
Abstract
Objectives:
The main purpose of the study was to study the association between circulating soluble lectin-like oxidized low-density lipoprotein receptor-1 levels and various markers, including inflammatory markers such as high-sensitivity C-reactive protein and fibrinogen, serum lipids, and renal function, in patients with poorly controlled type 2 diabetes.
Methods:
The subjects were 70 patients (men 45, women 25) who were hospitalized for treatment of poor glycemic control. Plasma soluble lectin-like oxidized low-density lipoprotein receptor-1 levels were assayed using a sandwich chemiluminescence enzyme immunoassay.
Results:
Circulating soluble lectin-like oxidized low-density lipoprotein receptor-1 was significantly positively correlated with lectin-like oxidized low-density lipoprotein-1 ligands containing apolipoprotein B, reflecting modified low-density lipoprotein, and with inflammatory markers such as high-sensitivity C-reactive protein and fibrinogen. In addition, there was a significant positive correlation between soluble lectin-like oxidized low-density lipoprotein receptor-1 and urinary albumin excretion.
Conclusions:
Soluble lectin-like oxidized low-density lipoprotein receptor-1 may serve as a marker reflecting the degrees of inflammation and albuminuria in patients with poorly controlled type 2 diabetes.
Keywords
Introduction
It is widely recognized that increased low-density lipoprotein cholesterol (LDL-C) promotes development of atherosclerotic plaques and therefore is associated with the risk of cardiovascular disease.1,2 Oxidation of LDL has an important role in formation of plaques under various conditions.3,4 Oxidized LDL, but not LDL in circulation or attached to the vascular endothelium, can be scavenged via scavenger receptors (SRs) such as CD36 and SR-A, which are expressed mainly in macrophages,5,6 resulting in formation of foam cells from macrophages and in enlargement of atheromas. 7
Lectin-like oxidized low-density lipoprotein-1 (LOX-1), a type α integral transmembrane glycoprotein of molecular weight 50 kDa in the class E SR family (SR-E1), was first cloned in bovine aortic endothelial cells and is another important scavenger receptor associated with progression of atherosclerosis. 8 LOX-1 has a C-type lectin-like domain, a single transmembrane domain, an extracellular domain including an α helical coiled-coil neck domain, and a cytoplasmic N-terminal domain.7,9,10 LOX-1 is mainly expressed in vascular endothelial cells, but has also been found in monocytes/macrophages, vascular smooth muscle cells, platelets, cardiomyocytes, adipocytes and fibroblasts.11–16
LOX-1 is expressed at low levels under physiological conditions, but stimulation with modified LDL, including oxidized LDL, pro-inflammatory cytokines and shear stress can cause a major increase in gene expression and the protein level of LOX-1.7,17 Among these stimuli, oxidative LDL is the most investigated LOX-1 ligand. Binding of oxidative LDL to LOX-1 in vascular endothelial cells promotes upregulation of NADPH oxidase, 17 resulting in increased oxidative stress and subsequent increases of inflammatory cytokines, chemokines, and adhesion molecules via NF kappa B (NFκB) or activator protein 1 (AP1). 7 These processes result in formation of atherosclerotic plaque and onset of cardiovascular events.
A soluble form of LOX-1 (sLOX-1) (~35 kDa) is formed by proteolytic cleavage in the neck region of LOX-1, 7 and sLOX-1 in the circulation is considered to reflect the level of LOX-1 expression in arterial walls. 18 A clinical study found that circulating sLOX-1 was elevated in acute coronary syndrome, suggesting that it is a sensitive biomarker for diagnosis and prognosis. 19 Circulating sLOX-1 has also been associated with atherosclerosis-related disorders such as coronary artery disease, cerebral infarction, smoking, and diabetes,19–22 which suggests that sLOX-1 may also serve as a biomarker for these disorders.
In diabetes, sLOX-1 has been found to be higher in patients with type 2 diabetes than in control subjects, 22 but there is little information on the association of circulating sLOX-1 levels with diabetes- or atherosclerosis-related markers, especially in patients with poorly controlled type 2 diabetes. Therefore, the main purpose of this study was to investigate the association between sLOX-1 levels and various markers, including inflammatory markers, serum lipids, and renal function, in patients with poorly controlled type 2 diabetes.
Patients and methods
Patients
All patients (n = 70; men 45, women 25) who were subjects in our previous study (registered as UMIN000025767) 23 were included in analyses in the current study. Measurement of sLOX-1 was included as a secondary evaluation item in the previous study, 24 in which patients with type 2 diabetes admitted to hospital for treatment of poor glycemic control were consecutively registered from February 2017 to August 2017.
