
Abstract
Background:
Upper extremity vascularized composite allotransplantation is a life-enhancing reconstructive treatment option that aims to improve recipients’ quality of life and maximize function. This study assessed upper extremity vascularized composite allotransplantation patient selection criteria perceptions among individuals with upper extremity limb loss. The perceptions of individuals with upper extremity limb loss on patient selection criteria may enable vascularized composite allotransplantation centers to improve criteria to avoid mismatched expectations about the posttransplant vascularized composite allotransplantation experience and outcomes. Realistic patient expectations may increase patient adherence, improve outcomes, and reduce vascularized composite allotransplantation graft loss.
Methods:
We conducted in-depth interviews with civilian and military service members with upper extremity limb loss and upper extremity vascularized composite allotransplantation candidates, participants, and recipients from three US institutions. Interviews assessed perceptions of patient selection criteria for suitability as a candidate for upper extremity vascularized composite allotransplantation. Thematic analysis was used to analyze qualitative data.
Results:
A total of 50 individuals participated (66% participation rate). Most participants were male (78%), White (72%), with a unilateral limb loss (84%), and a mean age of 45 years. Six themes emerged regarding upper extremity vascularized composite allotransplantation patient selection criteria, including support for candidates who: (1) are of younger age, (2) are in good physical health, (3) have mental stability, (4) are willing to “put in the work,” (5) have specific amputation characteristics, and (6) have sufficient social support. Patients had preferences about selecting candidates with unilateral versus bilateral limb loss.
Conclusions:
Our findings suggest that numerous factors, including medical, social, and psychological characteristics, inform patients’ perceptions of patient selection criteria for upper extremity vascularized composite allotransplantation. Patient perceptions of patient selection criteria should inform the development of validated screening measures that optimize patient outcomes.
Keywords
Introduction
Upper extremity (UE) vascularized composite allotransplantation (VCA) is an innovative treatment option for people with UE limb loss. UE VCA may provide functional, psychosocial, and aesthetic benefits to individuals with UE limb loss. To date, over 150 UE VCA procedures have been performed globally; 37 in the United States. 1
While solid organ transplantation is a life-saving procedure, UE VCA is a life-enhancing procedure that involves significant health risks associated with surgery and lifelong immunosuppression. 2 UE VCA requires rigorous and prolonged rehabilitative therapy to regain function and strict adherence to an immunosuppressive regimen. UE VCA is both a physically and psychologically demanding procedure that necessitates proper patient selection.
UE VCA recipients who experience complications during the posttransplant period, such as body image distortion and psychiatric challenges, may find it difficult to adhere to their immunosuppression or rehabilitation regimen leading to an increased risk of rejection and graft loss.3,4 Several UE VCA programs have reported psychiatric complications (i.e., depression, anxiety, drug/alcohol abuse) and nonadherence to immunosuppression and rehabilitation among transplant recipients. 5 Instances of immunosuppression nonadherence highlight the importance of patient selection and psychosocial suitability for VCA. Therefore, candidates considering UE VCA undergo an extensive evaluation process that involves physical, psychological, and social assessments to assess a patient’s ability to adapt to the challenges of posttransplant life.5,6
Some VCA clinicians have proposed that particular patients may be better suited psychosocially to VCA than others. 7 Patient selection is the process by which potential patients are selected or not selected for a medical procedure based on predetermined criteria. Patient selection is a complex process critical to the success of UE transplantation. The psychosocial evaluation protocol and assessments used for patient selection are not standardized and vary across transplant centers. 5 Inadequate patient selection screening protocols have been associated with poor outcomes in UE VCA recipients. 8
A myriad of patient selection characteristics (e.g., physical, psychosocial, anatomical health) are assessed in individuals with UE limb loss. 9 Prior research has recommended patient selection criteria based on age and adapting to life with limb loss. 10 Healthcare providers have reported an increased likelihood of selecting patients with bilateral amputations or loss of the dominant hand. 2 Few qualitative studies have identified psychosocial factors for suitable candidates, including setting realistic treatment expectations and coping with graft failure. Transplant providers have identified social support and the recipient’s prior experiences, behaviors, and characteristics as predictors of UE VCA success. 11
As efforts to standardize UE VCA patient selection criteria are advancing, we sought the perspectives of individuals with UE amputations, given their unique lived experiences, to aid in developing criteria which optimize patient-centered outcomes. The lived experiences of individuals with UE limb loss provide the necessary insight into the functional and psychosocial adaptations that the patients make after limb loss, enabling them to identify characteristics that may make someone a suitable candidate for UE VCA. Perceptions of patient selection criteria are needed from adults with UE limb loss because this population has vast anatomical heterogeneity (i.e., unilateral or bilateral, above elbow, or below elbow) that can influence their perceptions. A standardized approach may reduce medication nonadherence, noncompliance with rehabilitation practices, and other posttransplant complications. Patients’ experience, particularly UE VCA recipients, is an underutilized resource for improving UE VCA. 12 This study examines patients’ perceptions of patient selection criteria, including identifying factors that would make someone a good candidate or not a good candidate for UE VCA among individuals with UE limb loss.
