
Abstract
Objective:
The objective of the study was to assess the efficacy of the use of cyanoacrylate glue (CAG) as a means of securing midline catheters and peripherally inserted central catheters with the modified micro-Seldinger technique in adult hospitalised patients.
Methods:
Randomised clinical trial with two groups (1:1): control and intervention. The control group received a securement method with a sutureless device plus transparent dressing and the intervention group received the same securement method plus the CAG. The study was approved by the Drug Research Ethics Committee of the Lleida Health Region.
Results:
A total of 216 patients were assessed. The two groups of the trial were homogenously distributed in terms of sociodemographic and clinical variables. The intervention group had a statistically significant lower incidence of peri-catheter bleeding and/or oozing during the 7-day study period (odds ratio (OR), 0.6; 95% confidence level (CI), 0.44–0.81; p < 0.001) and a statistically significant lower incidence of catheter dislodgements during the first 24 h (OR, 0.2; 95% CI, 0.04–0.91; p = 0.03). There were no statistically significant differences in the incidence of phlebitis (OR, 1.30; 95% CI, 0.60–2.83; p = 0.56) or catheter-related pain (OR, 0.88; 95% CI, 0.40–1.94; p = 0.84).
Conclusion:
Midline catheters and peripherally inserted central catheters secured with CAG had fewer complications than catheters not secured with this adhesive.
Introduction
Recently, in clinical practice there has been growing interest in products for the safe securement of vascular access devices (VADs) to try to decrease their associated complications. One such product is cyanoacrylate glue (CAG),1 –3 with octyl-butyl-cyanoacrylate (e.g. Secure-Port IV™) being one of the most commonly used types today. Thanks to its inherent properties, CAG can result in improvements3 –5 that include greater safety thanks to its resistance to traction, wound closure through a protective barrier, the minimisation of haematic and/or fluid discharge from the puncture zone, and the prevention of infection from various types of bacteria, yeasts and fungi.
Numerous studies have shown the safety of the use of CAG in different VADs, 6 and more specifically in peripherally inserted central catheters (PICCs),7,8 peripherally inserted central catheters-Ports,9,10 centrally inserted central venous catheters (CICCs), 11 midline catheters 12 and arterial catheters. 13 Their safe use has been verified in adults, 14 paediatric patients 15 and neonatal patients.16,17 CAG has also been shown to have a strong haemostatic effect in the presence of blood, 18 and its long-term use does not damage polyurethane catheters. 19 On the negative side, it has been suggested that its use might not be suitable for patients with sensitive skin or cutaneous diseases, and healthcare personnel training has been recommended as cases have been reported of tissue damage due to incorrect removal of the product. 4
No randomised clinical trial (RCT) has been found in the literature that has tested the effectiveness of securement with CAG in adult hospitalised patients in acute condition who require insertion of a VAD using the modified micro-Seldinger technique (MST) with an incision to dilate the insertion site. This is important because presently it is the most commonly used technique for the insertion of midline catheters and PICCs. However, it is not without complications and the catheters continue to have an unacceptably high failure rate. 20 It is of fundamental importance to study and test products that aim to reduce this failure rate. This is especially the case in situations in which there is constant handling of VADs by healthcare professionals for blood extractions and/or IV drugs.
The main aim of the present study was to assess the efficacy of the use of CAG as a post-insertion securement method of midline catheters and PICCs using the MST in hospitalised adult patients in order to determine whether protocol-led application of CAG reduces the main complications associated with this technique: peri-catheter bleeding or oozing, catheter dislodgment, phlebitis and catheter-related pain.
Methods
Trial design
An RCT was developed and carried out in the University Hospital Arnau de Vilanova (HUAV) in Lleida (Catalonia, Spain) by the Vascular Access Team (VAT) from 16 September 2020 to 30 September 2021, following CONSORT Guidelines. 21
The hypothesis employed in the study was that the application of CAG plus standard care after insertion of a VAD using the MST decreases the main complications related to these catheters.
Participants
In the study, the inclusion criteria were as follows: legal adults; patients that required insertion of a midline catheter (BD-PowerMidline™) or a PICC (BD-PowerPICC™) according to the decision-making algorithm of the VAT of the HUAV; patients who had voluntarily accepted and signed the informed consent form; and patients who had been admitted to a hospital unit (expected minimum 7-day hospital stay). The exclusion criteria were: patients with cutaneous conditions for which the application of a skin adhesive is contraindicated; and patients with a known allergy to CAG.
