
Abstract
Objective:
Persistent vegetative state often occurs as a result of traumatic brain injuries; these patients are usually hospitalized for sustained periods, and the family caregivers are the main care providers in Iranian hospitals, especially for chronic and persistent vegetative state patients. The current study was conducted to investigate the family caregivers’ experiences of caring for persistent vegetative state patients following traumatic brain injury.
Methods:
This descriptive phenomenological study was carried out in 2019. Semi-structured interviews were done with 12 family caregivers caring for the patients in persistent vegetative state, hospitalized in a trauma center, after taking informed written consent and assuring about anonymity and confidentiality of their personal information. The interviews were analyzed using the Colaizzis҆ method.
Results:
After analysis of 12 interviews, 5 themes, and 10 subthemes were extracted from 428 codes. Five themes include “uncountable struggles/challenges,” “looking for peace,” “therapeutic concerns,” “preserving the connection,” and “unheard sounds.”
Conclusion:
In this study, the family caregivers of the persistent vegetative state patients in the hospital experienced some challenges, and looked for peace by doing some work, for example, praying. They had some therapeutic concerns and unheard sounds and tried to fulfill them. We recommend, by using the results of this study and other related research, necessary care and facilities would be provided for the family caregivers of persistent vegetative state patients in hospitals.
What do we already know about this topic?
Traumatic brain injury (TBI) is the main cause of disability among people under 45 years of age.
• 2.77% of patients with TBI would be in persistent vegetative state.
• Family caregivers (FCGs) are considered as the main members of the therapeutic team.
• Vegetative state patients are hospitalized for a long term.
• Available facilities are diverse in various regions for FCGs.
How does your research contribute to the field?
• This article is the first study on FCG experiences in Iran and in developing countries.
• This article showed the crises that FCGs of vegetative state patients are facing.
• The results showed the emotional and expectation concerns of FCGs of a vegetative state patient.
• The results reveal the required facilities for FCGs of vegetative state patients.
What are your research’s implications for theory, practice, or policy?
• The results of our study open a new window of paying attention to FCGs, which must be taken into account in health centers.
• Our results will help the health policymakers fulfill the requirements of FCGs of patients in hospitals.
• This study would be a base for other studies on family care in Iran and in other developing nations.
Introduction
Traumatic brain injury (TBI) is the main cause of death and disability for people under 45 years of age. It is estimated that more than 1.5 million people are affected by TBI in the United States, with a global incidence of 295 cases per 100,000 people. 1 The figure is equal to 56.3/100,000 in Iran. 2 Some research has confirmed that TBI causes more disability and mortality in developing countries and the mortality level is higher for the patients with severe TBI (Glasgow coma scale (GCS) score of <8). 3 In Iran, most of the TBI-affected individuals are younger than 30 years of age and are usually victims of car accidents. 4
Approximately, 2.77% of the patients with TBI are in the “persistent vegetative state” (PVS). This number is higher in developing countries (6.3%). 5 With regard to the incidence of TBI in Iran, 56.3/100,000 cases, 2 and the overall population of Iran (about 84 million people based on the world meter website.ifor26-7-2020:https://www.worldometers.info), it is estimated that, currently, there are 2980 patients in PVS in Iran.