Methods
Study design
We conducted a multisite, cross-sectional qualitative study involving in-depth interviews about perceptions of patient selection criteria among people with UE limb loss. We used the Consolidated Criteria for Reporting Qualitative Research for quality reporting of qualitative studies. 13
Setting
The study was conducted at Northwestern University (NU) in Chicago, IL; Johns Hopkins University (JHU) in Baltimore, MD; and Walter Reed National Military Medical Center (WRNMMC) in Bethesda, MD. The Shirley Ryan AbilityLab in Chicago, IL and David Rotter Prosthetics, LLC in Joliet, IL, supported recruitment for NU. The Institutional Review Boards approved the study at: NU (STU00209718), JHU (00225728), and WRNMMC (WRNMMC-EDO-2020-0432). NU served as the Institutional Review Board of record for WRNMMC but not for JHU.
Participants and recruitment
The inclusion criteria included: English-speaking adults (18–65 years) with an acquired UE amputation. Eligible participants included both civilians and military service members, individuals who never pursued UE VCA, UE VCA candidates (i.e., individuals who contacted a transplant center to express interest in pursuing UE VCA), UE VCA participants (i.e., individuals who began UE VCA evaluation), and UE VCA recipients. Exclusion criteria included: individuals who were cognitively impaired and/or had congenital limb loss.
Eligible participants at each study site were either mailed and/or emailed a letter describing the study. One week later, follow-up phone calls were made to screen the potential participants for eligibility. Potential participants were also recruited via study flyers through support groups and social media websites. Those who expressed interest were contacted through telephone to be screened for eligibility. All participants provided verbal informed consent.
Data collection
We conducted in-depth interviews from July 2020 to March 2022 to assess participants’ perceptions of patient selection criteria for UE VCA as part of a more extensive study on decision-making and informed consent for UE VCA. Interviews were conducted through telephone by the research team (BK, KV, MD, MN) trained by the Principal Investigator (EJG), a qualitative research expert. The interview guide was developed by an interdisciplinary research team comprised of ethicists, social scientists, and UE VCA clinicians/surgeons. Cognitive interviews were conducted with five participants (BK) to revise the wording and improve the clarity of in-depth interview questions. 14 Interviewers did not have prior established relationships with the study participants.
In-depth interviews included four open-ended questions about perceptions of patient selection criteria and factors that make someone a good candidate or not a good candidate for UE VCA. Participants were asked; (1) “Now think broadly about people with amputations, in general. What makes someone a good candidate for upper limb transplantation?”; (2) “Probe: What makes someone not a good candidate for upper limb transplantation?”; (3) “Probe: Physical/bodily characteristics, medical, psychological, emotional, social?”; (4) “Transplant teams evaluate patients when they have one or two amputation(s). Do you think the kind of amputation, one or two, matters for whether a patient should be selected for an upper limb transplant?” At the beginning of the interview, the interviewer briefly described UE VCA, including its definition, purpose, risks, and potential benefits. We did not provide information about patient selection criteria practices to elicit patients’ perceptions using emic terminology that was not influenced by the research team’s language to stay grounded in understanding their point of view.