Interventions
The control group (CG) was treated with standard care6,22: transparent dressing (3M®-1655-Tegaderm™ IV), a sutureless stabilisation device (BD-19940-StatLock™ PICCPlus) and sterile gauze at the insertion site. The treatment group (TG) received the same standard care, without the sterile gauze, plus the application of CAG (SP-015V50-SecurePortIV™ AdhezionBiomedical, Topical Skin Adhesive, Volume 0.15).
Catheter insertion was performed on the basis of a pre-insertion, during insertion and post-insertion checklist in order to avoid any variability of criteria among the investigators. A haemostatic protocol of timed 2-min compression was applied after insertion of the catheter. If bleeding continued after 2 min, compression was maintained until its cessation.
Outcomes
The primary outcome measure was the number of participants with post-intervention peri-catheter bleeding and/or oozing assessed by observation (Yes/No). For this, the percentage of participants with peri-catheter bleeding and/or oozing after insertion of a midline catheter or PICC with the MST technique was calculated. Four inspections were carried out (post insertion, at 24 h, 72 h and 7 days) in which the puncture site was visualised for signs of bleeding and/or oozing.
The secondary outcome measure was the number of participants with post-intervention catheter displacement assessed by observation (Yes/No). For this, the percentage of patients with catheter displacement after insertion of a midline catheter or PICC with the MST was calculated. Four inspections were carried out (post insertion, at 24 h, at 72 h and at 7 days) in which the puncture site was visualised to check if the catheter was still in the same point or if it had been displaced.
In addition, the number of participants with post-intervention phlebitis was assessed on the basis of the Maddox visual phlebitis rating scale. 23 The percentage of patients with signs of phlebitis after insertion of a midline catheter or PICC with the MST was then calculated. Four inspections were carried out (post insertion, at 24 h, at 72 h and at 7 days) in which the puncture site was visualised to check for signs of phlebitis.
Finally, an assessment was made of the number of participants with post-intervention pain on the basis of the Visual Analogue Scale (VAS). 24 The percentage of patients with pain after insertion of a midline catheter or a PICC with the MST was then calculated. Four inspections were carried out (post insertion, at 24 h, at 72 h and at 7 days) in which the patient was asked to describe on a scale from 1 to 10 the pain they were feeling in the extremity related to the catheter.
Sample size
The sample size was calculated based on the proportion of peri-catheter bleeding and/or oozing after insertion of a VAD with the MST.
To calculate the sample size an alpha risk of <0.05 and a beta risk of <0.2 were chosen. The expected proportion for the CG was 0.75 (75% catheters not bleeding/oozing) according to current scientific evidence, 25 and 0.91 for the TG (91% catheters not bleeding/oozing), a clinically significant difference. A follow-up loss rate of 23% was estimated according to internal data of the team.
Randomisation, sequence generation, allocation concealment mechanism, implementation and blinding
The project investigators carried out subject recruitment, participant enrolment and randomisation to a CG or TG in a parallel group design with the help of the website http://randomization.com/. The resulting randomised list was printed and kept in a closed non-transparent folder. When a patient met the criteria to form part of the study and had agreed to participate, the list was consulted to determine which group that patient had been assigned to. The patient did not know which group he would be part of (single-blind); however it was impossible for the nursing and medical staff and the investigator/s to be blinded, as they were the ones performing the insertion and carrying out the standard care.
Data collection
The recorded variables were divided into categories. The main sociodemographic and health variables were collected: age, gender, date of admittance, diagnosis, pharmacological treatment, blood test results in last 7 days, hospital unit of admittance and date of catheter insertion and withdrawal. The variables of the VAD were also collected: reason for insertion, number of punctures, type of catheter, gauge, length, side and vein. With respect to VAD complications, four data collections were performed (on the day of insertion, 24 h, 72 h and 7 days post insertion), and if any additional treatment had to be carried out by the healthcare professionals, this was entered onto a data collection sheet.