The term “vegetative” was first mentioned in Aristotle’s treatise On the Soul, and it was accepted as a diagnosis in 1972 by Jennett and Plum, as mentioned in Adams and Fins’ study. 6 A vegetative state is a devastating condition, in which the patients may be awake, but have no signs of awareness. It has recently been known as the “unresponsive wakefulness syndrome.” 7 In this state, the sleep–wake cycle and autonomic functions remain intact, but the awareness about self, others, and the environment is lost (6). The criteria for PVS diagnosis are usually subjective, although recently, some imaging studies have been promoted. 8 Criteria for PVS diagnosis include no evidence of awareness and relation with the environment, no response to the stimuli and doing the directed behavior, lack of understanding of the speech, the return of the sleep cycle, smiling and yawning, and sufficient autonomic function for survival (by the medical and nursing care) as well as bowel and bladder incontinence and variability in the cranial and spinal reflexes. 9
Considering the criteria of PVS, 9 these patients need strict and vigilant treatment and care. In a review study by Georgiopoulos et al. 10 PVS patients were treated with the medications, such as Levodopa, Amantadine, Zolpidem, and surgical interventions, for example, deep-brain stimulation, extradural cortical stimulation, and intrathecal baclofen. Another study showed that these patients required deliberate management and care in the domains of social, economic, and ethical dilemmas, as well as nursing and medical actions. They are fully dependent on the nurses and caregivers and need a vigilant assessment due to the possibility of occurrence of the critical threatening issues. 11 Furthermore, some clinical staff and physicians believe that there is no optimistic prognosis for PVS patients and they advise organ donation and euthanasia. 12 However, these decisions are context-based and are not allowed in Iran. 13
Given the latency in the recovery and partly poor prognosis of PVS after TBI, 14 the family caregivers (FCGs) of the PVS patients are considered as the main members of the therapeutic team. They are the first source of care, especially for patients with long-term and permanent needs. 15 Moreover, they experience a variety of distresses, prolonged grief, symptoms of depression, physical and financial burden, and social problems. 16 They should be familiar with some common procedures, for example, suctioning, position change, and infection precautions, and they feel longlines, isolation, and a variety of social and emotional problems.17,18 With increasing the functional and cognitive impairments of patients, FCGs deal with more difficulties and burdens. 19 This situation is much worse in Iran, due to the lack of resources in the field of healthcare provider shortage 20 hence, the FCGs of the PVS patients need support and help. 21
Previous studies have mostly focused on the FCGs challenges of patients in PVS at home, in which all family members and accommodation are available,17,22 and there is a lack of studies on this issue in the hospital environment. Given the lack of evidence on FCGs of the PVS patients following TBI in the hospitals of low- and middle-income countries and the lack of a sufficient number of palliative and nursing-home centers in these areas, the current study was conducted to investigate the FCGs experiences of caring for the PVS patients, following the TBI.
Methods
Design
This qualitative study was done as a descriptive phenomenological study from June to October 2019. These types of studies demonstrate the fact that the research focuses on the experiences of individuals and the realities they live through are necessary. 23 Descriptive phenomenology was used in this study because it has been originated from Husserl’s idea of philosophy and shows the life experiences of the participants while suspending the researcher’s viewpoints, 24 congruent with the philosophical points of view of the researcher.
Setting and sampling
The study was performed in the intensive care units (ICUs) and neurosurgery wards of the Taleghani Hospital in Kermanshah province, Iran, the main trauma center in the west of Iran. It is a public hospital with 200 active beds and a bed occupancy of 96%–100%. The participants were family members of the PVS patients, who were in the hospitals and cared for the patients at least for 1 month and were willing to participate in the study. The FCGs with less than 1 month’s experience, and having a problem with recording the voice were excluded. The participants were selected through purposeful sampling, which is common in qualitative research and is well suited for recruiting well-informed people about a phenomenon. 25
Data collection
For data collection, the researchers received permission from the Deputy of Research and Technology of Kermanshah University of Medical Sciences. Furthermore, the second and fourth researchers identified the patients through introduction and diagnosis by the first author, who is an expert in neurosurgery, the researcher (the second and the fourth author) attended the mentioned wards in the hospital and explained the aim and procedure of the study to the FCGs. The data collection tool was a researcher-made checklist including some demographic information (e.g., gender, age, type of family relation, time of caring, patient time of hospitalization, and time of interview) and some open questions. After signing a written informed consent from participants or a legally authorized representative (their father) for participant 2 (P2) and P5, who were under 18 years old, and assuring about anonymity and confidentiality of personal information, the first and second authors conducted a semi-structured interview by asking open questions, such as, “What are your experiences about caregiving?,” “What are your challenges considering the caregiving?,” and probing words, for example, “why,” “explain more,” and “give an example.” Each interview was recorded, and the first, third, and fourth researchers made notes and then commenced the analysis afterward. The interviews lasted for about 18–43 min. They were performed in the physician’s office in the ward, in agreement with the participants. Data collection continued until data saturation, meaning when no newer data and information can be achieved. 26 The data saturation was achieved through 11 interviews, moreover, 1 additional interview was also conducted for assurance.