Interviews also included questions about sociodemographic characteristics (e.g., age, health status, date of amputation) and health literacy (“How often do you need someone to help you when you read instructions, pamphlets or other written material from your doctor of pharmacy?” anchored by “Never” and “Always”; response options of “Never” and “Rarely” were reflected as adequate health literacy). Interviews lasted, on average, 78 minutes (range: 37–140) and were audio recorded and transcribed. Participants were compensated with a $35 gift card.
Qualitative analysis
Interview transcripts were analyzed for emerging themes using the constant comparison, inductive, and deductive coding methods.15,16 An initial codebook was established using deductive codes based on interview guide question domains (e.g., Patient Selection). The team then developed inductive codes by iteratively reviewing and open coding 2–5 transcripts at each study site. The team resolved coding discrepancies through discussion and iteratively refined codebook definitions until reaching thematic saturation.17,18 After finalizing the codebook, two research team members at each study site (JG-S, BK, MD, KV, MN, ML) independently coded the transcripts using NVivo (Lumivero) and established an inter-rater reliability (Kappa > 0.80). 19 Thereafter, research team members coded all interview transcripts and resolved discrepancies through discussion. Team members reviewed the coded transcript excerpts across interviews to identify patterns and themes and wrote analytical summaries for each code.
Results
Demographics
A total of 50 respondents participated (64% participation rate). Sixteen participants were from NU, 17 from JHU, and 17 from WR (Table 1). Most participants were male (78%), White (72%), with a unilateral amputation (84%), and had a mean age of 45 years. The mean number of years since participants’ first amputation was 10 years.
Participants’ sociodemographic and clinical characteristics (N = 50).

Abbreviation: SD, Standard Deviation; VCA, vascularized composite allotransplantation.
“Other” included people who identified as Hispanic or Mexican (n = 3), Did not specify (n = 1).
Percentages do not add up to 100 because some participants did not respond.
Percentages add up to greater than 100 due to more than one response from some participants.
Some participants had multiple surgeries for their amputation or multiple amputations, therefore, we used the time between the date of the first amputation surgery and the date of the interview for analysis.
Participants from locations not specific to a study site who reached out to the NU team were analyzed as “NU” participants.
Themes
We identified six themes regarding UE VCA patient selection criteria, including support for candidates who: (1) are of younger age, (2) are in good physical health, (3) have mental stability, (4) are willing to “put in the work” of rehabilitation, (5) have specific amputation characteristics, and (6) have sufficient social support. Table 2 presents illustrative representative quotations.
Representative illustrative quotations about perceptions of patient selection criteria for UE VCA by major theme and subtheme. a .
