
Abstract
Objective:
A better understanding of tuberculosis-related knowledge, attitude, practices in the community, and other issues can help in implementing evidence-driven activities to control tuberculosis in Jordan. This study aimed to assess tuberculosis-related knowledge, attitude, and behaviors among refugees, migrants, and general population, and assess their stigmatizing and discrimination attitudes toward tuberculosis patients, social behavior toward tuberculosis, and healthcare-seeking behaviors.
Methods:
A cross-sectional study was conducted among Jordanians, Syrian refugees, and migrants living in four governorates including Amman, Zarqa, Mafraq, and Irbid during the study period of June to September 2021. A structured questionnaire was developed to collect data via face-to-face interviews. Descriptive statistics, chi-square test, and general linear model procedure were used to analyze data.
Results:
A total of 2302 (27.7% Jordanians, 25.7% urban refugees, 22.1% camp refugees, and 24.5% migrants) participated in this study. Of the total, 90.1% of participants reported that they have heard of tuberculosis. However, 88.9% of Jordanians, 92.8% of urban refugees, 92% of camp refugees, and 90.5% of migrants had low level of tuberculosis-related knowledge. About 62.0% of urban refugees, 54.8% of Jordanians, 43.0% of camp refugees, and 55.4% of migrants had moderate to high stigmatizing attitude toward tuberculosis patients. About 15.1% of Jordanians, 10.6% of urban refugees, 23.7% of camp refugees, and 16.1% of migrants had moderate to high level of discriminating attitude toward tuberculosis patients. Camp refugees had a significantly higher level of discriminating attitude toward tuberculosis patients than the other groups.
Conclusion:
This study identified significant gaps in tuberculosis-related knowledge among the targeted groups. Moderate to high level of stigmatizing attitude was reported by a considerable proportion of the study participants. This suggests a need for public health education programs to educate people on tuberculosis causes, signs, symptoms, mode of transmission, and address related stigma, especially among the most disadvantaged and affected communities in Jordan.
Introduction
Tuberculosis (TB) is a serious chronic infectious disease that occurs in every part of the world. 1 According to the World Health Organization (WHO), about a quarter of the world’s population is infected with Mycobacterium tuberculosis and 10 million people fall ill with TB every year. 1 Despite that TB is a preventable and curable disease, it causes one and half million deaths each year that makes it the top infectious killer in the world. 2 Moreover, TB is the leading cause of death of people living with HIV causing more than one-third of all AIDS-related deaths. 3
The largest number of new TB cases occurred in the South-East Asian region accounting for 45% of TB new cases in 2021. 4 Furthermore, two-thirds of new TB cases occurred in 8 countries among the 30 high-TB burden countries. 5 In the Eastern Mediterranean Region (EMR), TB kills 136,000 people and affects 630,000 more every year accounting for 8.1% of the global TB burden.6,7 The EMR is the host to some of the world’s biggest emergencies and protracted crises and it carries the largest burden of displaced populations globally. 8 In 2020, the WHO estimated that the TB incidence rate was 112 per 100,000 population and the estimated number of deaths was 80,000 in the region. 8 The WHO and the international TB community consider TB in such complex emergencies a major challenge for control of the disease in the affected country or area, and beyond. 9 According to the WHO, the incidence of TB in Jordan was four cases per 100,000 people in 2021 and the case detection rate (% of confirmed and clinically diagnosed cases) was reported at 47%. 10 The Jordan National Tuberculosis Program (NTP) reached the Millennium Development Goal for TB reduction in 2011 and was preparing to shift to TB elimination. However, TB elimination planning has been disrupted due to the influx of Syrian refugees. 11 Since 2011, the Syrian crisis resulted in a regional humanitarian emergency with 5.6 million refugees, including 670,637 in Jordan. 12 The majority (80.6%) of Syrian refugees in Jordan are integrated into host communities (Urban refugees) and the rest are residing in camps. 13 Those refugees access the United Nations High Commissioner for Refugees (UNHCR)-sponsored clinics or Jordan Ministry of Health clinics, including TB diagnosis and treatment. 11 Beside the influx of Syrian refugees, Jordan has always been a destination for migrant workers. 14 Jordan had to cope with massive influx of people escaping conflict areas due to its strategic location between two major areas of instability and protracted conflict in the Middle East. 14 According to UNHCR, Jordan was hosting 67,000 Iraqis, 15,000 Yemenis, 6000 Sudanese, and 2500 refugees from a total of 52 other nationalities in 2019. 15
The burden of TB in Jordan is difficult to be assessed due to the lack of high-quality data, under-reporting, and lacking good-quality vital registration system. 16 The International Organization for Migration (IOM) began a program to support NTP in detecting and treating TB among refugees in 2012. 17 This support was in collaboration with UNHCR, the WHO, and United States Centers for Disease Control and Prevention. The goal 3 under the Sustainable Development Goals identifies ending the TB epidemic by 2030 under target 3. 18 Detecting and treating TB cases with the aim of increasing TB treatment coverage is a major component of the End TB Strategy. 2 However, despite ongoing efforts, there remains a significant gap between the number of notified and incident cases. 16 A better understanding of community-level knowledge, attitude, practices (KAP), and other issues related to TB such as stigma, discrimination, and healthcare-seeking behavior among Jordanians, refugees, and migrants can help the NTP in implementing evidence-driven activities as part of its obligation to control TB in Jordan. Therefore, this study aimed to assess TB-related knowledge, attitude, and behaviors among refugees, migrants, and general population as well as assess their stigmatizing and discrimination attitudes toward TB patients, their social behavior toward TB, and their healthcare-seeking behaviors. Including refugees and migrants in our study is important because they are the most affected populations at risk of developing TB and their arrival to Jordan can affect TB control efforts in the country. 19
Methods
Study design
A cross-sectional survey was conducted during the period of June to September 2021 among Jordanians (host population), Syrian refugees, and migrants living in four governorates including Amman, Zarqa, Mafraq, and Irbid. Syrian refugees included camp refugees living in Zaatari camp and those who are living outside refugee camps (Urban refugees). Migrants included those who live permanently or temporarily in Jordan “by choice” whether for work, education, or any other reason. The selection of the four governorates was based on criteria related to the presence of Syrian refugees in host communities. Almost 89.7% of Syrian refugees live in these governorates; 198,148 (29.6%) in Amman governorate, 167,191 (25%) in Mafraq, 136,820 (20.4%) in Irbid, and 98,254 (14.7%) in Zarqa. 13
Assuming that 50% of participants in each study group have a high TB-related knowledge with 5% absolute precision and confidence level of 95%, the estimated sample size was calculated at 385 per study group. The proportion of 50% was assumed to yield the largest possible sample size. To have adequate power to conduct subgroup analysis, the number of participants was increased to 2302 persons.
