
Abstract
Objectives:
The aim of the study was to evaluate the stiffness of cervix and determine its significance in predicting successful outcome of induction of labour. The primary objective was to determine the differences in elastography indices of different areas of cervix between the outcome groups of successful and failed induction of labour. A secondary objective was to find out the correlation of these elastography indices with Bishop’s score and cervical length.
Methods:
This was a prospective, observational study conducted over a period of 6 months on pregnant women admitted in the labour room for induction of labour. Establishment of adequate regular uterine contractions – at least three contractions lasting 40–45 s in a 10-min period – was taken as end point for successful outcome of induction of labour. Even after 24 h of initiation of induction of labour, regular, adequate and painful uterine contractions were not established, then induction of labour was described as having failed. Prior to induction, cervical length measurement, Bishop’s scoring and elastographic evaluation of the cervix were done by stress–strain elastography. A colour map was produced from purple to red and a five-step scale – the elastography index – was used to describe the various parts of the cervix. The differences between elastography indices of different parts of cervix were estimated using Mann–Whitney U test. Correlation of the indices with cervical length and Bishop’s score was determined by Spearman’s correlation coefficient.
Results:
A total of 64 women were included in the study. A significant difference (p < 0.001) was found in the elastography index of internal os between the two outcome groups of success (1.76 ± 0.64) and failure (0.54 ± 0.18). However, the elastography index of central cervical canal, external os, anterior lip and posterior lips did not differ significantly across the outcome groups. A significant positive correlation was found between elastography index of internal os and cervical length (Spearman’s correlation coefficient, r = 0.441, p < 0.001) and between elastography index of external os and cervical length (r = 0.347, p = 0.005), whereas a negative correlation was seen between elastography index of external os and Bishop’s score (r = −0.270, p = 0.031).
Conclusion:
Elastography index of internal os can be used to predict outcome of induction of labour. Cervical elastography is a promising new technique for cervical consistency assessment. Further larger studies are required to determine some cut-off point for elastography index of internal os in prediction of outcome of induction of labour and to strongly establish the usefulness of cervical elastography for pregnancy management, preventing preterm delivery and establishment of cut-off points to determine successful induction.
Keywords
Introduction
Induction of labour (IOL) has become a part and parcel of modern obstetrics with nearly one-fourths of all births requiring it. 1 This refers to the use of medications or other methods to induce, or cause, labour.2–4 This practice is used to make contractions start so that delivery can occur.2–4 It is usually done when the risks of pregnancy continuation outweighs the risks of pregnancy termination and delivery. 1 However, not all inductions result in successful outcome. This highlights the importance of prediction of outcome of IOL. 1 Various methods have been used to assess the cervical status prior to IOL. 1 Bishop’s scoring of the cervix by digital palpation, introduced in 1964, remains the standard method worldwide to determine whether cervix is favourable or unfavourable for labour inducibility and to decide the method for IOL.1,5 Five variables, namely foetal head station in relation to the ischial spine, cervical dilation, cervical position, cervical length and cervical consistency, are used in this scoring system.5,6 The disadvantages of this scoring system include subjective nature of the assessment, irreproducibility and non-acceptance by the patient.1,5 Hence, new techniques need to be incorporated into clinical practice to overcome these limitations. Cervical length measurement by transvaginal sonography, first described by Zemlyn in 1981, is a good option with the advantage of being more objective.1,7 Sonoelastography, a rapidly developing modern imaging technique, first described by Shina et al, enables objective measurement of stiffness of tissue.7,8 At present, sonoelastography is used in identifying malignant and benign tumours in superficial organs like breast and thyroid as well as for skin, kidney, liver, lymph nodes, prostate, blood vessels, muscle system and cervix.8–11 Placental elasticity is also being studied to predict the time of delivery in threatened preterm labour and on intraoperative bleeding in post-caesarean pregnant women.12,13 The first report on cervical elastography during pregnancy was published in 2007. 7 Two types of cervical elastography have been developed for quantitative determination of stiffness of pregnant cervix-strain elastography and shear wave elastography. 9 Its principle is based on compression of the tissue by the ultrasound transducer during B-mode scan followed by computerised analysis of the speckle changes. 5
This study was aimed to evaluate the stiffness of cervix and determine its significance in predicting successful outcome after IOL. The primary objective of this study was to determine the differences in elastography indices (EIs) of internal os, central cervical canal (CCC), external os, anterior lip and posterior lip of cervix (determined prior to IOL) between the outcome groups of successful and failed IOL. A secondary objective was to find out the correlation of these EIs with Bishop’s score and cervical length.