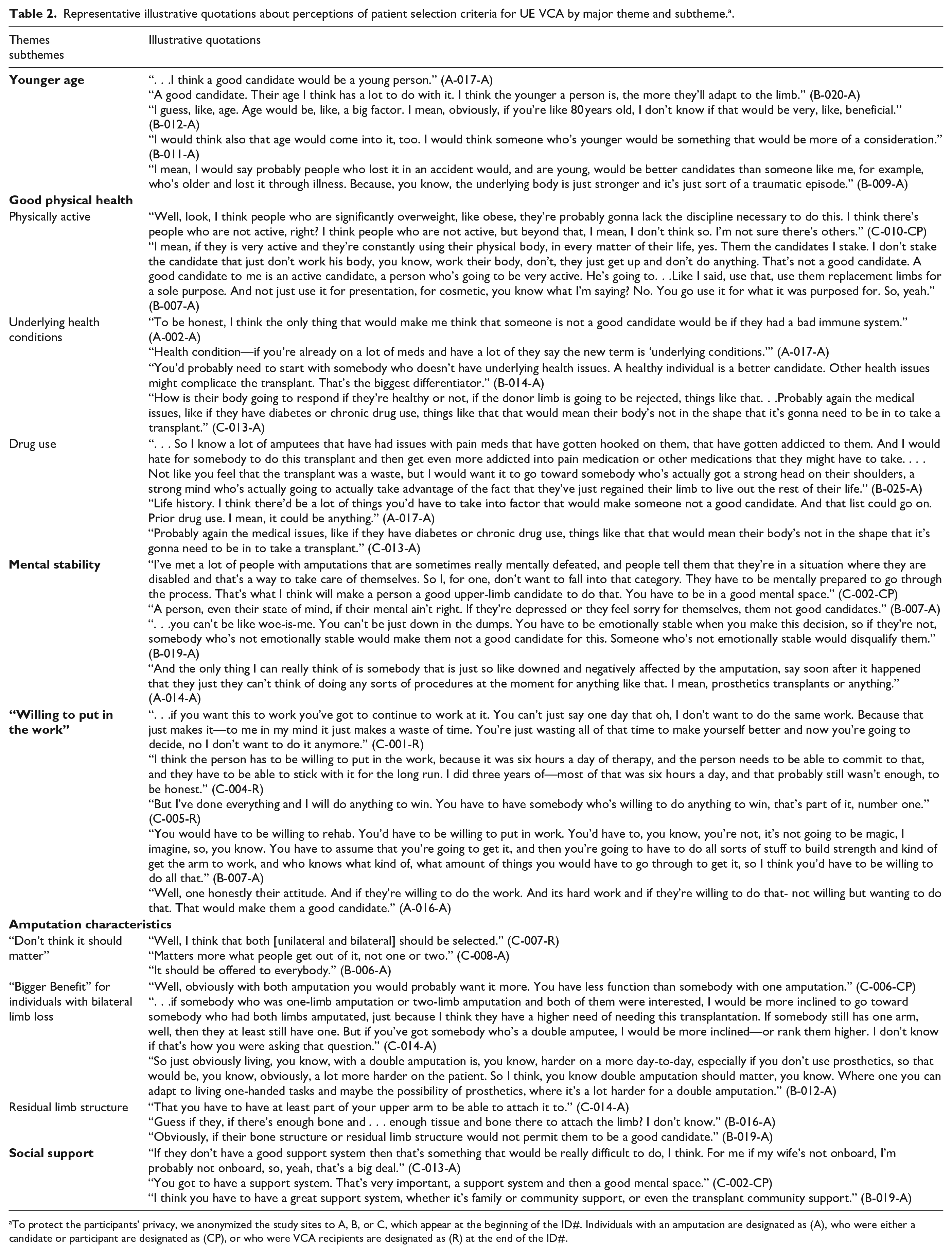
To protect the participants’ privacy, we anonymized the study sites to A, B, or C, which appear at the beginning of the ID#. Individuals with an amputation are designated as (A), who were either a candidate or participant are designated as (CP), or who were VCA recipients are designated as (R) at the end of the ID#.
Younger age
Participants reported that a good candidate for UE VCA should be of a younger age. Participants commented that compared to older individuals, younger individuals would make good candidates because they would be better suited to adapt to changes required for life with a UE transplant. One participant stated: “A good candidate. Their age, I think, has a lot to do with it. I think the younger a person is, the more they’ll adapt to the limb” (B-020-A). Most participants recommended that candidates be youth or children. Alternatively, some participants raised concerns that older individuals, namely those over 50 years “might not live to see much benefit over time from the transplant.”
Good physical health
Participants provided input on how physical health or overall bodily characteristics would affect a person’s suitability as a candidate for UE VCA. Most participants identified suitable candidates as being “healthy,” in “good physical condition,” and having a “sound immune system” as primary factors associated with physical health and whether someone is a good candidate. One participant stated: “I think just being in good physical condition, too, would be another reason, make another good candidate” (B-011-A). Subthemes identified with being in good physical health included: physical activity, underlying health conditions, and drug use.