Sampling and data collection
For Jordanians, a two-stage cluster sample of households was selected using the 2015 census frame. The sampling units in the first stage included clusters in the four governorates. The second stage of household selection involved choosing a random sample of households from each cluster using systematic sampling technique. For each selected household, one eligible adult resident (⩾18 years) was randomly selected. For urban Syrian refugees, the UNHCER databases were used to identify clusters of Syrian refugees in each governorate. A random sample of clusters was selected. From each selected cluster, a systematic random sample of households was selected. For camp Syrian refugees, a systematic random sample of households/prefabs was selected from each district in the Zaatari camp. Migrants were identified from those attending the health centers for obligatory testing for the purpose of work permits. In addition, a sample of migrants was selected after mapping the places where migrants work (agricultural, industrial, factories, etc.) in the four governorates. A cluster sample of work settings and migrants within these settings was randomly selected. For data collection, a structured questionnaire was used to collect the data face-to-face. For host community, urban refugees, and migrants, trained research assistants visited the selected households in the four governorates. For each selected household, one eligible adult resident (⩾18 years) was randomly selected to fill the survey. A household was visited at least two times before we marked it as “Not at home.” If the house is uninhabited, the next household was selected. For camp refugees from Zaatari camp, three trained research assistants, who were Syrian activists with a medical background, visited the selected households/prefabs and interviewed one eligible adult from each household.
Study questionnaire
A structured questionnaire was developed and adapted based on the previous work in other countries,20–23 the WHO TB prevalence survey handbook, 24 and the WHO sample advocacy, communication and social mobilization, KAP survey questionnaire. 25 The questionnaire was prepared in English and was translated to Arabic using backward forward translation method. The questionnaire was checked for clarity, consistency, and cultural acceptability. After pilot testing on 30 persons and subsequent modification, the questionnaire was used to collect the data using face-to-face interviews. The questionnaire was divided into sections including sociodemographic characteristics, TB knowledge and awareness, attitude, stigma, discrimination, social behavior toward TB, and healthcare-seeking behavior. For TB knowledge and awareness section, the questions covered knowledge about the TB cause, mode of transmission, signs and symptoms, prevention, and treatment of TB. One question was added to determine the sources of TB information. The correct response to each question was scored “1” and incorrect response was scored “0.” Then the correct responses to questions were summed and divided by the number of items to generate a knowledge score. Likewise, the scores were generated for the subscales of knowledge about TB. For attitude, it was assessed by a group of questions with four Likert-type scale responses (strongly agree, agree, disagree, and strongly disagree). 26 An answer consistent with positive attitude toward the disease and to a person with TB was scored “1.” An answer not consistent with the positive attitude toward the disease and to a person with TB was scored “0.” The responses to questions were averaged to generate an attitude score, with higher score indicating positive attitude. Stigma was defined as an attitude or belief within Jordan cultural setting that discredits/devalues an individual with TB. 27 Questions were used to assess the social control applied by labeling, marginalizing, stereotyping, excluding, and exercising power over TB patients. An answer consistent with stigmatizing attitude toward the disease and to a person with TB was scored “1.” An answer not consistent with stigmatizing attitude toward the disease and to a person with TB was scored “0.” The responses to questions were averaged to generate stigmatizing attitude score on 100% scale, with higher score indicting higher stigmatizing attitude. For assessing discrimination, questions were used to assess how people with stigmatizing attitudes deny/prevent others of their rights and life opportunities by excluding or marginalizing them. 22 An answer consistent with discriminating attitude toward the disease and to a person with TB was scored “1.” An answer not consistent with discriminating attitude toward the disease and to a person with TB was scored “0.” The responses to questions were averaged to generate stigmatizing attitude score, with higher score indicating higher discriminating attitude. The social behavior toward TB questions was used to assess the participants’ feeling regarding supporting TB patients, their reactions if infected with TB, and whom to talk to about the illness. Finally, healthcare-seeking behavior was assessed by questions asking about the willingness to go to the health facility and plan for timely visit to a health facility if respondents thought they had TB symptom.
