic. 34 As a result, the observed vaccination rates may not reflect the true uptake of vaccination. Three, it was not possible to collect all the vaccination data that should have been available as some health centers neglected to record the names or barcodes of some vaccinated children. This is likely to have resulted in an observed vaccination rate that is lower than the actual one. Four, as previously mentioned, most households reached were of Syrian. We suspect that Syrian households may have been easier to reach (more likely to be at home or receive the outreach workers), potentially resulting in a selection bias in the observed treatment effect. Lastly, the variation in the ability and motivation of outreach teams may have also affected administration of the treatment. This implies that the intervention may not have been implemented homogenously across households. While randomization should have minimized such effects, it may not completely ensure homogeneity within treatment teams, and between control and treatment groups due to the relatively small number of teams available.
Future interventions should consider the limitations of cluster randomized evaluations, and if feasible, opt for a unit of randomization that would yield a large enough sample to ensure homogeneity between the control and treatment groups. 35
Conclusion
This study highlights the importance of using behavioral science methods and insights to enhance the effectiveness of community-based outreach programs in low resource settings. Specifically, the study demonstrates how simple, low-cost nudges such as intention-implementation plans, norms, and commitments delivered in an appealing visual planning aid can be effective at addressing perceptual, social, and cognitive barriers to increase the demand for childhood vaccination. The study also identifies important factors that influence vaccine uptake, including locality, nationality, and number of un- or under-vaccinated children in the household. These findings have important implications for future vaccination programs in Lebanon and other similar contexts, and can help inform the design of future vaccination programs to ensure that more children receive life-saving vaccines.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Andrew Saab and Jana Kontar from Nudge Lebanon; Ali Roumani, Yara Hamadeh, and Khalil Ismail from MoPH Lebanon; Vincent Petit, Diala Ktaiche, Farah Mazloum, Genevieve Begkoyian and Jamil El Khoury from UNICEF Lebanon; the Lebanese Association for Early Childhood Development, and Makhzoumi Foundation for their valuable contributions to this research.
Authors contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. AO, FM, AH, NS, JY, JB, RC, WK, and RH contributed to the conception, design and implementation of the study. AO, FM, AH, and NS contributed to the data acquisition and analysis of the formative research. AO contributed to the data analysis and interpretation of the randomized evaluation, and produced the draft manuscript. All authors provided input into drafts, read, and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nudge Lebanon——a nongovernmental and non-profit organization—was contracted by UNICEF Lebanon to design and implement this study, including data collection and analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by UNICEF Lebanon through a grant received from the Bureau of Population, Refugees, and Migration (BPRM) – U.S. Department of State.