The variables were first recorded manually in a data collection notebook and subsequently the study data were collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at https://redcap.icslleida.cat.26,27 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
Statistical methods
The statistical analysis of the data was carried out with the SPSS® software (IBM Corp. Released 2020; IBM Corp., Armonk, NY, USA). 28 A descriptive analysis was made of all the study variables. Categorical variables were described through absolute and relative frequencies and continuous variables using the mean or median, standard deviation (SD) and minimum and maximum (min–max), including the total number of valid values. Frequency tables and graphs were also generated. The Chi-square test or Fisher’s exact test was used for comparison of variables between subgroups of patients. Odds ratios (ORs) were calculated. A confidence interval (CI) of 95% was used.
Ethical considerations
The study was carried out following the ethical principles for medical research on human beings of the World Medical Association and the Helsinki Declaration, and respecting legal requirements for personal data protection and confidentiality as established by the General Data Protection Regulation.
An information sheet about the study was given to all participants before inscription and signed consent forms were obtained in all cases. Participation was voluntary.
Approval for the study was obtained from the Drug Research Ethics Committee (CEIC-2333, agreement 12/2020 dated 13 August 2020), and the study was registered in ClinicalTrials.gov (NCT05299060).
Results
Verification of the eligibility for participation in the study of 349 hospitalised patients resulted in the exclusion of 133. A total of 216 patients were therefore recruited who received a midline catheter or a PICC (Figure 1).

Flow diagram of participant recruitment, group allocation, follow-up and analysis (modified CONSORT 2010 flow diagram).
A total of 48 patients (22.2%) did not have the catheter in situ at 7 days, due to the following reasons: hospital discharge and/or end of treatment (58.3%), accidental catheter removal (18.7%), death (16.7%) and other (6.3%).
Sociodemographic and clinical characteristics
Mean age was 68.34 (SD ± 13.11), with 68.1% male (Table 1).
Socio-demographic data.

The VAD and hospital variables are shown in Table 2.