For calculation of the scales’ scores, we first dichotomized the items within each scale, reversed the codes for some items, and added the scores to get the overall scale score on 100% scale. The average score for each scale was categorized using Bloom’s cutoff point. 28 Based on the sum scores, level of knowledge was classified into low-level knowledge (less than 60%), moderate-level knowledge (60%–80%), and high-level knowledge (80%–100%). Meanwhile, the attitude scores were classified into positive attitude (80%–100%), neutral attitude (60%–80%), and negative attitude (less than 60%). Subsequently, level of practice was classified into poor (less than 60%), fair (60%–80%), and good practices (80%–100%). Similarly, stigma and discrimination were categorized into low, moderate, and high levels.
Ethical approvals
The ethical approvals were obtained from the Institutional Review Board (IRB) at Ministry of Health on March 30 2021 (the IRB approval No. MoH/Rec/2021/056). Written informed consent was obtained from each participant. Participation remained anonymous and data were treated with confidentiality.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences version 22. Percentages, means, and standard deviations were used to describe study variables. The results related to knowledge, attitude, behaviors, stigma, and discrimination were presented separately for each study group (Jordanians, refugees, and migrants). Chi-square was used to compare the sociodemographic characteristics between the study groups (Jordanian, urban refugees, camp refugees, and migrants). The general linear model (GLM) analyses were conducted to determine factors associated with scales’ scores. The variables included in the multivariate models were gender, age, study group, marital status, education, employment, and borrowing money in the last month. All variables, including nonsignificant variables, were left in the models (full model). A p value of less than 0.05 was considered statistically significant.
Results
Participants’ characteristics
Of a total 2450 persons invited, 2302 (94.0%) persons (1229 (53.4%) males and 1073 (46.6%) females) participated in this study. A total of 2075 persons (90.1%) reported that they have ever heard of TB, and they completed the whole questionnaire. Of those, 595 were Jordanians, 540 were urban refugees, 498 were camp refugees, and 442 were migrants. More than half of Jordanians (58%) and Syrians (55.1%), and 65.6% of migrants were aged 25–45 years. Almost two-thirds of Jordanians (61.2%) and urban refugees (65.4%) and more than three-quarters of camp refugees (74.5%) and migrants (79.9%) were married. The Jordanian sample was more educated than the other groups, where 52.9% (n = 315) of Jordanians had education higher than high school compared to 22.2% (n = 120) of urban refugees, 20.7% (n = 103) of camp refugees, and 34.6% (n = 153) of migrants. The majority (82.4%, n = 364) of the participated migrants were employed and less than half of other groups including 47.2% (n = 281) of Jordanians, 42.6% (n = 230) of urban Syrians, and 38.8% (n = 193) of camp migrants) were employed. Table 1 shows the sociodemographic and other related characteristics of the 2075 participants who were aware of TB and completed the survey.
The sociodemographic characteristics of 2075 participants who were aware of TB from different target groups.
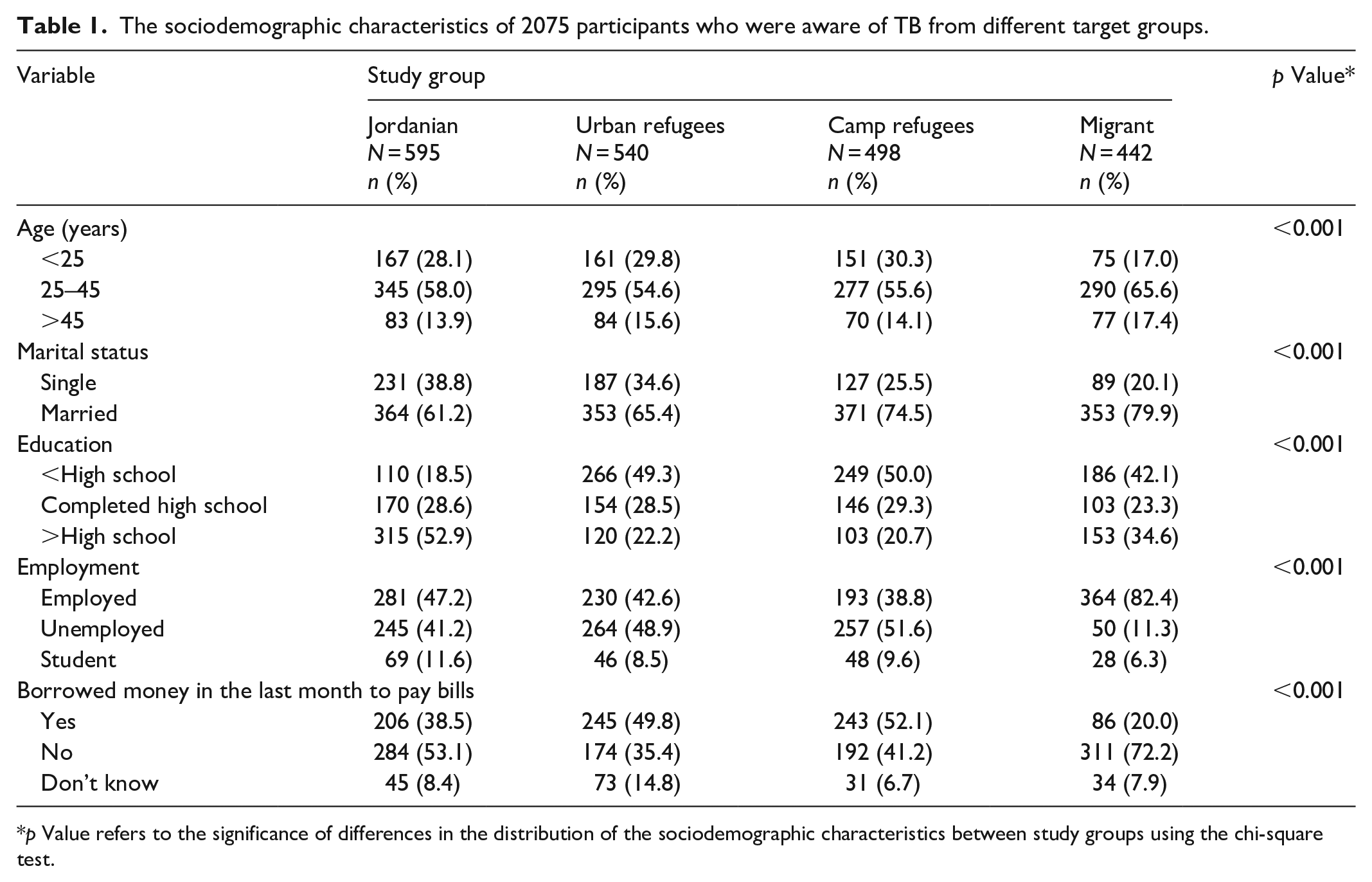
p Value refers to the significance of differences in the distribution of the sociodemographic characteristics between study groups using the chi-square test.