Key inclusion criteria in the study were patients (male or female) (1) aged 20 years or over at enrollment, (2) diagnosed with type 2 diabetes (based on 2010 Japan Diabetes Society criteria), (3) hospitalized for glycemic control and/or education for type 2 diabetes, and (4) who gave consent in writing for participation in the study. Key exclusion criteria were (1) patients with type 1 diabetes, pancreatic diabetes or secondary diabetes (Cushing syndrome, acromegaly etc.); (2) pregnancy, possible pregnancy, or lactation; and (3) patients judged by a physician to be inappropriate for participation in the study.
Detailed characteristics and laboratory data for the patients are presented in Table 1.
Clinical features and laboratory data in patients with type 2 diabetes.
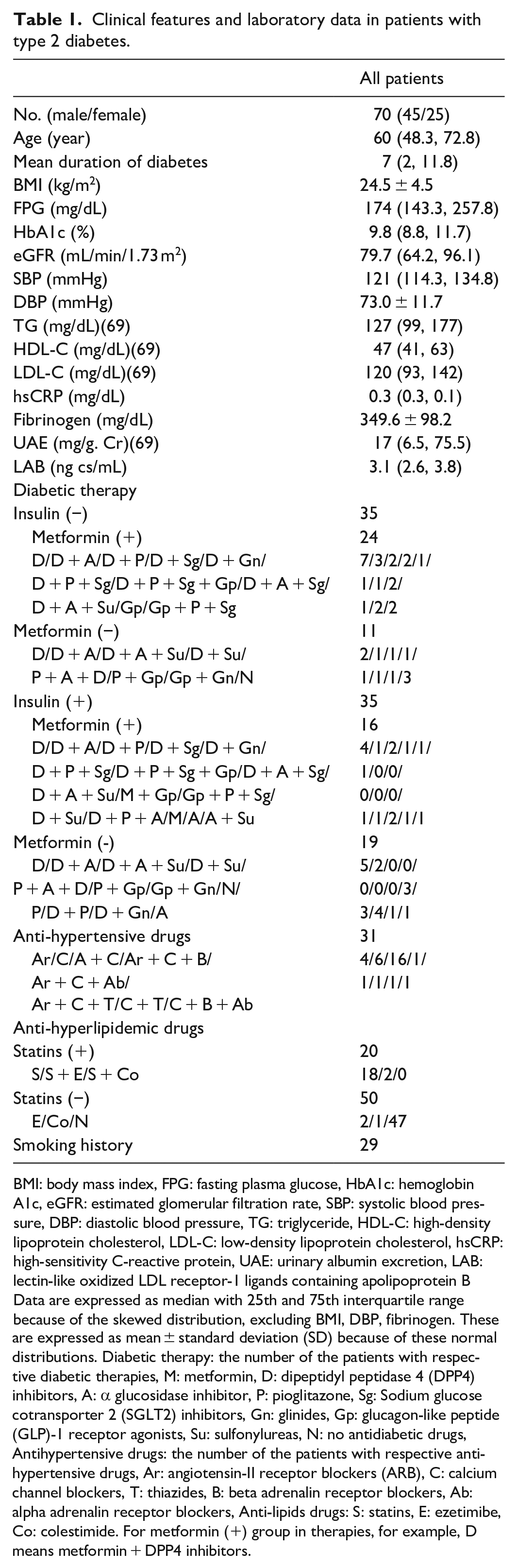
BMI: body mass index, FPG: fasting plasma glucose, HbA1c: hemoglobin A1c, eGFR: estimated glomerular filtration rate, SBP: systolic blood pressure, DBP: diastolic blood pressure, TG: triglyceride, HDL-C: high-density lipoprotein cholesterol, LDL-C: low-density lipoprotein cholesterol, hsCRP: high-sensitivity C-reactive protein, UAE: urinary albumin excretion, LAB: lectin-like oxidized LDL receptor-1 ligands containing apolipoprotein B
Data are expressed as median with 25th and 75th interquartile range because of the skewed distribution, excluding BMI, DBP, fibrinogen. These are expressed as mean ± standard deviation (SD) because of these normal distributions. Diabetic therapy: the number of the patients with respective diabetic therapies, M: metformin, D: dipeptidyl peptidase 4 (DPP4) inhibitors, A: α glucosidase inhibitor, P: pioglitazone, Sg: Sodium glucose cotransporter 2 (SGLT2) inhibitors, Gn: glinides, Gp: glucagon-like peptide (GLP)-1 receptor agonists, Su: sulfonylureas, N: no antidiabetic drugs, Antihypertensive drugs: the number of the patients with respective antihypertensive drugs, Ar: angiotensin-II receptor blockers (ARB), C: calcium channel blockers, T: thiazides, B: beta adrenalin receptor blockers, Ab: alpha adrenalin receptor blockers, Anti-lipids drugs: S: statins, E: ezetimibe, Co: colestimide. For metformin (+) group in therapies, for example, D means metformin + DPP4 inhibitors.