Physically active
A few participants identified physical activity as a factor associated with being a suitable candidate for UE VCA. Participants noted that individuals who are “active,” “work out,” and are “reasonably fit” are accustomed to “constantly using their physical body.” One participant stated: “I think, ideally, . . . somebody that works out, because then . . . they’re already used to using their body in that way and working to the point of failure. So somebody that’s active” (C-006-CP). Alternatively, a participant commented that individuals “who are significantly overweight” would likely “lack the discipline necessary to do [UE VCA].”
Underlying health conditions
Participants reported that individuals with “underlying conditions,” a “bad immune system,” or “preexisting conditions” would not be suitable candidates for UE VCA. Participants associated underlying health conditions with “poor health” and explained that health conditions could potentially adversely affect the health outcomes of UE VCA. Participants reflected on the potential of underlying conditions to “fight the transplant” or how the “body’s not in the shape that it’s gonna need to be in to take a transplant.” For example, “Well, like anything else, the additional advanced medical challenges will always make it more difficult for anyone to recover. So, if you know if someone has physical challenges that are beyond their amputation, that will make their recovery and their likelihood of being a qualified candidate less” (A-001-A).
Drug use
A few participants identified “prior drug use” and “chronic drug use” as factors that would make an individual with UE limb loss unsuitable to be a candidate for UE VCA. Participants perceived drug use as a factor associated with an individual not being physically and emotionally suitable for a transplant. Participants raised concerns about not knowing “how people are going to mentally respond to [UE VCA].” UE VCA is a physically and emotionally taxing procedure, and participants expressed concerns about individuals with a history of drug use ending “up in a worse position.”
Mental stability
Participants identified “stability” as an essential for being a suitable candidate for UE VCA, which they perceived as having emotionally accepted UE limb loss and not currently struggling with “mental health problems” such as depression or anxiety. Participants reported that candidates must be in a “good mental space,” “emotionally stable,” and “mentally strong” to make an informed decision to pursue UE VCA. Characteristics that participants associated with being suitable for UE VCA included having come to terms with UE limb loss and the ability to cope with stress. Individuals were not perceived as suitable candidates if they were “Somebody who is still not coping, I guess. Somebody who’s fragile, psychologically” (C-008-A). A history of “psychological problems” such as mood disorders (e.g., depression and anxiety) was identified as a characteristic that would make someone not a good candidate for UE VCA: “Mentally, I don’t think it would be good for someone who was chronically depressed or bipolar. There are a lot of ups and downs. Somebody not good at handling stress or setbacks.” (C-007-R).
“Willing to put in the work.”
Some participants, including all four UE VCA recipients, stated that good candidates for UE VCA must possess the “willingness to put in the work.” Participants described “put in the work” as an individual’s commitment to changing their life for UE VCA. Participants emphasized the importance of committing to the process, which includes long-term immunosuppression and rehabilitation. One recipient reflected on his experience and stated that individuals would be “wasting all of that time” if they do not “continue to work at it.” Another participant commented, “I think the person has to be willing to put in the work because it was six hours a day of therapy, and the person needs to be able to commit to that, and they have to be able to stick with it for the long run” (cite C-004-R).
Amputation characteristics
Participants reported that amputation characteristics, including amputation type (unilateral or bilateral), might affect a candidate’s status as a suitable candidate for UE VCA. Participants had conflicting views on the role of unilateral versus bilateral limb loss in patient selection. Three subthemes emerged regarding patients’ perceptions of patient selection criteria and amputation characteristics: laterality should not matter (i.e., individuals with one or two amputations should be eligible to receive UE VCA if they are suitable candidates); individuals with bilateral limb loss have more to gain from UE VCA; and suitability may be influenced by the residual limb structure.
Laterality does not matter
Nearly half of participants reported that individuals with either unilateral or bilateral limb loss should be eligible for UE VCA. As one participant stated, “One versus two shouldn’t be part of the equation. Doesn’t matter. If they want to get one, they should be able to” (N019-A).