TB knowledge and awareness
For TB knowledge, 90.1% (2075 out of 2302 participants) reported that they have ever heard of TB. Radio and family, friends, neighbors, or colleagues were the most reported sources of information about TB among Jordanians and Syrians, while internet websites were the main source of information for migrants. Among those who have ever heard of TB, almost one-third of Jordanians (31.4%), urban refugees (36.3%), camp refugees (34.5%), and one-quarter of migrants (25.6%) knew that TB is a bacterial infection. The majority (91.8%) of camp refugees stated that they know the signs and symptoms of TB, while almost two-thirds of each of the other groups (77.1% of migrants, 75.7% of urban refugees, and 68.2% of Jordanians) reported that they know TB signs and symptoms. Respectively, 64.4%, 59.1%, 77.3%, and 68.6% of Jordanians, urban refugees, camp refugees, and migrants, reported that TB is a curable disease. Furthermore, 47.5% of Jordanians, 47% of urban refugees, 36.0% of camp refugees, and 35.7% of migrants believe that TB is a very serious disease. Table 2 shows the TB awareness among different targeted groups.
Awareness of TB among Jordanians, urban refugees, camp refugees, and migrants in Jordan.

Using knowledge scales, 88.9% of Jordanians, 92.8% of urban refugees, 92% of camp refugees, and 90.5% of migrants had low level of TB-related knowledge. One-third (37.6%) of camp refugees had high level of knowledge about TB signs and symptoms while 22.7% of Jordanians, 21.5% of urban refugees, and 26.5% of migrants had high level of knowledge about TB signs and symptoms. Furthermore, the majority (84.2% Jordanians, 86.3% urban refugees, 89.8% camp refugees, and 81.4% migrants) had low level of knowledge regarding TB transmission. Table 3 shows the detailed level of knowledge about different aspects of TB among each group.
Level of knowledge about different aspects of TB among Jordanians, urban refugees, camp refugees, and migrants in Jordan.
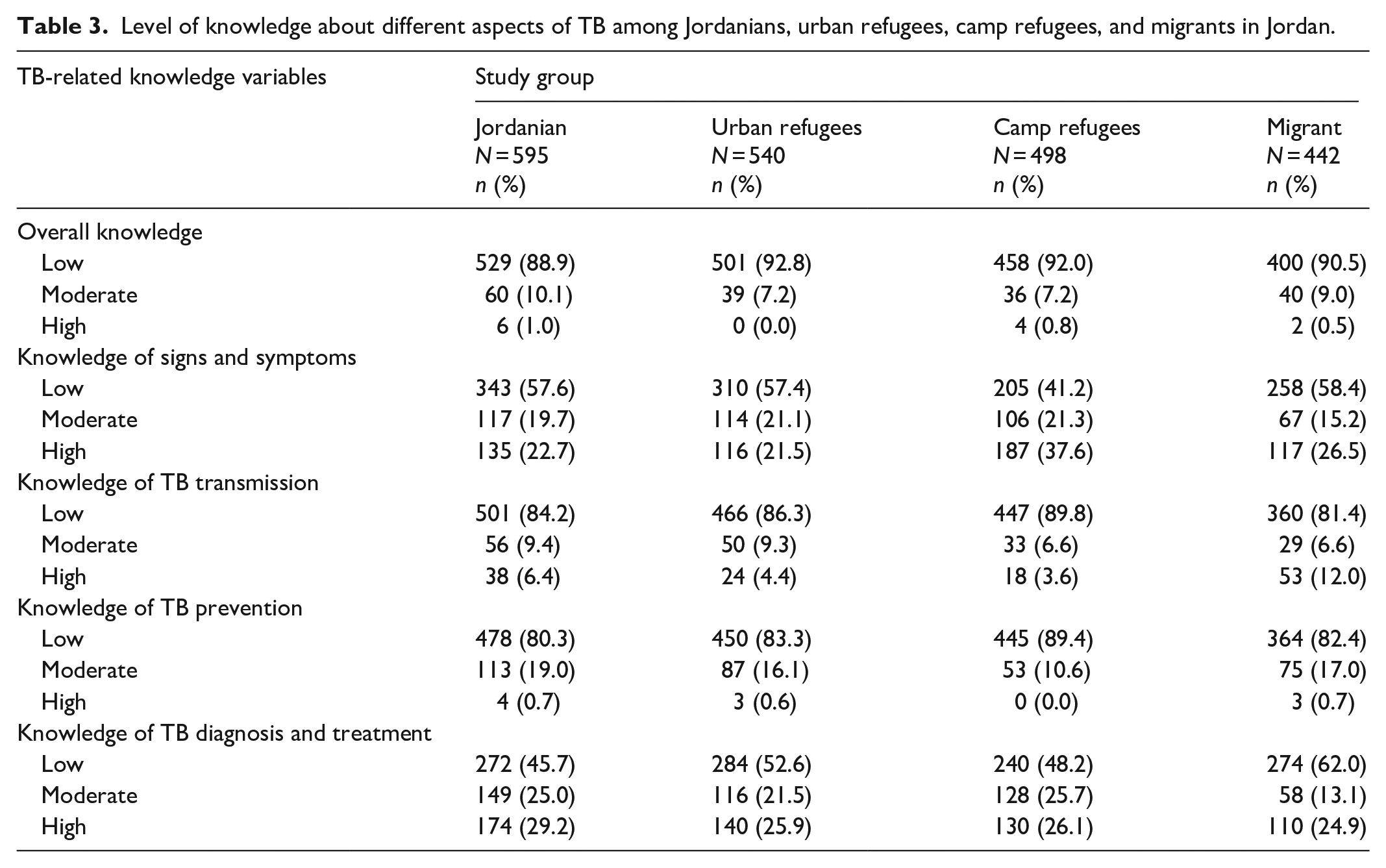
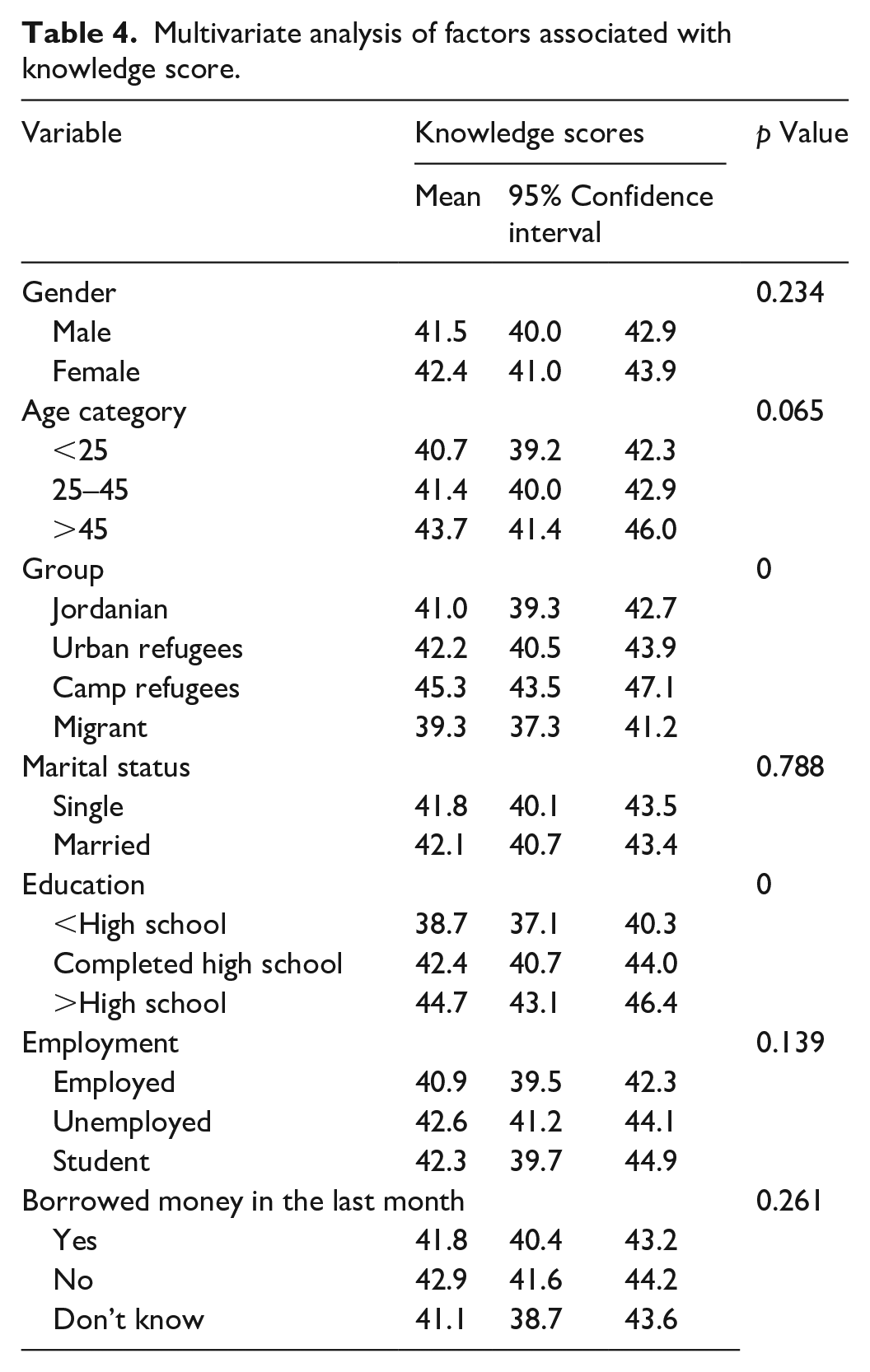
Table 4 shows the multivariate analysis of factors associated with knowledge score. The average knowledge score was the highest among camp refugees and the lowest among migrants. Those with higher educational levels had a significantly better overall knowledge regarding TB. Gender, age, marital status, employment, and having financial constraints were not significantly associated with knowledge score after adjusting for other variables in the model.