Data variables with respect to the VAD and hospital unit petitioning service.
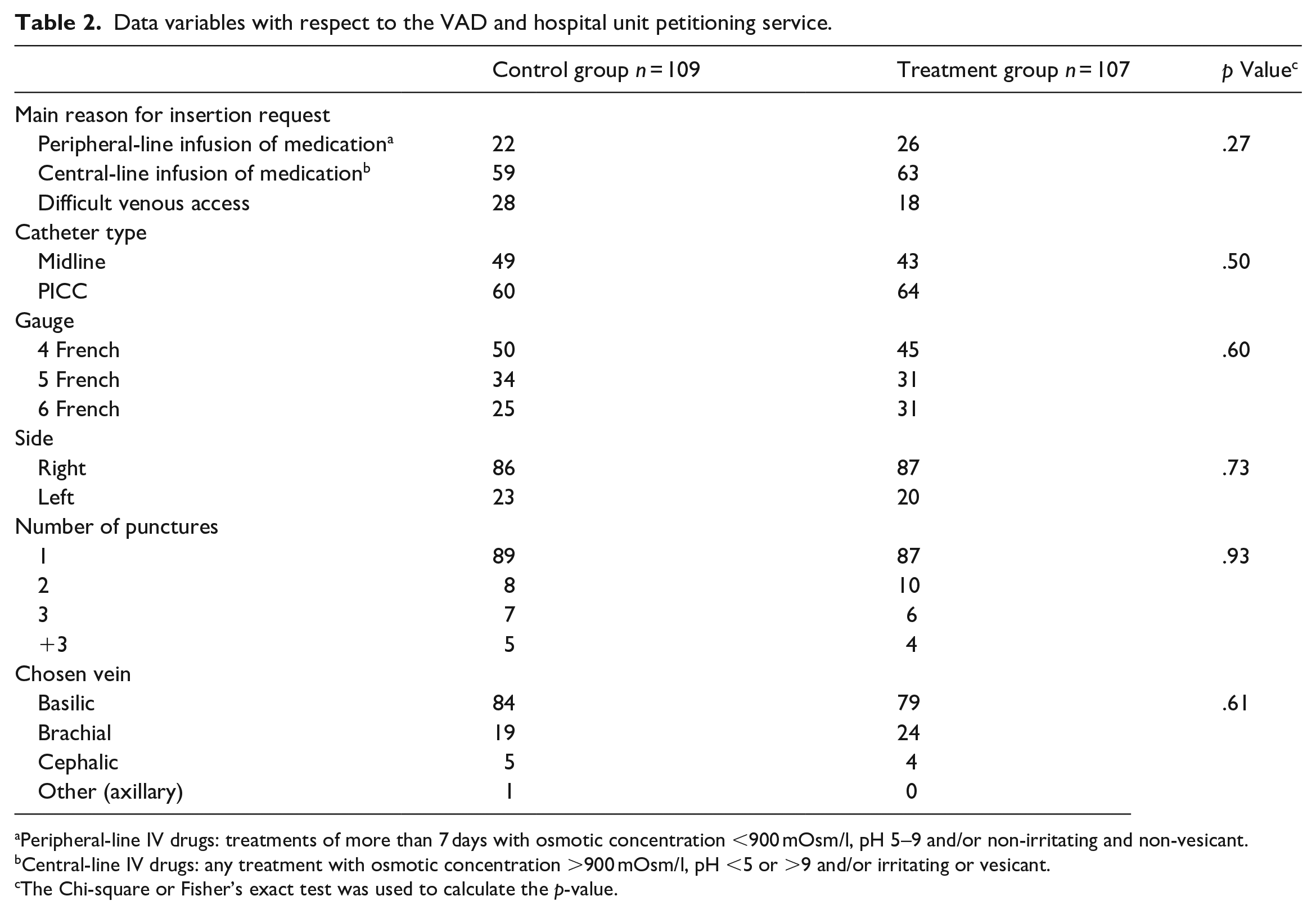
Peripheral-line IV drugs: treatments of more than 7 days with osmotic concentration <900 mOsm/l, pH 5–9 and/or non-irritating and non-vesicant.
Central-line IV drugs: any treatment with osmotic concentration >900 mOsm/l, pH <5 or >9 and/or irritating or vesicant.
The Chi-square or Fisher’s exact test was used to calculate the p-value.
The General and Digestive Surgery unit was the hospital service that made the most requests for the insertion of a VAD (48.1%), followed by Internal Medicine (19.5%).
The most commonly used anticoagulation and antiplatelet treatments in both groups were enoxaparin (36.1%), bemiparin (12%) and acetylsalicylic acid (10.4%), with no statistically significant differences between groups (p = 0.06).
Regarding coagulation and platelets, the mean international normalised ratio (INR) of the patients under study was 1.22 (SD ± 0.25, min–max: 0.81–2.5, p = 0.50) and the mean platelet count was 269,019 (SD ± 136,064, min–max: 48,000–1,261,000, p = 0.55), with no statistically significant differences between groups.
Inspection 24 h post insertion
With respect to the first inspection 24 h post insertion (Table 3), in the CG there was a higher incidence of peri-catheter bleeding and/or oozing (OR, 0.55; 95% CI, 0.32–0.96; p = 0.04) and a higher number of dislodgements (OR, 0.20; 95% CI, 0.04–0.91; p = 0.03) than in the TG, with statistically significant differences.
Inspection data 24 h post insertion.

The Chi-square test was used to calculate the p-value.
Fisher’s exact test was used to calculate the p-value.
No statistically significant differences were found for the appearance of signs of phlebitis (OR, 2.21; 95% CI, 0.64–7.58; p = 0.24) or catheter-related pain (OR, 1.62; 95% CI, 0.44–5.93; p = 0.52).
All patients with signs of phlebitis scored 1 or 2 according to the Maddox scale. Patients with pain recorded a mean score of 2.1 out of 10 according to the VAS scale (SD ± 1.3, min–max: 1–5).
Inspection data 72 h post insertion
In the inspection 72 h post insertion (Table 4), in the CG there was a higher incidence of peri-catheter bleeding and/or oozing (OR, 0.43; 95% CI, 0.23–0.79; p = 0.007) than in the TG, with this difference being statistically significant.
Inspection data 72 h post insertion.
