
Abstract
Objective:
Governance in health care generally means strengthening leadership and governance functions, improving systems, and having both central and local governments jointly take responsibility for overall health system performance. More than half of the world’s population has expressed distrust of state institutions including the health sector. Ethiopia, like other African countries, faces many challenges in the process of good governance building. The aim of this study was to assess the practices health care governance in the South Wollo Zone health sectors, Northeast Ethiopia.
Methods:
A facility-based cross-sectional study design was conducted in the South Wollo from 15 May to 15 June 2021. A simple random sampling technique was used, and the data were collected using a structured survey. The data were entered into Epi data version 4.6 for cleaning and exported to SPSS v.25 for further analysis. We performed binary and multivariable logistic regression analysis to identify factors of governance practices. Variables with p values less than 0.05 during multivariable logistic regression analysis were declared statistically significant.
Results:
A 96.75% (387) of the study participants completed the study questionnaires. Out of these, 37.98% (95% confidence interval: 33.1%, 42.9%) have been found practicing good governance in the health sector. Having had training (adjusted odds ratio = 7.92, 95% confidence interval: 4.04, 15.51), having job descriptions (adjusted odds ratio = 2.05, 95% confidence interval: 1.03, 4.09), opportunity to share with peers (adjusted odds ratio = 6.64, 95% confidence interval: 3.02, 14.62), political interference (adjusted odds ratio = 0.40, 95% confidence interval: 0.22, 0.71), and age < 25 years (adjusted odds ratio = 0.13, 95% confidence interval: 0.02, 0.77) were found to have a statistically significant association with the governance practice of managers.
Conclusion:
The overall practice of governance was found poor in light of the national and World Health Organization standards for health sector Governance. Having had training, having job descriptions and the opportunity to share with peers significantly increased the odds of good governance while political interference and young age significantly decreased the odds of good governance. Managers could implement training, write job descriptions, and encourage sharing with peers to improve governance.
Introduction
Good governance is a system of values, policies, and institutions for communities to manage economic, political, and social issues through government, private sectors, and civil sectors. 1
Good governance in health care generally means strengthening leadership and governance functions, improving systems, and having both central and local governments jointly take responsibility for overall health system performance. 2 In addition to our vision and mission to develop policies, programs, and strategies that support our overall health goals and objectives, good governance has these policies at all levels for accountability and transparency. 3 Citizen participation is one of the most important factors in the practice of good governance. 4
According to Jaya, good governance is the exercise of legitimate political power and the development and implementation of policies and programs that are fair, transparent, non-discriminatory, socially sensitive, participatory, and accountable to the people. 5
More than half of the world’s population has expressed distrust of state institutions. 6 The concept of good governance is relatively new. This appears in a World Bank report on sub-Saharan Africa, explaining that the crisis in the region is a government crisis. 7
The effects and consequences of bad governance affect the poorest, leaving them vulnerable as they are deprived of basic needs such as health care, food, and shelter. 8
Ethiopia, like other African countries, faces many challenges in the process of democratization and good governance building. To fill the identified gaps, the Government of Ethiopia has developed a cross-sectoral national capacity-building strategy advocating the principles of decentralization, regional autonomy, and efficiency, with community participation and accountability in the health sector. 9
Good governance is pointed out as one of the Millennium Development Goals (MDGs), Sustainable Development Goals, and Poverty Reduction and Sustainable Development Agenda goals. It is probably the only and most important factor in eradicating poverty and promoting development. 10
According to a state government survey conducted by the United Nations Economic Commission for Africa, Ethiopia’s performance on all indicators of good governance is below the sample average (53%), while Ethiopia’s sample indicator is 36%. The same trend persists in the country’s governance profile by subsequent Economic Commision for Africa’s (ECA) governance survey. In the public sector government and agency International Development Association (IDA) resource allocation index, Ethiopia has an average score of 3.1, with six being the highest and one being the lowest. In particular, the country’s public sector transparency, accountability, and corruption scores are below average at 2.5 points. 7 In Ethiopia, plan for accelerated and sustained development to end poverty (PASDEP) promotes a higher level of public participation and a more effective environment for improving public sector accountability, responsiveness, and effectiveness mechanisms. 7 Governance should be “good,” not “bad.” It is a term that symbolizes the paradigm shift in the role of government. 11
Health governance and community welfare are key elements of good governance which are considered in a value framework that includes health as a human right, universal public goods, and one of the key aspects of social welfare and equality. 12
Although the Ethiopian government has taken important steps to promote good governance by approving many international human rights documents, the Constitution generally adopts a multi-party government system and is the most internationally recognized since 1991. The process of good governance building is facing serious and complex challenges. The challenges are primarily related to the fact that good governance is still in its infancy. Participation in national decision-making processes, particularly the health care system, is hindered by a lack of authority, financial incentives, or influence. 13
However, health systems in several countries around the world are still poorly managed, and these countries still face many challenges in making health care decisions. 14
This study assessed the practice of health care governance among case team leaders and managers in public health institutions found in South Wollo, Amhara Regional State, Ethiopia which contributed a lot to the health care managers and decision-makers taking an intervention in the practice of governance.