Multivariate analysis of factors associated with knowledge score.
Attitude
According to the attitude scale, 68.9% of Jordanians, 71.7% of camp refugees, 64.3% of urban refugees, and 56.6% of migrants had a positive attitude toward TB and patients with TB (Figure 1). Positive attitude included willingness to help and support TB patients, being open to be examined for TB if there is a relative patient with TB, believing that patients with TB should have the same rights to go to school or work as other people.

Attitude toward TB and patients with TB among Jordanians, urban refugees, camp refugees, and migrants in Jordan.
In the multivariate analysis of factors associated attitude toward TB and patients with TB, migrants had a significantly lower attitude score (indicating negative attitude) than the other groups. Employed people tended to have higher attitude score than unemployed participants and students (Table 5). Other studied variables were not significantly associated with attitude scores after adjusting for other variables in the model.
Multivariate analysis of factors associated with attitude scores.

Stigma
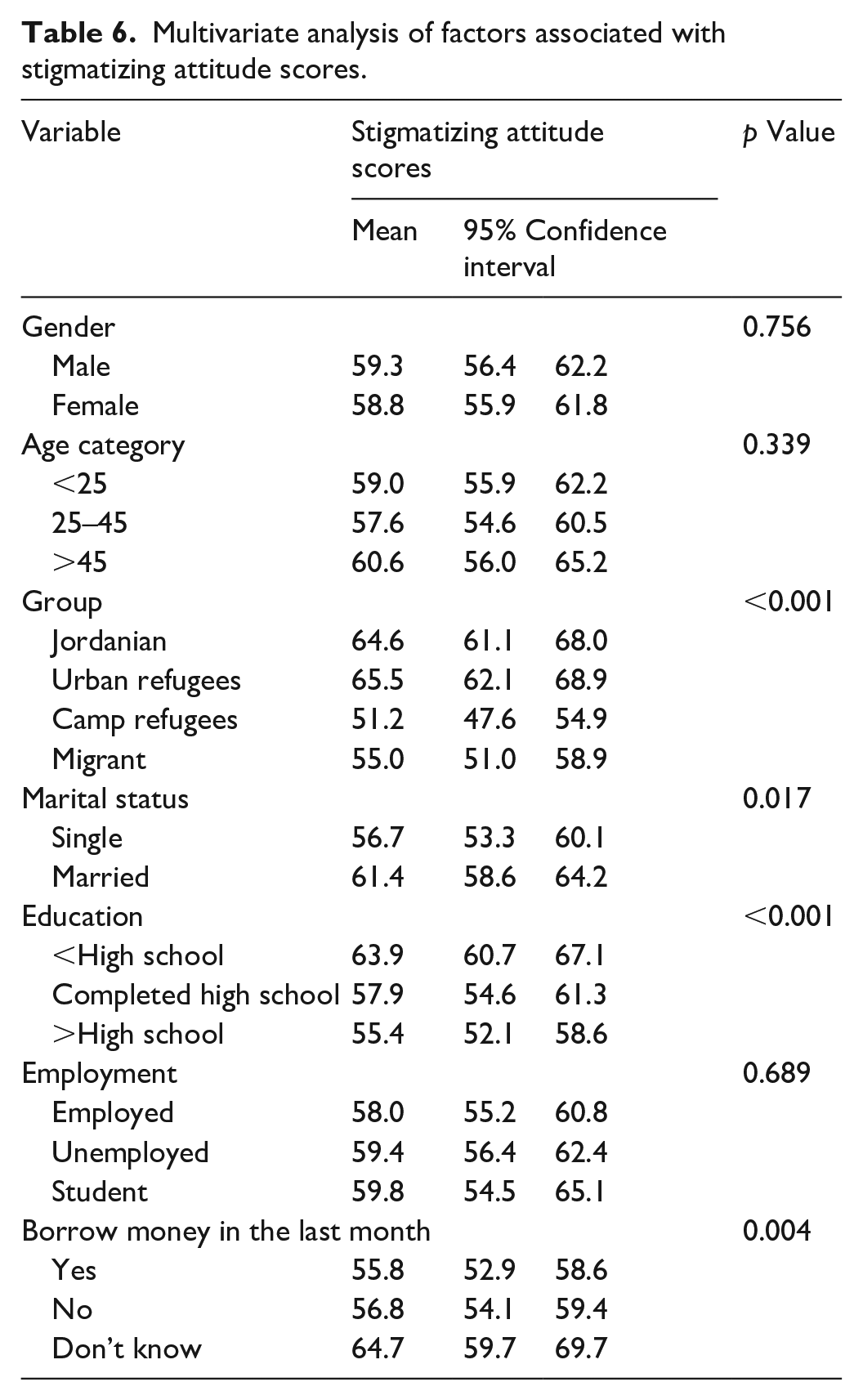
About 62.0% of urban refugees, 54.8% of Jordanians, 43.0% of camp refugees, and 55.4% of migrants (55.4%) had moderate to high stigmatizing attitude toward TB patients. The stigmatizing attitude included feeling scared of dealing with TB patients, staying away from TB patients, refusing to eat with TB patients, feeling that TB patients should be isolated and not go to work or school, and thinking of that other nationalities with TB should not enter Jordan. The association of stigmatizing attitude score with gender, age, study group, marital status, education, employment, and borrowing money in the last month was analyzed using the GLM procedure (Table 6). In this analysis, Jordanians and urban refugees had significantly higher scores of stigmatizing attitude than camp refugees and migrants. Moreover, married participants had significant higher scores of stigmatizing attitudes than single participants. Participants with lower educational level (<high school) had significantly higher scores of stigmatizing attitudes than participants with higher educational levels.