Methods
This study was cross-sectional one in which the correlation of circulating sLOX-1 with various markers was investigated.
Blood tests were conducted in the morning after overnight fasting for at least 10 h, on the day after hospital admission. Samples were frozen at −80 C until analysis for sLOX-1 and LOX-1 ligands containing apolipoprotein B (LAB). Body weight (BW) and blood pressure were also measured during admission. The methods for measurement of FPG, HbA1c, LDL-C, high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), sLOX-1, LAB, high-sensitivity C-reactive protein (hsCRP), fibrinogen, estimated glomerular filtration rate (eGFR), intima-media thickness of the carotid artery (IMT), cardio-ankle vascular index (CAVI), ankle brachial pressure index (ABI), and evaluation of diabetic retinopathy are described in our previous study. 24
Coefficient of variation of RR intervals (CVRR)
CVRR was evaluated in the morning in patients without arrhythmia on an electrocardiogram using records of consecutive cardiac cycles and calculated as CVRR = standard deviation of RR/mean RR × 100.
Urinary albumin excretion (UAE)
UAE was measured once in daily collection of urine during admission by an immunoturbidimetric method using a TAC-2 test albumin U reagent kit (Medical & Biological Laboratories Co., Ltd, Nagoya, Japan). Values of albumin were corrected for the level of urinary creatinine.
Urinary C-peptide (U-CPR)
U-CPR was measured once in a 24 h urine specimen during admission by a chemiluminescent enzyme assay, based on a two-step sandwich method using a Lumipulse-presto C-peptide reagent kit (Fujirebio Co., Ltd, Tokyo, Japan).
Ethical considerations
All subjects gave written informed consent for inclusion in the study (registered as UMIN000025767). The study was approved by the Local Ethics Committee at our hospital (approval number: 1654) and was conducted based on the guidelines of the Declaration of Helsinki.
Statistical methods
The normality of data for each variable was examined using a Shapiro-Wilk test. Among the variables shown in Table 2, body mass index (BMI), diastolic blood pressure (DBP), fibrinogen, and CAVI had a normal distribution. sLOX-1 had a skewed distribution even when the values were log10-transformed. Therefore, correlations between sLOX-1 and all variables in Table 2 were examined using Spearman correlation as a non-parametric coefficient. The correlation between hsCRP and fibrinogen was examined by Pearson correlation after hsCRP was log10-transformed because of the skewed distribution; the log10-transformed hsCRP had a normal distribution. The correlation between UAE and eGFR was evaluated using Spearman correlation because of the skewed distribution of UAE; UAE did not show a normal distribution even after log10-transformation. Comparisons of sLOX-1 between two subgroups of patients with type 2 diabetes were performed by Mann–Whitney U test. Comparison of sLOX-1 among three groups was performed by Kruskal–Wallis test with a post hoc Steel–Dwass test.
The correlation of sLOX-1 with multiple variables.

sLOX: soluble lectin-like oxidized low-density lipoprotein receptor-1; BMI: body mass index; FPG: fasting plasma glucose; HbA1c: hemoglobin A1c; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG: triglyceride; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; LAB: lectin-like oxidized LDL receptor-1 ligands containing apolipoprotein B; hsCRP: high-sensitivity C reactive protein; AST: aspartate transaminase; ALT: alanine transaminase; GGT: gamma-glutamyl transpeptidase; eGFR: estimated glomerular filtration rate; UAE: urinary albumin excretion; CAVI: cardio-ankle vascular index; IMT: intimal medial complex thickness; ABI: ankle brachial index; U-CPR: Urinary C-peptide immunoreactivity; CVRR: Coefficient of variation of R-R interval on electronic cardiogram.
These correlations were all evaluated using Spearman’s correlation coefficient (ρ) because of the skewed distribution of sLOX-1.
p: p value, p < 0.05 is defined as statistical significance (*). Parentheses mean the number of the patients.
On the needed sample size, the sample size calculation before initiation of the study (prior sample size calculation) could not be performed because of this study having been additional one. Although we selected non-parametric method on correlations between sLOX-1 and various variables due to above reason, the normal probability plot of sLOX-1 bordered on straight line by the log-transformation, despite the results of Shapiro–Wilk test. Therefore, it may be possible to assess the needed number of patients (n) by using a test for statistical significance of correlation coefficient (test for zero correlation), and we decided to perform this analysis. All statistical analyses were performed using BellCurve for Excel software (Social Survey Research Information Co., Ltd, Tokyo, Japan). A two-sided p < 0.05 was considered to show statistical significance.