Methods and materials
Study design and setting
The facility-based cross-sectional study design was carried out in South Wollo from 15 May to 15 June 2021. The South Wollo Zone is adjacent to North Shewa to the south, East Gojjam to the west, South Gondar to the northwest, North Wollo to the north, Afar region to the northeast, and the Oromo Special Zone to the east.
It is one of the 11 zones of the Amhara National Regional State. There are 21 districts in this zone with a total population of 2,518,862, of which 1,248,698 are male. It has a total area of 17,067.45 km2. The South Wollo Zone Ministry of Health reports that the zone has 11 public hospitals, 133 health centers, and 508 health posts.
The estimated potential coverage of health services was 47.7%. Dessie is 401 km north of Addis Ababa, the capital of Ethiopia, and 480 km from Bahir Dar, home of the Amhara National Regional. There are a total of 6454 health care providers in the zone. There are 735 case team and managerial level workers. 15
Source and study population
All health institution managers and case team leaders in South Wollo were considered as a source population while all selected health facility managers and case team leaders currently working were considered as a study population.
Illegibility criteria
All case team leaders and managers who were available during the data collection period were included in the study, while individuals who are unable to communicate due to serious illnesses and individuals who have less than 6 months of experience in the current health facility during the data collection period were excluded.
Sample size determination and procedures
The sample size was determined using a single population proportion formula with the following assumptions: The proportion of good governance practice (p) in Eastern Ethiopia was 54.6%, 16 margin of error (d) 5%, at 95% CI and adding 5% non-response rate.

The final sample size used for this study was 400 case team leaders and health institution managers in South Wollo Zone.
After listing all health institution managers and case team leaders (735) found in the south Wollo zone, 400 samples were selected by using the lottery method for all health institutions as a sample frame. From those by simple random sampling technique, managers and case team leaders were selected.
Study variables
Governance practice (good or poor) was used as a dependent variable, and socio-demographic, training-related, and work environment-related factors were used as independent variables.
Operational definitions
Governance practices were measured based on responses to 32 statements, each scored between 0 and 4. Taking the mean value as a cutoff point of 60, a score of below the mean (0–60) indicated poor governance practice and a score of 61–128 which is above the mean indicated good governance practice. 17
Having had training: Case team leaders and managers who had got governance-related training in the past during their career. Organizational communication: Whether the organization has an external relationship with other organizations. Managers: health center director, hospital chief executive officers, and Woreda health office heads. Case team leaders: health center department heads, hospital Metrons, medical directors, and department heads.
Data collection tools and procedures
Data were collected using standardized and structured questionnaires adapted from reviewing different literature in which all data relevant to the governance were gathered and analyzed. Both primary and secondary data were used as a source of information. A pre-tested structured questionnaire composed of closed-ended self-administered questionnaires was used in 5% of the calculated sample to collect the required information. The study used the governance statement standardized tools developed by the health system and adopted from the study conducted in eastern Ethiopia. 16 Eight BSc nurses were recruited for data collection, and two MSc. Nurses were recruited for the whole process of data collection supervision.
Statistical analysis
The questionnaires were first to be developed in English and then translated into the Amharic language by language experts via the Wollo University English department. A day of training was given to supervisors and data collectors on basic data collection techniques, procedures, and confidentiality and privacy issues. Even though standardized questionnaires were used, a pretest was conducted among 5% of the sample size of North Wollo zone health facilities to check the consistency of the questionnaires. In addition, the necessary adjustments were made before actual data collection. Moreover, the data collector was monitored daily by two supervisors. The filled questionnaires were inspected daily for integrity and consistency by supervisors and the principal investigator.