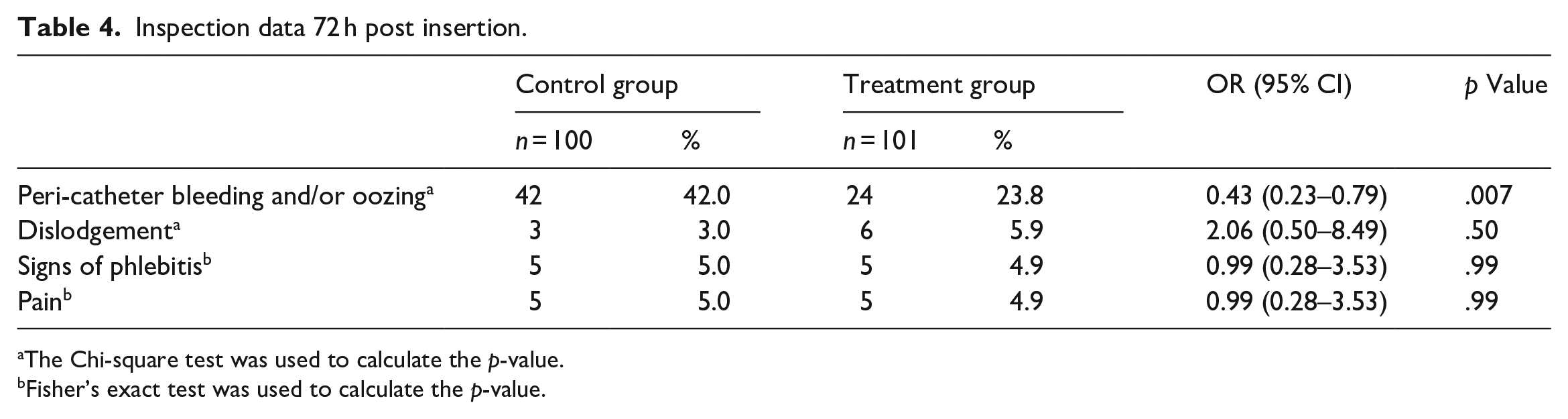
The Chi-square test was used to calculate the p-value.
Fisher’s exact test was used to calculate the p-value.
In contrast, there were no statistically significant differences with respect to dislodgements (OR, 2.06; 95% CI, 0.50–8.49; p = 0.50), or the appearance of signs of phlebitis (OR, 0.99; 95% CI, 0.28–3.53; p = 0.99) or pain (OR, 0.99; 95% CI, 0.28–3.53; p = 0.99).
Patients with pain scored a mean of 1.8 out of 10 (SD ± 1.03, min–max: 1–4).
Inspection 7 days post insertion
With respect to the inspection 7 days post insertion (Table 5), no statistically significant differences were found for peri-catheter bleeding and/or oozing (OR, 0.70; 95% CI, 0.35–1.40; p = 0.39), catheter dislodgement (OR, 1.67; 95% CI, 0.27–10.29; p = 0.68), signs of phlebitis (OR, 0.73; 95% CI, 0.12–4.46; p = 0.99) or pain (OR, 0.27; 95% CI, 0.03–2.43; p = 0.37).
Inspection data 7 days post insertion.

The Chi-square test was used to calculate the p-value.
Fisher’s exact test was used to calculate the p-value.
Patients with pain scored a mean of 1.6 out of 10 (SD ± 0.55, min–max: 1–2).
Additional care
With respect to additional care, performed by nurses of the hospital unit, a total of 34 urgent changes of dressing had to be made in 22 different patients, mostly for peri-catheter bleeding and/or oozing (33/34), with no statistically significant differences between groups (p = 0.44).
Grouped data of all inspections/care treatments
When grouping all the study data (day of insertion inspection, at 24 h, at 72 h, at 7 days and additional care), the total number of observations (inspections + additional care treatments) that was made amounted to 831 (425 in the CG and 406 in the TG). Peri-catheter bleeding and/or oozing was found in 33.9% of the total number of CG observations, compared to only 23.4% in the TG (OR, 0.60; 95% CI, 0.44–0.81; p < 0.001), with this difference being statistically significant.
Also in the grouped data, catheter dislodgement was found in 3.7% of the CG observations compared to 2.8% in the TG (OR, 0.74; 95% CI, 0.34–1.66; p = 0.55), with no statistically significant differences.
With respect to the appearance of catheter-related signs of phlebitis in the grouped data, no statistically significant differences were found between groups (OR, 1.30; 95% CI, 0.60–2.83; p = 0.56).