Results
The median (25th and 75th percentile) sLOX-1 level was 464 (131.5, 776.25) ng/L. There was one extreme outlier in these data (19,753 ng/L). The correlations of sLOX-1 with all the examined variables are summarized in Table 2.
There was a significant positive correlation between log-transformed hsCRP and fibrinogen (r = 0.5557, p < 0.001) and a significant negative correlation between UAE and eGFR (ρ = −0.2953, p = 0.0318). No significant difference was obtained between subgroups of patients treated with and without insulin, metformin, ARBs or statins. There was no significant difference in sLOX-1 levels in patients with or without smoking history, or among those classified as no diabetic retinopathy (NDR), simple diabetic retinopathy (SDR), and proliferative diabetic retinopathy (PDR). 25
On the assessment for the needed number of patients, the most important associations in this study as we considered were those between sLOX-1 and hsCRP or fibrinogen. If log10 sLOX-1 followed normal distribution, Pearson’s correlation coefficients between log10 sLOX-1 and log10 hsCRP and between log10 sLOX-1 and fibrinogen would be, respectively, 0.2834 and 0.2725 (more than 0.25). Therefore, we estimated the needed number of patients when r is 0.25 using next formula: t = r (n−2)1/2 / (1−r2)1/2. In this case, 2 would be applied to t as 5% of significance (two sided), and n (the needed number of patients) would be estimated as 62.
Discussion
In the current study, there was a tendency for a positive correlation of sLOX-1 with LDL-C, and a significant positive correlation between sLOX-1 and LAB, which reflects modified LDL. 26 This latter result is consistent with a report showing an association of sLOX-1 with increasing LAB levels in middle-aged community dwelling US and Japanese men. 27 The result appears to be reasonable because stimulation by oxidative LDL (i.e. binding of oxidative LDL to LOX-1) promotes expression of LOX-1, 7 which probably results in an increase of sLOX-1 in the circulation. In addition, activation of LOX-1 by binding of oxidative LDL induces oxidative stress, which may then be involved in oxidation of native LDL; this may also partly explain the positive association between sLOX-1 and LAB.
The significant positive correlation between sLOX-1 and hsCRP, a representative inflammatory marker, is of interest. CRP, which can also bind to LOX-1, promotes vascular permeability and impairment of endothelium-dependent vasodilator function.28,29 Importantly, activation of LOX-1 by binding of CRP can increase expression of LOX-1 itself in endothelial cells. 30 Therefore, the significant association between sLOX-1 and hsCRP observed in this study is plausible, and a clinical study has shown a similar significant positive correlation in smokers. 31 However, in contrast, Tan et al. 22 found no significant correlation between sLOX-1 and log-transformed CRP in patients with type 2 diabetes. The reason for the discrepancy between our results and those in Tan et al. is unclear, but differences in backgrounds, including race, age (older patients in this study), and glycemic control (higher HbA1c in this study), might have influenced the results.
We also examined the correlation between sLOX-1 and fibrinogen. To our knowledge, this is the first report to examine this correlation. Fibrinogen is a coagulation factor and an inflammatory marker, 32 and we and others have shown a significant positive correlation between hsCRP and fibrinogen,33,34 as also observed in this study. The significant positive correlation found between sLOX-1 and fibrinogen is difficult to explain with certainty because it is unclear whether activation of LOX-1 can directly influence expression of fibrinogen. In addition, it is possible that hsCRP acted as a confounding factor for the association between sLOX-1 and fibrinogen because we were unable to perform multiple regression analysis with sLOX-1 as the dependent variable because of its skewed distribution. However, an increase in LOX-1 stimulates production of vascular growth35,36 and in plaque this increase can stimulate angiogenesis, which contributes to plaque instability and ulceration and results in an increased thromboembolic effect. This phenomenon may induce production of inflammatory factors, including fibrinogen. Regardless of the cause, this result (i.e. the correlation between sLOX-1 and fibrinogen) is interesting because the binding of oxidative LDL to LOX-1 in platelets induces activation of integrin αIIbβ3, which is a receptor for fibrinogen and therefore has a crucial role in formation of thrombus associated with fibrinogen. 37
A significant positive correlation between sLOX-1 and UAE was also found in the current study. This corresponds to the results in Stankova et al., 38 which were also obtained in patients with poorly controlled type 2 diabetes. These results also appear to support a study showing a significant relationship between LOX-1 expression in the tubulointerstitium and tubulointerstitial damage and protein in urine in patients with diabetic nephropathy. 39 However, it is important to note that a correlation between LOX-1 and tubulointerstitial damage does not necessarily imply involvement of LOX-1 because diabetic nephropathy and LOX-1 expression are both induced by a high concentration of glucose, 22 which causes vascular inflammation and oxidative stress products. However, mesangial cells are thought to be associated with lipid-mediated renal impairment, 40 and oxidative LDL treatment has been shown in vitro to induce expression of LOX-1 mRNA and protein dose-dependently in human mesangial cells. 41 This also supports the result in the current study. Interestingly, sLOX-1 was not correlated with eGFR, despite the significant correlation between sLOX-1 and UAE. Therefore, sLOX-1 might reflect an earlier stage of diabetic nephropathy than the advanced stage, at least at the clinical level.