The collected data were entered into Epi-data version 4.6 and then exported to SPSS version 25 for statistical analysis. Data cleaning was performed to check for accuracy, consistency, and missed values of the variables. Any logical and consistent errors identified during data entry were corrected after the revision of the original completed questionnaires.
To explain the study population about relevant variables, descriptive statistics (frequencies, mean, SD, percentage) were used. Both binary and multivariable logistic regressions were fitted to assess the association between the outcome and explanatory variables. Hosmer and Lemeshow’s test (Surjanovic N. et al., 2020) was found to be insignificant and the Omnibus test (Ebner B. et al., 2021) was significant which indicated that the model was fitted. Variables having a p value <0.25 during bi-variable analysis were entered into the multivariable logistic regression model. Associations between dependent and independent variables were assessed, and their strength was presented using odds ratios at 95% CI. Variables having a p value <0.05 in the multivariable logistic regression model were considered statistically significant factors for governance practice. The result of the analysis was presented using tables, charts, graphs, and texts.
Ethical approval and consent to participate
Ethical clearance was obtained from the Ethical Review Committee/ERC/of Wollo University, College of Medicine and Health Sciences with reference ID: CMHS 474/02/13 on 05/06/2013. These letters were sent to the respective heads of the health facility. Participants were informed of the purpose and importance of the study. The data were collected after obtaining complete informed consent in writing, maintaining the confidentiality of the information, and ensuring privacy. All the ethical issues are managed according to the Helsinki Declaration.
Results
Socio-demographic characteristics
A total of 387 participants completed the questionnaires making a response rate of 96.75%. The mean (SD) age was (32.42 ± 6.31) years. The majority (228 (58.9%)) of the respondent’s age was found between 25 and 35 years. More than two-thirds (267 (69.0%)) of the study participants were married. More than half 222 (57.4%) were orthodox in religion. Among the respondents, 204 (52.7%) and 67 (17.3%) were nurses and midwifery professionals, respectively. Among respondents, 181 (46.8%) have 1–5 years of work experience and the majority 276 (71.3%) of the respondents were working in the health centers (Table 1).
Socio-demographic characteristics among case team leaders and managers of South Wollo Zone Health Facilities, Ethiopia, 2021 (n = 387).

Radiology, finance, and administration; **Specialist, subspecialist.
Training and work-related factors
The majority of study participants were educated from government and private colleges, 287 (74.2%) and 100 (25.8%), respectively. Concerning the duration of training, more than half 143 (55%) was for >6 days. Regarding education or training type majority of the respondents, 273 (70.5%) were trained on a regular program basis. The majority of study participants 306 (79.1%) had a feedback system in their organization. Regarding organizational communication, 266 (68.7%) was good. About 282 (72.9%) of the respondents had a job description. In terms of the method of assignment to position, 193 (49.9%) of respondents had their assignments made by facility workers. . Among the respondents, 303 (78.3%) had an opportunity to share with peers (Table 2).
Training and work-related characteristics among case team leaders and managers of South Wollo Zone Health Facilities, Ethiopia, 2021 (n = 387).

Governance practice
The overall good governance practice among the study participants was found to be 37.98% (95% CI: 33.1, 42.9) whose mean score above 60. Almost 38% of study participant were found to practice good governance in the health sector in the study area.
Factors associated with governance practice
The bi-variable analysis result showed that sex, history of training, type of training institutions, having feedback mechanism, availability of job description, opportunity to share with peers, political interference, and age were significantly associated with governance practice at p value <0.25.
In multivariable analysis history of training, availability of job description, opportunity to share with peers, political interference, and age were significantly associated with governance practice.
The odds of good governance practice (i.e. a governance practice score above 60) for those having a history of training related to governance practice were 7.92 times higher compared with those who had no history of having training (adjusted odds ratio (AOR) = 7.92, 95% confidence interval (CI): 4.04, 15.51).
The odds of good governance practice for case team leaders and managers who had job descriptions were 2.06 times higher than those who had not a job description (AOR = 2.06, 95% CI: 1.03, 4.09).
The odds of good governance practice for those having the opportunity to share with peers were 6.64 times higher as compared to those not sharing with peers (AOR = 6.64, 95% CI: 3.02, 14.62).
The odds of good governance practice among those who had political interference were reduced by 60% as compared to leaders and managers who had no political interference in their work environment (AOR = 0.40, 95% CI: 0.22, 0.71).
Leaders and managers whose ages were less than 25 years had 87% lower odds of practicing good governance as compared to those 46 years old and above (AOR = 0.13, 95% CI: 0.02, 0.77) (Table 3).