Finally, with respect to catheter-related pain, again no statistically significant differences were found between groups (OR, 0.88; 95% CI, 0.40–1.94; p = 0.84).
Discussion
It has been possible to show in this study that using CAG plus a sutureless stabilisation device and transparent dressing after insertion of a midline or a PICC with the technique MST in adult hospitalised patients has advantages that help to decrease some of the main complications related to VADs.
Effect on bleeding and oozing
CAG has been shown to have very interesting haemostatic properties for common use in clinical practice. With the application of CAG at the insertion site, the nursing staff will not have to perform as many dressing changes due to peri-catheter bleeding and/or oozing. Nonetheless, they should visually inspect the insertion site 24 h post insertion as use of the CAG is not a 100% guarantee against such bleeding and/or oozing, as shown by the 36.9% of patients in the TG who suffered this complication during the first 24 h. Reducing the number of changes of dressing is of great interest according to Timsit et al. 29 In the case of VADs, there is an associated reduced risk of catheter colonisation when removing the dressing (p < 0.001).
In the same study of Timsit et al., 29 earlier-than-scheduled changes of dressing were required in 67% of patients. In the present study, adherence was high in both groups, and earlier-than-scheduled changes were required only in 4.1% of the inspections.
The overall incidence of peri-catheter bleeding and/or oozing in the CG in the present study was 33.9%, slightly higher than in other similar studies such as that of Leung et al. 25 in which 24.7% of patients suffered this complication. This may be related to the incision performed prior to catheter insertion.
There was a lower tendency for bleeding in the TG compared to the CG (OR, 0.60; 95% CI, 0.44–0.81; p < 0.001), showing that the probability of bleeding in the group without CAG is 67% higher during the first 7 days than in the group with CAG.
This indicates that CAG is a promising application at reducing bleeding after VAD insertion, but haemostasis must be in place prior to application. These properties have been observed in vitro and in vivo in pigs 18 at 3, 6, 9 and 12 min after treatment. It has also been seen with different VADs: PICCs,7,14,30 CICCs 11 and arterial catheters.31,32 Application of CAG is therefore of particular interest in hospitalised patients where catheter handling by professional healthcare workers is constant. It is particularly of use in patients who are receiving an anticoagulation and/or antiplatelet treatment as it helps to reduce the risk of bleeding in a high percentage of patients.33,34 Although peripheral VADs and nontunneled PICCs are considered minimally invasive techniques, 35 this reduction in bleeding and/or exudate may help reduce the number of dressing changes by the healthcare professionals.
Effect on the number of catheter dislodgements
In the study by Lacostena-Pérez et al., 33 post-insertion VAD dislodgement was observed in 6.94% of cases, and in the prospective cohort study of Grau et al. 36 the corresponding value was 8.9%. In another study by Bugden et al., 7 it was found that the CAG group had 7% fewer dislodgements than the non-CAG group.
In the present study, the total number of dislodgements in the CG (3.7%) was very similar to that of the TG (2.8%). Statistically significant differences were only found in the inspection 24 h post insertion (OR, 0.2; 95% CI, 0.04–0.91; p = 0.03), indicating that the probability of catheter dislodgement in the group without CAG is five times higher during the first 24 h than in the group with CAG. This datum surprised the investigators as the number of dislodgments in the inspections 72 h and 7 days post insertion was very low in both groups.
Effect on phlebitis incidence
In the present study, the suspicion of phlebitis was very low (3% in the CG and 3.8% in the TG). In addition, there was no infection or serious adverse effects associated to the VAD during the first 7 days post insertion, which is in line with the current evidence.4,37
In a study by Lacostena-Pérez et al. 33 it was reported that 17.36% of patients had a suspected and 9.03% confirmed phlebitis. In another study by Leung et al. 25 it was reported that infection/phlebitis occurred in 9.7% of cases, but over a longer period of observation. In other RCTs, such as that of Rickard et al. 14 and Edwards et al. 32 no infection or catheter-related severe adverse effect was found in the group with CAG.
Consequently, as concluded in the study by Pittiruti et al., 2 it appears that CAG may reduce the risk of infection by reducing bacterial contamination via the extraluminal route in all VADs.