“Bigger Benefit” for individuals with bilateral limb loss
Half of the participants reported that individuals with bilateral limb loss might have more to gain from UE VCA than those with unilateral limb loss. Participants explained that individuals with bilateral limb loss would be more likely to experience improved function and quality of life (QOL) than individuals with unilateral limb loss. For example, one stated: “I mean, it seems that someone who had two amputations, the ability to have one functioning arm. . . Like, going from zero to one to me seems like a lot bigger benefit than going from one to two” (B-009-A).
Residual limb structure
Participants also expressed concern about the state of the residual limb and the capacity for attaching a transplanted limb to the residual limb as factors affecting suitability. For example, participants questioned whether there was “enough tissue and bone” or if there has been “damage in the stump.” One participant stated, “I mean, obviously, if they had extenuating circumstances on their existing amputation. This bone’s messed up, so it might not work or something like that” (A-033-A).
Social support
Participants identified the importance of having a support system comprised of family and friends in candidate suitability for UE VCA. Participants related that pursuing UE VCA would be “really difficult” without a robust support system to rely on through the “good and the bad of [UE VCA].” Some participants remarked that they would not pursue UE VCA if their spouses were not supportive of the procedure: “in my case, my wife—I would want her to totally agree about the decision because it would have a major impact on her, especially for the first year of going through the surgery and the aftercare” (B-014-A).
Discussion
Our qualitative study identified factors that patients perceived to be important for the selection of candidates for UE VCA. These factors were anticipated to result in transplant success, improved function, and enhanced QOL.
A key factor that we identified was patient age, with younger individuals perceived as better candidates for UE VCA as they would be better able to adapt to living with a UE VCA than older individuals. Prior qualitative research corroborates this finding, in which respondents perceived younger individuals as being better able than older individuals to endure the complex UE VCA medical procedure, extensive rehabilitation, and lifelong immunosuppression. 10 However, the allocation of UE grafts to younger candidates does not necessarily decrease the likelihood of graft failure. Studies show that younger kidney recipients have a higher risk of graft loss due to nonadherence.20,21
Our study participants believed that preexisting medical conditions and physical activity were critical in determining candidacy. Participants’ perception that preexisting medical conditions would diminish the likelihood of a successful UE VCA aligns with the UE VCA patient screening practices utilized by transplant centers. 8 In addition to conducting extensive anatomical and physiological testing to determine a patient’s eligibility, transplant centers evaluate fitness and preexisting medical conditions and do not select UE VCA patients with medical conditions that could negatively affect surgical, functional, or immunomodulatory results. 8
We found that mental stability and a willingness to “put in the work” were psychological criteria that participants deemed necessary for successful UE VCA candidates. This finding coincides with prior research suggesting the importance of psychological and psychiatric assessments in selecting suitable candidates for transplantation due to the risk of adverse outcomes associated with psychiatric disorders.8,22,23 Psychiatric and psychological screening for UE VCA includes assessing an individual’s preparedness for transplantation, preexisting psychiatric illness, drug use, and coping mechanisms. 8 In addition, consistent with our study, other research on UE VCA providers and recipients found that adherence to the transplant protocol and self-motivation during rehabilitation is essential to patient selection and pivotal to the success of hand transplantation. 24
A key finding was the importance participants placed on a “good social support system” in determining a patient’s suitability for UE VCA. Other research with UE VCA recipients similarly identified the importance of a quality support system as recipients recounted the practical and emotional support provided to them by their networks. 25 The support of friends and family has been associated with predicting posttransplant UE VCA outcomes. 8 While social support is currently used to evaluate a candidate’s suitability for UE VCA, how social support is defined and assessed is at the discretion of each UE VCA program. 4 As VCA becomes more widely performed, standardizing eligibility criteria for social support will be necessary. 26 Future research should assess perceptions of social support received and needed among individuals with UE limb loss during the transplant process.