Data analysis
The interviews were tape-recorded and the third, fourth, and fifth researchers analyzed them using the Colaizzis҆ seven-step method, as noted in the study by Morrow et al. 27 In the first step, the researcher listened to the audio files several times and read them after writing the verbatim text. In the second step, the meaningful statements were determined. In the third step, the researcher formulated the meanings, and a related code was dedicated to each significant statement. In this stage, the researcher tried to include the opinions and presuppositions about caring for the PVS patients in the bracket. In the fourth step, the themes emerged and were clustered based on the meanings/codes. Furthermore, the themes were incorporated into each other and an exhaustive description of them was considered in the fifth step. In the sixth step, we tried to describe the phenomenon of caregiving for PVS patients in the hospital, while offering the participants’ quotations. In the final step, the verification and trustworthiness of the structure and findings were implemented. MAXQUDA 10 software was used for data management.
Trustworthiness
The trustworthiness was established with regard to four components of Guba and Lincoln’s Evaluative Criteria involving credibility, dependability, transferability, and confirmability cited by Shenton. 28 For credibility, the researcher fully engaged with the participants and immersed in their context after a complete explanation regarding the purposes of the study and tried to create trust between himself and FCGs. At least two sessions were held between the researchers, the process of the study was discussed and peer debriefing was done continually. Member check was performed by requesting the participants to have an opinion about the analyzed data. We tried to take all the meaningful statements into account including negative statements and made a thick description of the findings. For transferability, all the data about the settings of the study were provided. Dependability was resolved through an explanation and a clear description of the methodological approach alongside reliance on the other established studies. For confirmability, the writing notes were used besides having a complete description of the external audit, and the themes and subthemes were raised in an explicit method.
Results
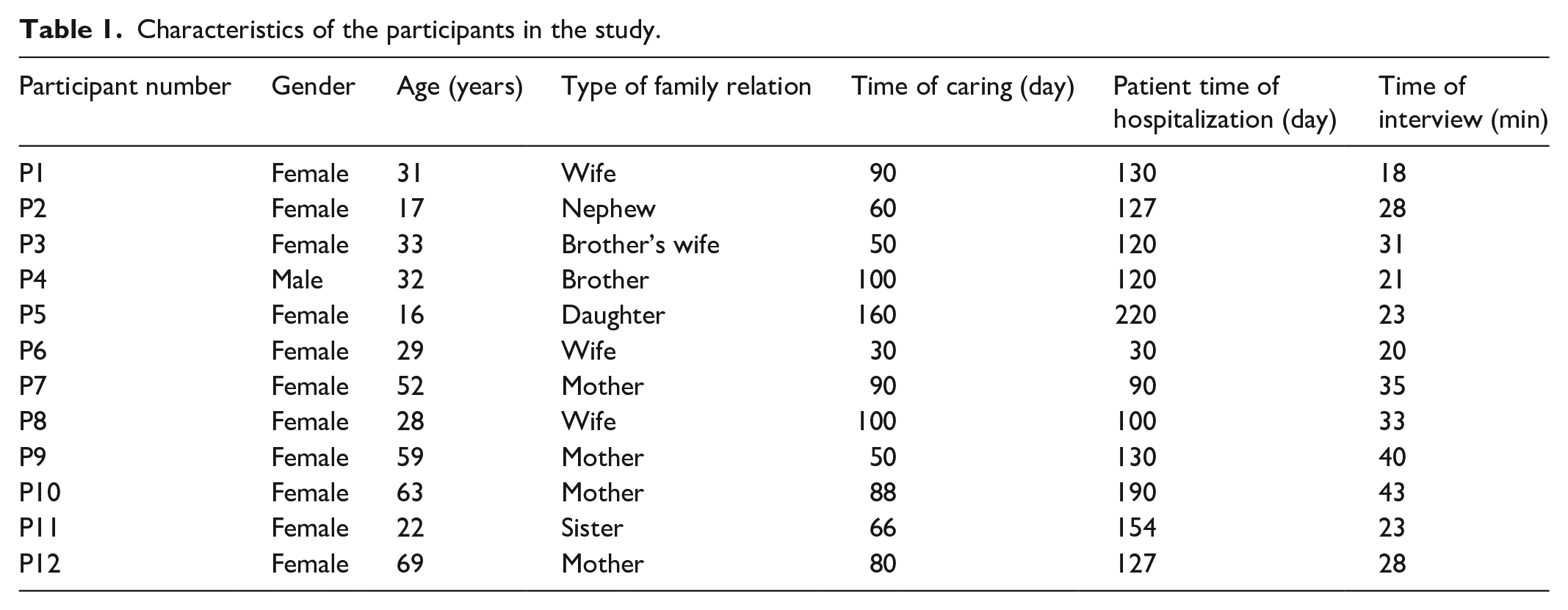
The 12 main caregivers of the PVS patients were included as participants in the study. Table 1 summarizes their demographic characteristics.