Materials and methods
Study design: This was a single centred, prospective observational study conducted over a period of 6 months from August 2019 to January 2020.
Study participants: The study participants were antenatal pregnant women admitted in labour room, Department of Obstetrics and Gynaecology, AIIMS, Patna for IOL.
Sample size calculation: Taking into account the study conducted by M S Freund and K Preis in 2011 as the reference study, the means of EI of the internal os, where the difference between groups of failure and success of IOL was significant (0.39 and 1.23 units, respectively, and the pooled standard deviation was 1.19), were taken. With 80% power and 95% confidence interval, the sample size calculated by Statulator app was 64.
Sample size calculation results
Assuming a pooled standard deviation of 1.19 units, the study would require a sample size of 32 for each group (i.e. a total sample size of 64, assuming equal group sizes), to achieve a power of 80% and a level of significance of 5% (two sided), for detecting a true difference in means between the test and the reference group of 0.84 units.
In other words, if we select a random sample of 32 from each population, and determine that the difference in the two means is 0.84 units, and the pooled standard deviation is 1.19 units, we would have 80% power to declare that the two groups have significantly different means, that is, a two sided p value of less than 0.05. 14
Participants recruitment:
Inclusion criteria:
All antenatal pregnant women getting admitted in the labour room for IOL during the aforesaid period, willing to participate in the study and giving written and informed consent were enrolled in the study. Inclusion criteria included singleton pregnancy, above 34 weeks of gestation, vertex presentation, with proper indication for IOL and normal foetal well-being on cardiotocography.
Exclusion criteria:
The patients who were excluded from the study were those with contraindications of IOL such as previous two or more caesarean sections, placenta previa, contracted pelvis, pelvic tumour, cephalopelvic disproportion, malpresentation, previous cone biopsy, previous history of preterm delivery, active genital herpes infection, multiple pregnancies, foetal compromise and patient not willing to participate in the study.
Data collection:
Written and informed consent was taken from all patients. A detailed history including patient’s demographic data, parity, presenting complaints, history of present pregnancy, past medical and surgical history, obstetric history and family history was noted. Body mass index was not collected as patients were enrolled in the study in third trimester of pregnancy and at different periods of gestation. Clinical examination including general examination, systemic examination, obstetric examination and pelvic examination was done. Participants were assessed for IOL. Indication of IOL was noted. Cervical assessment was done using Bishop’s scoring. Prior to IOL, cervical elastographic evaluation was done by the Department of Radiodiagnosis using 4–9 MHz two-dimensional transvaginal transducer connected to Logiq E9 machine. The women were asked to empty the bladder and were placed in dorsal lithotomy position. Transvaginal probe was introduced into the vagina without applying any additional pressure to the cervix. Length of cervical canal was measured from the internal os to the external os from a sagittal view of the cervix. Then stress–strain elastography was applied. The transducer probe was not moved by the operator after visualisation of the cervix in B-mode. Patient was asked to breath normally. Elastographic images of the cervix due to the movement generated by patient’s breathing and arterial pulsation were achieved and were not operator dependent. Dual images of the uterine cervix on grey scale sonography and colour map elastography were taken from different regions of interest (ROI) – internal os, external os, CCC, anterior wall of cervix and posterior wall of cervix. For the elastography measurement, the ROI calliper was placed within a 1.0 cm radius on the internal os, external os, CCC, anterior corner of the cervix and the posterior corner of the cervix. The cervical elastography findings were described using a numeric scale called the EI. A colour map was produced from purple to red with purple designating the hardest tissue with a score of 0 points and progressively softer tissues displayed as blue (1 point), green (2 points), yellow (3 points) and softest tissue as red (4 points).15,16 A five-step scale – EI was created to describe the various parts of the cervix.15,16 If any part of the cervix had two colours, the highest possible was assigned to it. Images, in which foetal skull if visible was coded as purple and amniotic fluid was coded as red, were selected for analysis, using the best available image in each case. EI values from different parts of cervix were recorded. Figures 1 and 2 show the images of the cervical elastography measurement.