We found that patients’ perceptions varied regarding whether unilateral versus bilateral limb loss should affect patient selection for UE VCA. Participants’ contention that individuals with bilateral limb loss would have more to gain than individuals with unilateral limb loss is consistent with research among hand surgeons who reported being more supportive of performing UE VCA among people with bilateral limb loss. 2 Surgeons’ preference for bilateral UE VCA may be derived from perceptions of UE VCA as a high-risk procedure, as individuals with bilateral limb loss may have fewer treatment options available. 2
Our study participants’ preferences for patient selection criteria are similar to those used by transplant programs to evaluate patients. 8 Our findings highlight that patients prioritize similar characteristics as healthcare professionals; both populations have identified the same attributes as critical to determining a patient’s suitability for UE VCA.
Our findings have implications for clinical practice. Specifically, a patient-centered approach should be incorporated into patient selection processes to assess patient suitability for UE VCA. Patient-centered educational resources that are driven by patient perspectives in conjunction with data about UE VCA outcomes should be used to facilitate informed treatment decision-making regarding UE VCA.27,28 A patient’s perspective is vital to patient selection to ensure that the patient selection protocol for UE VCA incorporates characteristics meaningful to patients. Particular characteristics may influence patients’ willingness to adhere with the treatment regimen, which could ultimately affect patient outcomes.
Strengths of this study include a large sample of a difficult-to-reach population from a geographically diverse sample, which enhances the transferability of study results. Our qualitative approach yielded rich data to fill an important gap in understanding patient perceptions of UE VCA patient selection criteria. Additionally, our sample is representative of the broader population of people with UE amputations in terms of gender, race, and age. 29 This study has limitations. The use of a convenience sample, comprised predominantly of male and White patients, may limit the transferability of the results to other demographic groups of individuals with UE limb loss. We did not assess participants’ understanding of UE VCA and immunosuppression; participants may not fully understand the risks associated with VCA and lifelong immunosuppression use, which may have affected their reported preferences regarding the eligibility of individuals with unilateral or bilateral limb loss for UE VCA. Similarly, research shows that living donors are willing to assume much more risk than transplant healthcare professionals. 30 In both VCA and living donor contexts, such individuals may be more inclined to accept greater risks because they feel well enough to assume some risks to pursue their desired treatment.
Conclusion
Our qualitative study found that individuals with UE limb loss identified medical, psychological, and social characteristics as important for patient selection. Patient perceptions of UE VCA patient selection criteria may inform clinical practice of evaluating candidates.
Footnotes
Author contributions
EJG conceived and designed the research study, participated in performing the research, analyzing/interpreting the data, and writing the article. KV, MD, and JG-S participated in performing the research, analyzing/interpreting the data, and writing the article. BK, MD, MN, ML, WA, TR, and SF participated in the data collection. GB, ST, GD, and CC provided access to their patient populations for study recruitment. All authors reviewed and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Department of Defense Reconstructive Transplant Research Program awards: #W81XWH-19-2-0033/RT180041 to E.J. Gordon, Initiating Principal Investigator; #W81XWH-19-2-0034/RT180041P1 to M Levan, Partnering Principal Investigator; #W81XWH-19-2-0035/RT180041P2 to G Brandacher, Partnering Principal Investigator; and #W81XWH-19-2-0036/RT180041P3 to S Tintle, Partnering Principal Investigator. The opinions and assertions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of Defense, the US Government, the Uniformed Services University, or the Henry M. Jackson Foundation for the Advancement of Military Medicine. The funders had no role in study design; collection, analysis, and interpretation of data; writing the article; and the decision to submit the article for publication.
This study was supported by the Department of Defense through the CDMRP Reconstructive Transplant Research Program; Initiating Principal Investigator: E.J. Gordon (Grant No. W81XWH-19-2-0033); Partnering Principal Investigators: M. Levan (Grant No. W81XWH-19-2-0034); G. Brandacher (Grant No. W81XWH-19-2-0035), S. Tintle (Grant # W81XWH-19-2-0036).
Data availability
The data sets generated during and/or analyzed during the current study are not publicly available due to their sensitive nature, in that individual privacy could be compromised given the small samples by study site.