Multivariate analysis of factors associated with stigmatizing attitude scores.
Discrimination
About 15.1% of Jordanians, 10.6% of urban refugees, 23.7% of camp refugees, and 16.1% of migrants had moderate to high level of discriminating attitude toward patients with TB. We found that most participants had a low level of discriminating attitude toward patients with TB. Most of them had no problem sharing a meal with a TB patient, live in the same environment as TB patients or to let their children or other relatives play with TB patients’ children, and work in the same office as TB patients. The association of discriminating attitude score with gender, age, study group, marital status, education, employment, and borrowing money in the last month was analyzed using the GLM procedure (Table 7). Camp refugees had significantly higher level of discriminating attitude toward patients with TB than the other groups. Participants with higher educational levels and who were employed had higher level of discriminating attitude toward patients with TB than the other groups. Other studied variables were not significantly associated with discriminating attitude scores after adjusting for other variables in the model.
Multivariate analysis of factors associated with discriminating attitude scores toward TB and patients with TB.

The social behavior toward TB
While 42.9% of Jordanians, 40.7% of urban refugees, 52.0% of camp refugees, and 48.0% of migrants reported that they feel compassion and desire to help people with TB, 29.7%, 27.4%, 33.7%, and 27.4% of them, respectively, feel the same but tend to stay away from those people. On the other hand, 27.9% of Jordanians, 29.4% of urban refugees, 16.3% of camp refugees, and 21.5% of migrants reported that their communities reject TB patients. When participants were asked about their reaction if they were found to have TB, 77.3% of Jordanians, 72.7% of urban refugees, 74.6% of migrants, and 59.4% of camp refugees stated that they will be surprised. However, only 12.9% of camp refugees answered that they will feel ashamed and 20% of them answered that they will be embarrassed if they were found to have TB. The majority of participants (90.4% of Jordanians, 89.2% of urban refugees, 93.3% of camp refugees, and 87.5% of migrants) stated that they will tell their doctors and other healthcare providers if they have TB. Moreover, more than two-thirds of participants among all groups reported that they will tell their spouse or parents if they are infected.
Healthcare-seeking behavior
While almost two-thirds (65.5%) of the Jordanian participants had medical insurance, only 33.3% of urban refugees, 30.3% of migrants, and 19.9% of camp refugees did. Most of participants among all groups (90.9% camp refugees, 82.1% Jordanians, 76.6% urban refugees, and 74.7% migrants) stated that they would go to a health facility if they thought they had symptoms of TB. Furthermore, 83.3%, 73.8%, 67%, and 72.4% of camp refugees, Jordanians, urban refugees, and migrants, respectively, would seek help as soon as they realize that their symptoms might be related to TB. About 52.2% camp refugees, 45.2% urban refugees, 44.7% Jordanians, and 74.7% migrants reported that they feel well-informed about TB and the majority (89.5% camp refugees, 83.7% migrants, 76.1% urban refugees, and 75.8% Jordanians) wish to get more information about TB.
Discussion
This study identified significant gaps in TB knowledge among the four targeted groups. The level of knowledge of signs and symptoms, transmission, and treatment of TB was inadequate among all studied groups. The overall knowledge about TB among all targeted groups was lower than what was reported in other surveys.20,29–31 One study from the region in Iran found that 62% of participants had good knowledge about TB. 31 Studies in the EMR reported variable TB-related knowledge levels. In a study conducted in Al-Anbar Governorate in Iraq, only 10.6% of study participants had good knowledge of TB. 32 A study in Saudi Arabia reported higher level of TB-related knowledge; 25.1% of participants had good knowledge regarding TB. 33 Other studies that investigated TB KAP among underprivileged groups such as immigrants and refugees also revealed limited knowledge with variety of misperceptions about TB symptoms and transmission.34,35
Our study showed that the average knowledge score was significantly higher among camp refugees. This might be a result of receiving further information about TB through the educational programs or counseling that are usually provided for refugees from different organizations at camps such as IOM and UNHCR. In 2013, it was reported that 300,000 refugees benefited from TB awareness raising, active TB screening, referrals for further investigations and treatment, and directly observed treatment follow-up. 36 There was a significant association between TB-related knowledge and educational level. Regardless of the target group, the average knowledge score was significantly higher among respondents with higher educational levels. The same finding of the association between education and TB-related knowledge was reported in other studies conducted in different countries.20,30,37,38
The majority of respondents had a positive attitude toward TB. This finding is consistent with the findings of other studies29,30,38 and not consistent with the findings of few studies.20,39 Migrants had a significantly lower score of positive attitudes than the other groups. This might be explained by the fact that all migrants must be regularly screened for TB as a residency requirement in Jordan and they might be afraid to be deported if diagnosed with TB. As expected, participants who were employed tended to have higher positive attitude than unemployed participants and students. Employed participants are most likely to have higher educational level than unemployed respondents and therefore more adequate TB-related knowledge which leads toward more positive attitudes. The same finding was reported by other investigators.38,40
Stigma is a social determinant of health and found to be a major barrier to accessing health care, which results in diagnostic and treatment delay. 41 For TB, the most common cause of stigma is the perceived risk of transmission from TB-infected individuals to susceptible community members. 42 This study showed that a considerable proportion of the study participants had moderate to high level of stigmatizing attitude toward TB patients. And this may contribute to the gaps in TB detection and treatment seen in Jordan.