Factors associated with governance practice in binary and multivariable logistic regression among case team leaders and managers of South Wollo Zone Health Facilities, Ethiopia, 2021 (n = 387).
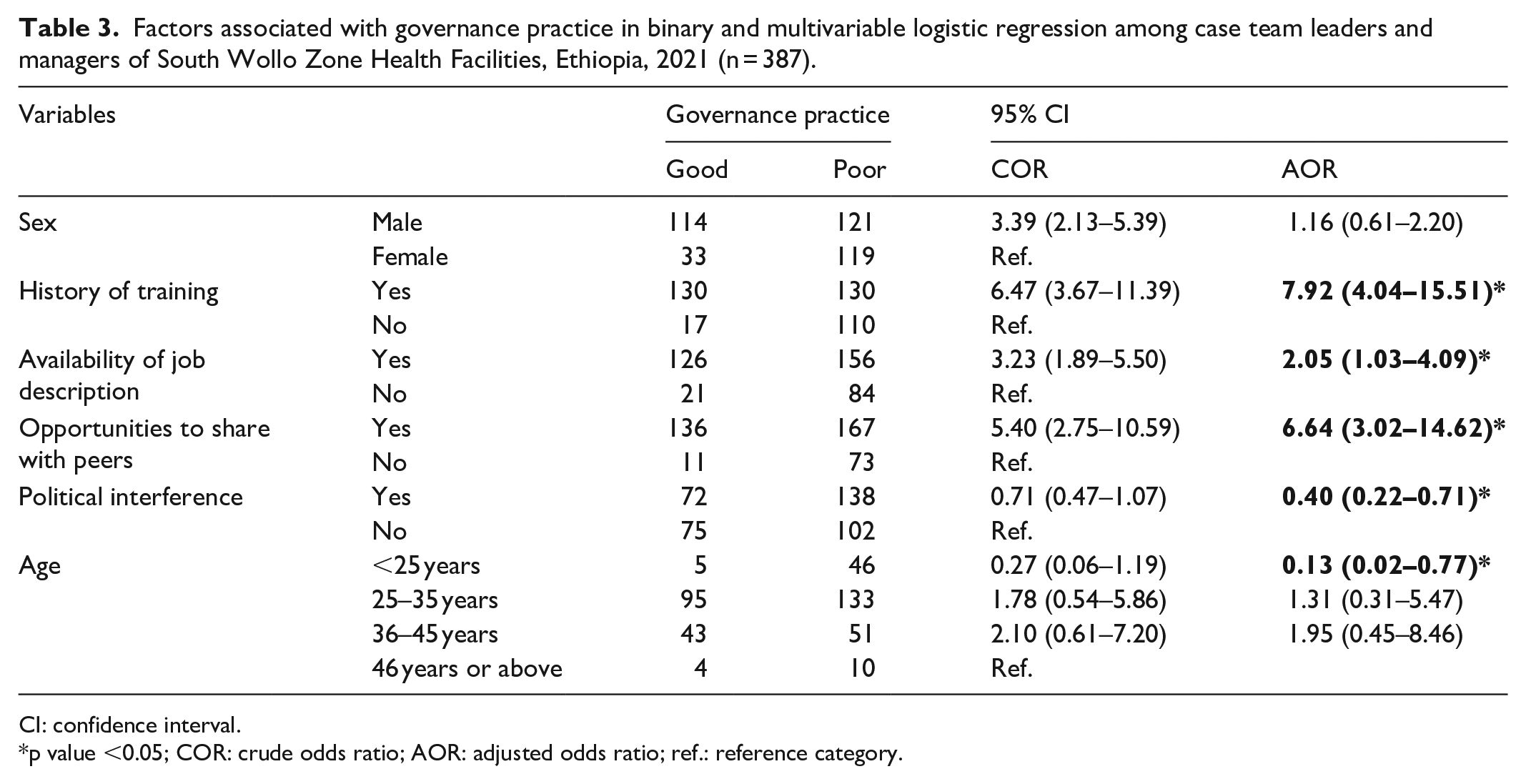
CI: confidence interval.
p value <0.05; COR: crude odds ratio; AOR: adjusted odds ratio; ref.: reference category.
Discussion
About 38% (95% CI: 33.1, 42.9) of participants had good health care governance practice (i.e. a health care governance score above 60), which was a lower percentage than other countries.