Characteristics of the participants in the study.
After a qualitative data analysis of 12 interview manuscripts, 428 codes were extracted and divided into five themes—“uncountable struggles/challenges,” “looking for peace,” “therapeutic concerns,” “preserving the connection,” and “unheard sounds.” After that, 10 subthemes emerged (Figure 1, Table 2).

Coding three of the studies.
Emerged themes and related subthemes.

Uncountable struggles/challenges
About 140 codes were related to this issue, and the FCGs expressed the tensions that had happened after the event. Two subcategories including “physical and psychological injuries” and “familial crises” emerged in this regard.
Physical and psychological injuries
Most of the FCGs said that they experienced psychological shock while facing the injured patients. This was accompanied by fainting, dizziness, continuous crying, and moaning. For example, one of the caregivers, the mother of a patient with head trauma caused by a car accident said “When I saw the head of my son that had been splinted, I was so upset and hurt and I fell down into my daughter’s arms” (69-year-old mother). Another participant said “I ҆have gone through a lot of ups and downs. I am very upset and shocked and feel like I am asleep and not awake. It is a terrible nightmare” (22-year-old sister). P8 (28-year-old wife) described that moment, when she saw the patient, as follows: “The whole world crashed on my head.”
Some FCGs faced physical damage because of an inappropriate situation in the ward and they were malnourished and got sleep disorders. P3 (33-year-old brother’s wife) described the terrible conditions associated with sleeping beside the patient: “I lay on the floor mosaics (which they barely allow) as the (Foley) catheters are next to my face and the smell of urine is very disturbing,” another caregiver explained her situation as follows: “I have been starving for a long time; we have no place to stay and I have a cold and our situation is very bad” (52-year-old mother).
Familial crisis
After the event, most of the FCGs were confronted with some familial crises, and 91 codes were extracted in this regard. Some participants, such as P2 (17-year-old nephew) and P12 (69-year-old mother), and on top of that, the male patient said that “The patients’ wives became separated from them after the accident,” so because of this, other family members engaged in caring. P12 (69-year-old mother) declared, At night, I and my other son are in the hospital, and during the day, my granddaughter and I stay here if she does not go to the school . . . Everyone is upset and my son has no personal life, he is at work for days and comes to the hospital at night and he is tired.
Many families also struggled economically. They mostly said that they cannot pay the hospital charges and afford adequate medications and devices. P11 (22-year-old sister), who cared for her brother was unemployed and said, My father has passed away a year ago (she implicitly stated that they have no other supporter), and we are all unemployed and we only receive my father’s social security wage and we are financially under pressure, it is difficult for us to travel (for coming to the hospital from home).
Another participant, the mother of a patient also explained, I do not have enough money to get the supplies, and I am under the auspices of the Relief Committee (a center for supporting very poor people in Iran), they (the committee officials) give me a small salary, they did not give me a loan, they told everyone that I have such a child and cannot lend me the money. (59-year-old mother)
Looking for peace
Some of the participants were exhausted because of the situation, and because they had to care for the patient for a long time, such as P9, P10, and P11, who were caring for the patients for more than 4 months in the hospital, and the patient’s prognosis was not optimistic. Therefore, the FCGs tried to escape these situations to calm themselves and somehow overcome the problems. For this purpose, they tried to “rely on praying” and “emotion evacuation” phrases, which were included in about 42 codes and statements.
Relying on praying
Many participants relied on religion as an assisting tool, often making statements such as: “resorting to the prayer,” “hope to God,” “giving Alms,” and “appealing to the Imams.” They tried to calm themselves and describe the event as “Divine providence.” One of the participants in interview 8, whose patient was in the ICU said: Until the morning prayer, I was awake and one of her sisters (the patient’s sister) who was single, was by my side and we were crying and crying and praying, until the morning, we only recalled Imam Reza and all our vows were in the way of Imam Reza.