Dual images of the cervix with soft cervical canal and orifices.

Dual images of the cervix with hard cervical canal and orifices.
Patients then underwent standard obstetrical management in the labour room. Gestational age was determined from first day of last menstrual period and confirmed by crown rump length measurement in first trimester or head circumference in the second trimester. IOL was done according to the existing standard protocol in the institute. Bishop’s score was determined by a senior experienced obstetrician. The method of IOL was decided based on Bishop’s scoring and indication of IOL. Dinoprostone gel of 0.5 mg, intracervical 6 hourly (maximum of 3 doses), was given in most cases or 25 μg of oral misoprostol 4 hourly (maximum of 6 doses) was given (in cases with pre-labour rupture of membranes (PROM) or intrauterine death (IUD)) until adequate regular painful uterine contractions started. Establishment of adequate regular uterine contractions – at least three contractions lasting 40–45 s in a 10-min period – was taken as end point for successful outcome of IOL. Even after 24 h of initiation of IOL, regular, adequate and painful uterine contractions were not established, then IOL was described as having failed. Caesarean section was performed in cases of suspected foetal distress or failure to progress. Labour was managed by the labour room on-duty team, blinded to the findings of the pre-induction cervical elastography. Data on pregnancy outcomes were recorded.
There is no general consensus yet on definition of successful IOL. Most of the previous conducted studies considered vaginal delivery as successful IOL. However, this is questionable since caesarean section may be done in many patients with satisfactory progress of labour for indications such as foetal distress or worsening of maternal diseases. To exclude these confounding factors, establishment of adequate regular uterine contractions was taken as end point to reflect successful induction.
Statistical analysis: Data were entered into Microsoft Excel 2019 and then analysed in IBM-SPSSv25. Continuous data were represented in mean and standard deviation, and categorical data in frequency and percentage. Shapiro–Wilk test was done to test normality of variables. Mann–Whitney U test was used to compare the difference of non-normal continuous data between two groups, and Spearman’s correlation was used to find the association between the two continuous variables.
Ethical considerations: This study was conducted after approval from Institute Ethics Committee, All India Institute of Medical Sciences, Patna. (AIIMS/Pat/IEC/2017/200).
Results
A total of 64 antenatal patients were included in the study. The mean age of the patients was 24.55 ± 2.83 (in years). The mean period of gestation (in weeks) at IOL was 38.56 ± 1.29. The mean Bishop’s score was 3.03 ± 2.33 and the mean cervical length (in cm) was 2.61 ± 0.97. Of all the patients, 62.5% of the patients were nullipara, 32.8% of the patients were primiparous and only 4.6% of patients were multiparous. For IOL, dinoprostone gel was used in 79.7% of the patients, whereas oral misoprostol was used in 20.3% of patients. Successful IOL was seen in 46.9% of the patients and induction failed in 53.1% of patients. Table 1 shows the various indications for which IOL was done. The most common indications were intrahepatic cholestasis of pregnancy followed by post-dated pregnancy, PROM and decreased foetal movement. Other indications included gestational diabetes mellitus, oligohydramnios, IUD and pregnancy-induced hypertension.
Indications of induction of labour.