As expected, participants with lower educational level.43–45 Jordanians and urban refugees had significantly higher scores of stigmatizing attitudes than camp refugees and migrants. Moreover, married participants had significantly higher scores of stigmatizing attitudes than single participants. Some studies did not support the association between sociodemographic characteristics and TB-related stigma.44,45 However, other studies showed variation in TB-related stigma between different social groups and communities.20,46,47 This suggests that improvement in TB awareness activities to reduce TB stigmatization is important for TB control efforts irrespective of the background and varieties of a population.
Discrimination is another social determinant of health where stigmatized individuals suffer discrimination and status loss at the hands of the broader community. 48 Camp refugees had a significantly higher discriminating attitude score toward patients with TB than the other groups. In some other studies, discrimination against TB patients was felt more strong in certain subpopulations, including women, refugees, individuals from rural areas, and people with lower education levels.44,49,50 Surprisingly, in our study, participants with higher educational levels and who were employed had higher level of discriminating attitude toward patients with TB than the other groups. Further and in-depth research is needed to explore and explain this relationship.
Only 40%–50% of participants reported that they feel compassion for TB patients and desire to help people with TB. The negative social behavior toward TB was mostly seen among camp refugees although they were found to have higher knowledge score than other groups. Almost half of our respondents stated that their communities are friendly, but they generally try to avoid people with TB. Similar findings were reported in other studies as fear of TB stigma can lead infected individuals to hide their TB status even from their own families.46,51 Moreover, such social behavior toward TB results in a sense of shame or guilt, leading to self-isolation as TB-infected individuals internalize their community’s negative judgments about the disease. 52 Luckily, this was not the case among our participants where the majority stated that they will talk with doctors and other healthcare providers about their TB illness. Moreover, more than two-thirds of participants among all groups reported that they will talk with their spouse or parents about their TB illness.
Most of our participants had positive healthcare-seeking behavior regarding TB. The majority of all groups stated that they would go to a health facility if they thought they had symptoms of TB to seek help as soon as possible. This positive healthcare-seeking behavior is essential as it helps to prevent missed opportunities for TB diagnosis and reduce the spread of TB.53,54 However, it is possible that reported healthcare-seeking behaviors might be different from actual actions and this might explain the inconsistency between our participants’ relatively negative social behavior and positive healthcare-seeking behavior. Furthermore, we found that only half of participants or less reported that they feel well-informed about TB and most of them (89.5% camp refugees, 83.7% migrants, 76.1% urban refugees, and 75.8% Jordanians) wished to get more information about TB. This finding underlies the importance of ensuring healthcare centers are adequately equipped, and health workers are adequately trained to facilitate early diagnosis and treatment of TB. 20
Adequate TB-related knowledge plays a significant role in promoting early detection, timely treatment-seeking behavior, and adherence to treatment. The reported gaps in TB-related knowledge among the study participants hinder TB control and prevention in Jordan since it might lead to a delayed diagnosis especially when symptoms are unrecognized. This might increase the risk of further transmission leading to more TB morbidity and mortality. Poor treatment adherence occurs from insufficient understanding of TB full treatment, fostering drug-resistant strains, and complicating control. Equally important, addressing attitude and discrimination issues enhances TB control efforts, leading to improved outcomes and reduced disease burden. The reported positive attitudes and low discrimination levels support effective control measures and might help overcoming barriers to care seeking and treatment adherence in Jordan.
The strength of this study was that it is the first national-level survey on TB-related knowledge, attitude, and behaviors in Jordan that explored different population groups. Our study provided valuable insights regarding knowledge of TB, stigma in the community and identified some areas requiring intervention by the national TB program and other stakeholders in the fight to control TB in Jordan. One of the main limitations of this study is that we did not use standardized tools to assess knowledge, attitude, stigma, and discrimination because such assessment tools are lacking. This would compromise the comparisons between our study population and other populations.
Conclusion
In conclusion, the study populations had significant gaps in TB-related knowledge. Although our findings indicate a general positive attitude and low level of discriminating attitude toward TB patients, moderate to high level of stigmatizing attitude was reported by a considerable proportion of the study participants. The poor knowledge on TB, negative attitude, and high level of stigmatizing attitude varied between the studied groups, level of education, and employment status. TB-focused health education interventions to close knowledge gaps and reach the most disadvantaged and affected communities in Jordan are highly needed. Raising awareness about TB will help to promote positive attitudes toward TB and TB patients.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231187743 – Supplemental material for Tuberculosis-related knowledge, behaviors, stigmatizing attitude, and discrimination among refugees, migrants, and the general population in Jordan
Supplemental material, sj-docx-1-smo-10.1177_20503121231187743 for Tuberculosis-related knowledge, behaviors, stigmatizing attitude, and discrimination among refugees, migrants, and the general population in Jordan by Majd A Alsoukhni, Yousef Khader, Hiba Abaza, Nevin Wilson and Srinath Satyanarayana in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all individuals and organizations who have contributed to this research. Special thanks to the staff of Jordan national TB program for their invaluable guidance and support. We are grateful to the participants for their cooperation. Thanks to our colleagues, friends, and families for their encouragement.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication resulted (in part) from a project supported by the International Organization for Migration.
Ethics approval
Ethical approval for this study was obtained from the Institutional Review Board (IRB) at Ministry of Health on March 30, 2021 (the IRB approval no. MoH/Rec/2021/056).
Informed consent
Written informed consent was obtained from each participant. Participation remained anonymous and data were treated with confidentiality.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.