Another caregiver declared: Our religious beliefs are very high and I always say that the doctors are the means, and only God can do it, on his own, and he can also heal my wife and I have prayed for him and made many vows hoping for his healing, to spend the rest of my life with him. (29-year-old wife)
Some participants took the arbitrary fasting (a kind of religious tradition in Islam), and one of them stated, “I was fasting and every hour of the night I woke up praying for God to save him (patient)” (33-year-old brother’s wife).
Emotion evacuation
Evacuation of the feelings—a method assisting the people in becoming peaceful and discharging their stress—was mentioned in 13 statements as a way of calming. It was indicated by “showing kindness,” “being happy with the patient,” and “crying.” P1 said, “Because I love my spouse, very much, I cannot and do not want to hear anything that disappoints me.” The other participant showed her affection for the patient and said: She understands all my words. The last time I took a bath, I was very upset and cried for her, and she shook her mouth, as though she was saying something, she approached my face and said something, kissed me, and her face was such that she wants to thank me. (33-year-old wife)
Three of the participants hoped that the situation will be ended. One of them, the nephew of the patient who was a high school student said “I wish he would get well soon or her daughters take her; I would love to get out of here soon because I am really tired, school time is near and I have not done any of my school work” (17-year-old nephew).
Therapeutic concerns
Almost all the participants played some sort of therapeutic role and tried to learn and perform them as appropriately as possible and 107 meaningful statements were extracted in this regard. For this purpose, four subthemes emerged including: “Relationship with the healthcare providers,” “information gap,” “continuing the assessment,” and “trying to provide a holistic care.”
Relationship with the healthcare providers
This subtheme was extracted from 22 codes and statements, and the participants had various types of communication with the healthcare providers, from friendship to fear and worries about the staff’s behavior. They mostly expressed satisfaction with the personnel because they allowed them to be at the bedside of patients and participate in the care. P8 (28-year-old wife) noted that “The staff was really good and allowed me to stay with my wife and read the Quran while they were in the ICU, and explained (about the patient issues) a lot to us,” another participant declared “The nurses are great, I have a good relationship with them; the crews are not bad either and they are good” (16-year-old daughter). However, some FCGs were not satisfied enough with the staff, because of not caring for the patients properly. For example, P1 (31-year-old wife) said: My husband needs to have a (Foley)catheter changed early because his catheter is blocked early, but the nurses change it later and say “we are tired so much” . . . When my husband’s condition becomes worse, they are wailing about what has happened to him . . . (for this), I feel sad, but I do not say anything (because she was afraid).
Information gap
Six participants did not know the causes of injury/trauma, some assumed that violence was the primary cause of damage; others said the patient had fallen from somewhere, and in line with this, they heard controversies and somehow contradicting views from the healthcare workers. P4 (32-year-old brother) said: They said God knows what is going on. The nurses said we would neither hope nor despair, but he could be paralyzed. One of the doctors said he (the patients҆ soul) was in another universe, I am not sure, called the vegetative world and said that his alertness was five and that he might stay in this situation for the rest of his life, all of us would be very upset.
The other caregiver represented “His doctor has said it will take time to heal or he may not heal at all” (17-year-old nephew). Some of them stated that they do not know how to care for the patients after discharge and have not been educated well.
Continuing the assessment
The FCGs tried to understand the meanings of consciousness and assess them at various times for identifying the changes. All of them knew about the meaning of the GCS score and hoped to raise it. P6 (29-year-old wife) said, No one has explained to us (about consciousness and GCS) and they just say that it is good to go up and the highest number is 15 and they say if it reaches 9 or 10, the patients҆ condition is good, it is really a big number for me because I do not have anyone and my husband is like a shadow on my head and my son’s (a proverb meaning that he is the overall supporter for us).
P7 (52-year-old mother) also noted, “When it (the consciousness) was 4, we were frustrated and upset, but as it went up, we were hopeful.”