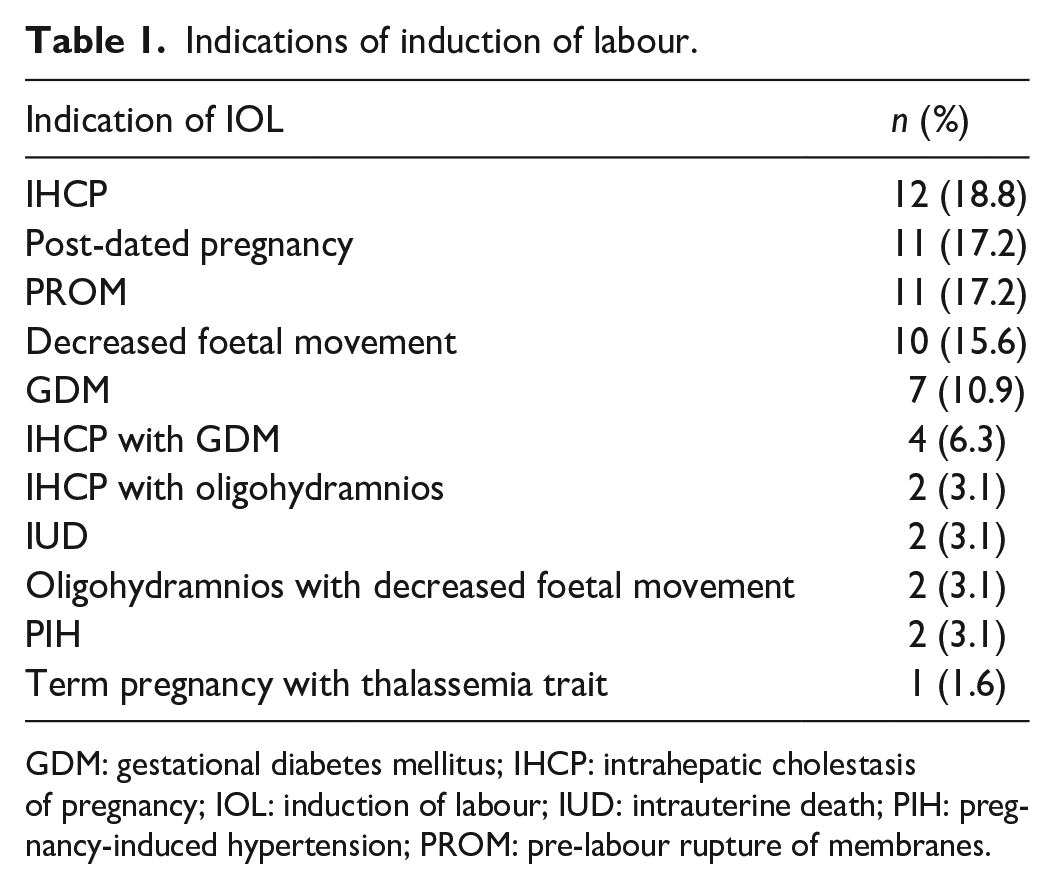
GDM: gestational diabetes mellitus; IHCP: intrahepatic cholestasis of pregnancy; IOL: induction of labour; IUD: intrauterine death; PIH: pregnancy-induced hypertension; PROM: pre-labour rupture of membranes.
Table 2 shows the mode of delivery and indications of caesarean sections. Of the total 64 patients undergoing IOL, 36 (56.3%) patients delivered vaginally, whereas caesarean section was required in 28 (43.7%) patients. The indications for lower segment caesarean section were meconium-stained liquor, non-reassuring non-stress test, arrest in second stage of labour and failed induction.
Mode of delivery and indications of LSCS.

LSCS: lower segment caesarean section; MSL: meconium-stained liquor; NRNST: non-reassuring NST.
Table 3 shows the difference of EIs of the internal os, CCC, external os, anterior lip and posterior lip across the groups of success and failure outcome of IOL. Mann–Whitney U test was used for the same, since the distribution of EI was not normal (Shapiro–Wilk, p < 0.05). 17 There was a significant difference in the EI of internal os between the two outcome groups of success (1.76 ± 0.64) and failure (0.54 ± 0.18), as shown by p < 0.001. However, the EI of CCC, external os, anterior lip and posterior lips did not differ significantly across the outcome groups.
Difference of EIs across the two outcome groups.

CCC: central cervical canal; EI: elastography index; IQR: interquartile range; SD: standard deviation.
Mann–Whitney U test used since the distribution of EI is non-normal.