Effect on the number of catheter-related pain reports
The main indicator of phlebitis in inserted VADs is pain at the puncture site. In a clinical study by Chan et al. 38 the incidence of pain reported in the groups with and without CAG was 14% and 10.5%, respectively. In contrast, the incidence of catheter-related pain in the present study was very low. This may be related to the fact that the catheters were inserted by a group of nurses who are experts in this technique. In a recent study by Fujioka et al. 39 it was concluded that catheter insertion by specialist VAT nurses following a structured protocol significantly reduced pain scores compared to when performed by bedside nurses.
Limitations
Certain limitations of the study should be acknowledged. Firstly, as sterile gauze was applied to the puncture site in the standard care of the CG, this may have absorbed blood and/or exudate during the first 24 h which might have had a masking effect and resulted in missed bleeding and/or oozing events at the 24 h inspection. Secondly, no patients were entered in the study with an INR > 2.5 or with a platelet count <48,000/µl in the previous 7 days, due to a lack of patients meeting the inclusion criteria. Finally, some of the variables, such as pain, were subjectively evaluated through patient questionnaires.
Conclusions
In this study, a comparison was made of the efficacy of a sutureless stabilisation device and transparent dressing with and without CAG after catheter insertion with the MST in hospitalised adult patients. It was found that the occurrence of peri-catheter bleeding and/or oozing during the first 7 days post catheter insertion was 67% higher when CAG was not used compared to when it was.
It was also found that the probability of catheter displacement was five times higher during the first 24 h if CAG was not used compared to when it was.
On the other hand, it was not possible to confirm a reduction in the incidence of phlebitis or catheter-related pain during the first 7 days post catheter insertion.
All this suggests that CAG shows promise in reducing the number of bleedings and the number of displacements after insertion of midline catheters or PICCs, provided that effective haemostasis has been performed prior to its application.
Finally, further researches are recommended to compare the efficacy of CAG in different patients and health situations.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231170743 – Supplemental material for Effectiveness of cyanoacrylate glue in the fixation of midline catheters and peripherally inserted central catheters in hospitalised adult patients: Randomised clinical trial (CIANO-ETI)
Supplemental material, sj-docx-1-smo-10.1177_20503121231170743 for Effectiveness of cyanoacrylate glue in the fixation of midline catheters and peripherally inserted central catheters in hospitalised adult patients: Randomised clinical trial (CIANO-ETI) by Ferran Padilla-Nula, Alejandro Bergua-Lorente, Jordi Farrero-Mena, Anna Escolà-Nogués, Miriam Llauradó-Mateu, Carme Serret-Nuevo and Filip Bellon in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to express our appreciation for the selfless collaboration of all the nursing staff at HUAV who helped develop and carry out this study. We would also like to thank the heads of Innovation, Research and Training and the nursing management team of HUAV for their unconditional support. Our thanks also go to Dr Rubinat and Dr Blanco for their support and advice during the study design and management, as well as Dr Requena and Dr García for the critical analysis made of the study and the advice given before its submittance for publication. We would also like to thank Mr Malcolm Hayes for the English language revision
Author contributions
FP-N: Conceptualisation, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, preparation, creation and/or presentation of the published work, specifically visualisation/data presentation, writing – original draft, writing – review & editing. AB-L: Conceptualisation, data curation, investigation, methodology, software, validation, writing – original draft, writing – review & editing. JF-M: Conceptualisation, data curation, investigation, methodology, resources, writing – original draft, writing – review & editing. AE-N: Conceptualisation, data curation, investigation, methodology, preparation, creation and/or presentation of the published work, specifically visualisation/data presentation, writing – original draft, writing – review & editing. ML-M: Conceptualisation, data curation, investigation, methodology, writing – original draft, writing – review & editing. CS-N: Conceptualisation, data curation, investigation, methodology, writing – original draft, writing – review & editing. FB: Conceptualisation, formal analysis, investigation, methodology, project administration, validation, writing – original draft, writing – review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Lleida Official Nursing College [Grant 2020 to the best nursing research project].
Ethics approval
Ethical approval for this study was obtained from Drug Research Ethics Committee of the University Hospital Arnau de Vilanova (HUAV) in Lleida (Catalonia, Spain) of the Territorial Management of Lleida – GSS (CEIC-2333, agreement 12/2020 dated 13 August 2020).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
The study was registered in ClinicalTrials.gov (NCT05299060).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.