It was lower when compared with a study conducted in different countries. A study conducted in western Harergie, Ethiopia reported that 54.6% 16 of primary health care unit (PHCU) managers had good governance, and hospital-based studies in Ethiopian showed Tikur Anbessa Specialized Hospital (57%), Gondar University Hospital (51%), Ayder Referral Hospital (72%), Hawassa Referral Hospital (57%), Welaita Sodo University Hospital (54%), Dilla University Referral Hospital (51%), Jimma University Specialized Hospital (62%), Harar Hiwot Fana Specialized Hospital (59%), and Adama Hospital (63%). 10 The possible reason for the difference might be as some kinds of the literature showed due to lack of coordination among human resources, finance, and planning departments in implementing incentive packages, less availability of work-area health-protective supplies, unsafe and unsuitable working environments.
The governance practice in Arsi University, Asela Referral Hospital, 18 and a study in Addis Ababa 19 were similar to our study findings.
Having had a history of training in governance practice was a significant factor in practicing good governance. This finding was supported by a study conducted in Ethiopia. 20 The conceptual map and assumptions of training are to improve the knowledge and skills associated with leadership, and management practices of case team leaders and managers in primary health care settings that significantly improve individual and team performance.
Job descriptions and opportunities to connect with colleagues in the workplace were predictors of governance practices. These perspectives were supported by studies conducted in western Harergie. 16 This might be due to the job description serving as a reminder for both practical and legal reasons, with the specific skills and abilities required for the job, or the environmental impact and corporate governance associated with the job. In other respects, colleagues have had a significant impact on promoting accountability, self-esteem, and transparency. The exchange of experience provides an opportunity to train/learn people who can fulfill their citizens’ obligations, adapt to the workforce, contribute to the creation of a better working environment for all, and foster interpersonal relationships that lead to mutual trust. In addition, it promotes multiculturalism, which can lead to good governance practices. 21
Participants who had political influence in the workplace were influenced by governance practices. This result is consistent with the study conducted in Nigeria. 22 This might be due to the immaturity of the political systems of most African countries, including Ethiopia.
Leaders and managers whose age was less than 25 years were less likely to practice good governance as compared to 46 years and above counterparts. This finding is also in-line with the study conducted in the sub-Saharan region. 16 This might be due to age increases the level of tolerability, decision-making ability, and learning from experience was also increased.
A study in Dukem Town, Oromia Regional state revealed that some leaders lacked knowledge, competence, and skills, and they lack monitoring and evaluation capabilities which in turn affects good governance practice. 23 This is in fact that change can never exist in the absence of knowledgeable and skilled individuals.
Limitation of the study
It lacks a qualitative component that may augment the result and explain the reasons for the factors in the depth of information.
It was a self-administered data collection method that might be exposed to response bias.
Conclusion
In this study, the overall governance practice was lower than the national target. Factors increasing good governance scores were having a history of training, availability of a job description, and the opportunity to share with peers. Factors decreasing good governance scores were younger age and political appearance. Managers could implement training, write job descriptions, and encourage sharing with peers to improve governance of the health sector for the overall improvement of the health system.
Footnotes
Acknowledgements
First of all, we would like to thank all the study participants for their cooperation in providing the necessary information. We also appreciate the collaboration of managers and coordinators at various levels. We also thank the data collectors and supervisors for their dedication and effort during data collection. Last but not least, we provide our deepest gratitude to Wollo University for giving us this chance to research this area.
Author contributions
G.S. has been involved in the conception, design, analysis, interpretation, and article writing. A.F., T.Y., M.D.A., N.G., N.W., and M.G.C. were also involved as a team in the design, analysis, interpretation of the data, and article writing, editing, and review. All authors read and approved the final article for publication.
Availability of data and materials
All the data supporting the findings are within the article.
Consent for publication
All the authors consented to the publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Ethical Review Committee /ERC/ of Wollo University, College of Medicine and Health Sciences, Wollo University, Ethiopia. (Reference ID: CMHS 474/02/13 on 05/06/2013).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study fund was covered by the primary author as a self-sponsor his postgraduate program (Master’s degree program).
Informed consent
Informed voluntary written consent was obtained from all participants. The study was conducted on adults who can give consent to participate. Participants’ information was kept confidential using anonymous questionnaires and use of codes. Personal privacy and cultural norms were respected. The respondents were informed of their right not to participate in the study or withdraw from the study at any time without affecting their participation in the HDSS.