Trying to provide a holistic care
In 52 statements, the participants declared that when it comes to providing the necessary care to the patients, they were ready to devote a substantial amount of time, even at the cost of their own health. Two of the participants who were a sister (P11) and a mother (P10), both said that they are ready to “sacrifice themselves for their patient.” P3 (33-year-old brother’s wife), in response to the question “How long do you want to continue the care?,” answered, “I will continue to the last point, as long as it takes.” The FCGs tried to address all of the patient’s needs from basic (such as changing the dress and cleaning the skin) to advanced (suction, dressing, and mouth care). In this regard, P12, who was a 69-year-old mother of a patient said “First I come (to the ward), wash her hands and face and rub olive oil all over her body, clean her teeth, feed her and give her pills, then do the suction and bath.” P11 (22-year-old sister) announced that she carries out the advanced operations on the patient “We do the suction, change her oxygen tube, clean her mouth, and give her food and medicine. We have done whatever the doctors said.” P1, P3, P4, and P7 declared that they perform physiotherapy and massage on the patients҆ foot and back every day, and P3 and P12 used olive oil to massage.
Preserving the connection
Considering this theme, 88 meaningful statements were identified and the participants tried to hold their connection to the patient and maintain hope however, they were affected by some events. In this aspect, two subthemes of “swing of the hope-disappointment” and “communication with the patient” were extracted.
Swing of hope-disappointment
Some participants began to feel hope by observing the perceived improvement signs. This mostly required time to pass to create more hope for the future. The caregiver in interview 6, who cared for her husband, said “When my son rehearsed the name of Imam Reza and my husband was shaking, both my son and I were hopeful, and that is a great and good memory for me, and I am getting more and more hopeful.” In this regard, the P10 (63-year-old mother) said that she gets her hope from God: I hoped and said he (the patient) was going to be good and although they (staff) did not give me hope, I was hoping for myself and now I have more hope and trust in the God and I think everything is going to be fine.
However, sometimes disappointment would occur because of the “statement that the staff gave about the disease of the patient,” “seeing similar patients,” and “having no movement or signs.” The P5 (16-year-old daughter) said: -First, we were hoping and thinking, my mother (the patient) would be fine but when we went to the ICU, we became disappointed. We saw another patient with a similar situation to my mother in the ICU and we met her companions and went to the ward before my mother, and when we asked about her later, she was dead.
P11(22-year-old sister) also complained and said: -I was expecting the doctors to give hope, but the doctor disappointed us so much. Once we went to another doctor’s office and he gave us hope and even wrote a prescription for medications that his previous doctor had not prescribed for him and we had to provide the drugs by our family in another country.
Communication with the patient
The FCGs are trying to communicate with the patients through different approaches. P1 said that the patient looked at her while she was speaking; another one used a hands-free device with voices familiar to the patient (17-year-old nephew). The mother of a patient in interview 12 said: -I asked one member of the staff who was there whether my son was listening to me? He said . . . he was listening and explained to me that he was like a child who hears and understands but cannot speak. I thought maybe he would understand. When I told her that I was her mother and if he could shake his hand or foot, he shook his hand and I had a special feeling at that moment, saying, thank God, he understands.
Some showed empathic feelings, for example, in interview 4, the participant (32-year-old brother) said: “I would like to be in bed (be a patient) instead of her in bed, but see my sister will be fine.” The caregiver in interview 7 mentioned the past events and stories to a patient and received a response “Sometimes when I tell her the past memories, she smiles and shakes hands and feet.”
Unheard sounds
The six FCGs had some expectations and complaints that they wanted to be heard and addressed. These types of expectations have often not been addressed despite mentioning most of their concerns and complaints. This was a recurring theme in a remarkable number of statements (41). P11 (22-year-old sister) complained that the hospital did not provide good accommodation for them, They do not give food to the caregivers, while they are very tired and need to eat . . . There is no resting place here, and we need a refrigerator and even a trash bin can be near my brother’s bed. Patients like my patient should be in a separate room because the noise is so disturbing . . ., My mother (another caregiver) wanted to stay during the night several times but because she was with other patients’ caregivers, who were men, she was not comfortable to sleep in the room, and she could not even fit and unfortunately, her chair did not fold (it was broken).
P9 (59-year-old mother) complained about the crowded ward and said: His (the patient) lungs are infected and there are a lot of infected people here because the room has four patients and each patient has a few visitors in the room. It is not suitable for the patients. If the rooms were for a single person, they (the patients) would heal sooner . . . -The doctor does not have the time and I do not see him. Once I went to the office and waited for several hours to see him. The nurse said “Take his (patient) home,” and I told by what means? Here, they (nurses) check the blood pressure, they inject the ampoules around the belly so that, their blood does not clot, and do the suction. How do I do these procedures at home?