Association of sLOX-1 with IMT (reflecting atherosclerosis) and CAVI (a marker of arterial stiffness) was also investigated. Increased oxidative LDL and expression of LOX-1 have important roles in progression of atherosclerotic plaques. 7 Therefore, we expected to observe significant correlations between these factors, but no correlation was obtained for sLOX-1 with IMT, supporting previous negative results, 27 or with CAVI. A significant positive association between sLOX-1 and ABI has been found in patients with type 2 diabetes, 42 but no correlation was obtained in the current study, which may have been due to the low number of enrolled patients. The negative results for the association of IMT or CAVI with sLOX-1 in the current study may be due to the presence of risk factors such as hypercholesterolemia, diabetes, or hypertension in our patients, which may have caused a tendency for an increase in sLOX-1. However, we could not confirm a potential elevation of sLOX-1 in our patients because we did not measure sLOX-1 levels in healthy control subjects. Notably, recent studies have shown significantly higher circulating sLOX-1 levels in patients with single-, double-, and multiple-vessel coronary artery disease (CAD) 43 or in those with CAD complicated by metabolic syndrome, 44 compared to healthy subjects. In addition, baseline sLOX-1 concentrations have been found to be correlated with major adverse cardiovascular events (MACE) in patients with stable CAD, 45 and there may be a further increase of sLOX-1 in situations of ulcerated plaques.46–48 Therefore, despite the negative results in this study, more detailed investigations are warranted on the association between sLOX-1 and cardiovascular disease.
sLOX-1 was also not correlated with FPG or HbA1c. These associations are uncertain in patients with type 2 diabetes,22,38 which may be due to the small number of patients in these studies and differences in the background of patients. Therefore, although glucose stimulates expression of sLOX-1 in vitro, 22 more detailed analyses in more patients are needed to determine whether glycemic control can influence circulating sLOX-1 levels from a clinical perspective.
There are limitations in this study. The prior sample size calculation could not be performed because the study was additional one as described previously, and therefore, the number of the enrolled patients was based on our previous study; the number of patients may have been relatively small. However, that appears to be in allowable range based on the result of test for statistical significance of correlation coefficient performed after the study. sLOX-1 was not measured in non-diabetic control subjects. The data in healthy subjects would be helpful in order to better interpret the value of circulating sLOX-1 in patients with type 2 diabetes although previous reports presented the significant elevation of circulating sLOX-1 in patients with type 2 diabetes compared with that in healthy subjects.22,38 This is an important limitation of this study. Because of the possible skewed distribution of sLOX-1 levels even after log-transformation, we did not perform multiple regression analysis with LOX-1 as a dependent variable. Therefore, in each correlation, involvement of possible confounding factors could not be completely excluded.
Conclusion
Circulating sLOX-1 was found to be significantly positively correlated with LAB, which reflects modified LDL, and with hsCRP and fibrinogen (inflammatory markers) and UAE. In contrast, sLOX-1 was not correlated with IMT (a marker of atherosclerosis) and CAVI (a marker of arterial stiffness), or with FPG and HbA1c (markers of glycemic control). Therefore, sLOX-1 may serve as a marker reflecting the degrees of inflammation and albuminuria in poorly controlled type 2 diabetic patients.
Footnotes
Acknowledgements
The author(s) thank the reviewers for constructive review and suggestions.
Author contributions
K.T. and T.S. investigated the patients. K.T. examined the data and wrote the manuscript. M.Y., K.H., T.T., T.I., and K.H. reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Local Ethics Committee at Dokkyo Medical University Saitama Medical Center (APPROVAL NUMBER 1654).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS) (grant numbers 19K09018 (Koshi Hashimoto) and 20K11394 (Kenji Hara)).
Informed consent
Written informed consent was obtained from all subjects before the study.