Table 4 shows the correlations of different EIs with Bishop’s score and cervical length. The EI of internal os is significantly positively correlated with cervical length as shown by Spearman correlation coefficient, r = 0.441, p < 0.001, which is a strong correlation. Again, the EI of the external os has significant positive correlation with the cervical length (r = 0.347, p = 0.005) and negative correlation with Bishop’s score (r = −0.270, p = 0.031). Both are moderately correlated with the EI of the external os.
Correlations of EIs with Bishop’s score and cervical length.

CCC: central cervical canal; EIs: elastography indices.
Discussion
An increase in EI or decrease in consistency of cervical tissue around external os may suggest approaching delivery and may help us to decide management of patients undergoing IOL. In the above study, the EI of internal os was 1.76 ± 0.64 in the group with successful IOL and 0.54 ± 0.18 in the group with failed IOL. A significant difference in the EI of internal os between the two outcome groups implies that this can be used as a predictor of successful outcome of IOL. We also found that that there was a significant strong positive correlation of EI of internal os with cervical length (r = 0.441, p < 0.001). Thus, it can be said that of all the different areas of cervix, elastographic evaluation of the internal os seems to be the most useful factor in predicting outcome of IOL and thus be used in clinical practice prior to IOL. Similar to the findings of our study, Preis et al. 15 found a strong correlation between elastography results and success of labour induction. Freund et al. 16 found that the mean EI of internal os in patients with successful IOL was 1.23 while in the failed induction group was 0.39 with a significant difference. However, the outcomes of IOL used in these studies are different which makes the results hard to compare. Other studies favouring cervical elastography as a tool to predict outcome of labour include those conducted by Zhou et al., 1 Strobel et al., 18 Londero 19 and Fruscalzo et al. 20 Sonnier et al. 21 and Pereira et al. 22 however did not find cervical elastography useful in predicting delivery.
Although cervical elastography seems to be a promising tool in predicting outcome of labour, further studies with larger sample size focussing on overcoming the limitations of cervical elastography are required to strongly establish the usefulness of cervical elastography for pregnancy management, preventing preterm delivery and establishment of cut-off points to determine successful induction.
Limitations
Strain elastography requires human movements on the ultrasound transducer to generate stress on the target tissue. In our study, patient’s respirations and arterial pulsations were used. These movements are neither objective nor standardised which is a limitation of this method. Intra- and inter-observer agreements were not evaluated. Foetal movements or shaking hands of the operator can also act as pressure source and affect assessment of uterine cervix. In the presence of several vibration sources, it may be difficult to determine which images represent cervical stiffness. 23 This may lead to inter-observer and intra-observer variations. Shear wave elastography, in which ultrasound pulses is used to generate shear waves across the tissue of target, was not used. Also, unlike other tissues like breast, there is no internal reference tissue in the cervix which adds to another limitation. A reference cap – made of material with well-defined stiffness, which can compensate for the lack of reference tissue – was not applied to the end of the transvaginal ultrasound transducer. Definition of ROI also differs depending on investigator. Selective subjective selection of ROI cannot represent the stiffness of whole cervix. Other limitations include small sample size and confounding factor such as inclusion of multiparous women in whom labour is generally more rapid.
Conclusion
Cervical elastography is superior to cervical length and Bishop’s scoring in predicting IOL. It can be supportive in assessing the stiffness of cervical tissue around the internal os and thus help in predicting outcome of IOL. Although cervical strain elastography has been used for evaluation of cervical stiffness and for prediction of outcome of IOL, there is still no standardised measures established yet, hence limiting its incorporation into clinical practice. Cervical elastography, an incompletely defined technique at present, needs further improvement and evaluation for clinical use in assessment of cervical consistency.
Footnotes
Acknowledgements
The authors are thankful to all the women for their active participation in this study.
Author contribution
MA and NN conceptualised the study. MA, SS, NN and KK were involved in data curation. PK, SK, SS, NN and IP were involved in investigations, management of patients and data collection. Statistical analysis was done by RR. SS prepared the initial draft of the article under the supervision of MA, which was reviewed and approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Institute Ethics Committee, All India Institute of Medical Sciences, Patna (AIIMS/Pat/IEC/2017/200).
Informed consent
Written informed consent was obtained from all subjects before the study.