Some participants, such as P5 and P6 expected to get a clear response from the staff about the patient’s situation, and the P3 requested “The bathroom and floor should be cleaned.”
Discussion
This study was conducted to investigate the Iranian FCGs’ experiences of caring for PVS patients following TBI, in a qualitative study. For this purpose, the FCGs in the main trauma center in Kermanshah province, western Iran were interviewed. Our findings showed that these caregivers had suffered from and tolerated the physical and psychological stresses, and were confronted with some familial crises, such as divorce, unemployment, and economic issues. In a cross-sectional study by Yousefzadeh-Chabok et al., 29 in Guilan province, Iran, the FCGs of the PVS patients had some psychological problems including depression, anxiety, phobia, somatoform, obsessive-compulsive, and paranoid disorder. Another study conducted in Italy verified many physical and psychological problems in these caregivers 30 and Chiambretto et al. 31 declared that the FCGs of PVS patients are affected continually by the prolonged grief. Gudarzi et al., in qualitative research, represented that the Iranian FCGs of the PVS patients suffered from some physical and psychological trauma, such as herniated disk, knee and arm pain, malnutrition, sexual disorder, severe fatigue, and insomnia. 17 These results are congruent with our study. The possible causes of the physical and psychological problems in these caregivers are related to the thoughts of caregivers about the possible death of the patient 32 and feelings of uncertainty. 33 In addition, contrary to some examples in the literature that the FCGs should be cared for and that their needs should be addressed, 34 the FCGs in Iran are neglected and have no support. 35 In this regard, another study in China showed that psychological interventions reduce anxiety and enhance the coping powers of the FCGs of PVS patients. 36 It is believed that these caregivers should be visited periodically by the clinicians, and undergo psychological and physical support in the hospitals.
The participants tried to soothe themselves by praying and changing their mindset to gain hope and boost positive thinking. These measures may help them in the process of coping with the issues. Goudarzi et al., 22 in a qualitative study on the FCGs of PVS patients, extracted the concept of “lasting hope” with subthemes of “positive thinking about the patient recovery” and “hopeful care,” meaning that the caregivers tried to hold their hope and continue the care and avoid the stimulators that threatened their thoughts and hope. Furthermore, they relied on spirituality for maintaining hope. Other studies have also revealed the role of beliefs, spirituality, and religion in the process of caregiver’s coping with cancer patients 37 and Alzheimer’s disease patients. 38 These results are in accordance with our findings. Spirituality is one of the main domains of human beings, and attending to it could enhance self-awareness and comprehension of the meaning of life connecting individuals to the transcendent powers of God, hence, they feel an “inner peace.” 39 The FCGs of the PVS patients seek meaning in care for the patients and try to feel that their work is in line with their spiritual and religious beliefs, therefore, God rewards them, and they can easily cope with the difficulties associated with caregiving. 40 Devotion to family and faith in God are considered the moderators of distress, 41 and this culture is also rooted in Iranian traditions.
The participants in this study had some therapeutic duties and tried to engage in caring measures, such as changing the position, physiotherapy, foot and back massage of the patient, and suction. Also, they struggled with the information gap about the care procedures, continually assessed the patient, and attempted to provide holistic care. In a qualitative research by Cipolletta et al., 42 the FCGs of the PVS patients knew themselves as the ones who comprehend and meet all the needs of their patients. They did not have complete trust in the healthcare workers and needed clear information. In the study by Latchem et al., 43 the families of the PVS patients supposed that physiotherapy could provide maximum comfort for the patients and helps them to maintain their health, and stimulates their consciousness. In addition, another study conducted in Iran showed that these caregivers are enthusiastic about education, and consider all the resources for this purpose. Because they are worried about what will happen after the discharge of the patients, doing imposed care duties, such as feeding, changing the position, changing the bed sheets, and giving the medication. 44 It seems that another factor influencing this situation is the shortage of nurses and workloads in the Iranian hospitals inducing the nurses to use the FCGs to assist the patients. 45 In this regard, some believed that the nurses should educate the FCGs about doing comprehensive care.17,21 Therefore, it seems to elaborate that some formal courses with authentic credits for FCGs of PVS patients are mandatory.
The six caregivers had some complaints and declared that their words are not heard, mostly related to the accommodation and to the fact that the physicians and nurses did not dedicate enough time to the patients. Others demanded hope from the healthcare staff. The governmental hospitals of Iran lack the appropriate accommodations, so the FCGs are under suffering. 35 They are frustrated by being in a hospital because they cannot participate in care in a good manner. 46 In a study by Ashrafian et al., 47 on the “unmet needs of the caregivers,” the most important needs were related to the information and to the fact that the physicians and nurse staff should come and see the patient when needed as quickly as possible. This was ascertained by another study mentioning that the FCGs lack support and care through trial and error. 48 Given the insufficient home care services in Iran, the teaching and supporting roles of the nurses and physicians for the FCGs of the PVS patients should be more prominent. 40 These caregivers stay in the hospitals for a long time, so it is suggested to provide them with the required services and that the staff nurses should reduce their suffering by offering compassionate, good relationships, and giving authentic information by devoting a period to answering their questions. Furthermore, the healthcare workers need to be trained in this regard and would be familiar with the requirements of FCGs. The training should include some continuing education on daily assessing and managing the problems of FCGs, and, if needed referring to other professionals to address their illness.
Limitations
This study had some advantages, as well as some disadvantages. For example, as an advantage, the researchers of the study were physicians and clinical staff members; therefore, they had a better understanding of the patients’ and caregivers’ conditions. However, most of the caregivers were female, and due to their tiredness, the interviews were somehow short, which may be considered a limitation. We used a research-made questionnaire with some open-ended and probing questions which was not pretested and a pilot study was not performed on it.
Conclusion
This qualitative study was done to investigate the FCGs’ experiences regarding caring for PVS patients with TBI. The FCGs experienced some stress, physical and psychological trauma, and some familial crises. Because these caregivers cared for a long period (at least for one month), they wished to liberate themselves by praying and evacuating their feelings. Furthermore, they did some therapeutic duties and tried to address all patients’ needs and assess patients’ signs, daily. However, they had an information gap and wanted to obtain the information through a relationship with the staff. The FCGs communicated with the patients and maintained their hope that the patient would recover. They complained about the accommodations and the lack of visits by the healthcare providers. Regarding the results of this study, it is recommended to address all the FCGs’ concerns by conducting formal courses for healthcare workers and FCGs and providing palliative care services for these caregivers in hospitals. Future research is necessary on the implementation of supportive measures and addressing the difficulties of FCGs of PVS patients.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231177550 – Supplemental material for The experiences of the caregivers caring for the patients in persistent vegetative state due to traumatic brain injury
Supplemental material, sj-docx-1-smo-10.1177_20503121231177550 for The experiences of the caregivers caring for the patients in persistent vegetative state due to traumatic brain injury by Ehsan Alimohammadi, Atefeh Arast, Zeljko Vlaisavljevic, Alireza Abdi and Haider Ramadhan in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121231177550 – Supplemental material for The experiences of the caregivers caring for the patients in persistent vegetative state due to traumatic brain injury
Supplemental material, sj-docx-2-smo-10.1177_20503121231177550 for The experiences of the caregivers caring for the patients in persistent vegetative state due to traumatic brain injury by Ehsan Alimohammadi, Atefeh Arast, Zeljko Vlaisavljevic, Alireza Abdi and Haider Ramadhan in SAGE Open Medicine
Footnotes
Acknowledgements
Author contributions
EA (neurosurgeon) AA (medical student), and AAR (nursing faculty, expert in qualitative research) contributed to designing the study. EA and AAR collected the data and analyzed by EA, AA, HR, and ZV (nursing professor). The final report and article were written by AA, ZV, HR (family physician), and EA, and the article was read and approved by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Kermanshah University of Medical Sciences. This study is the result of an approved project by the student research committee of the research and technology deputy of Kermanshah University of Medical Sciences (approval no. 3008929). The ethics research committee of the university confirmed ethical considerations (with no. IR.KUMS.REC.1399.524).
Ethics approval and consent to participate
The written informed consent was taken from the participants and legally authorized representative (their father) for P2 and P5, who were under 18 years old, and they would have assured about anonymity and confidentiality of personal information. The study was approved by the research ethics committee of Kermanshah University of Medical Sciences with ID: IR.KUMS.REC.1399.524
Consent for publication
All the authors and the Kermanshah University of Medical Sciences consented to publish the study in your journal.
Availability of data and material
Data will not be shared to ensure patient confidentiality.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.