
Abstract
Objective:
The study objectives were aimed to highlight the areas where public awareness is needed to enhance preventive practices among the public. Hence, to avoid the spread of virus in public settings. In addition, the study has provided compelling data and evidence on the coronavirus disease-2019 trend for health policymakers to make strategic decisions.
Introduction:
The coronavirus disease-2019 is a highly contagious respiratory disease caused by severe acute respiratory syndrome coronavirus type-2. The disease has spread across the globe. In Afghanistan, thousands of confirmed cases with hundreds of deaths have been reported. In addition, due to insufficient healthcare workforce, insecurity, fragile healthcare infrastructure, low coronavirus disease-2019 vaccination and low testing capacity, the true nature of the pandemic is unlcear.
Method:
An online survey of the general population in Afghanistan was conducted from April-May 2021. Convenience sampling technique was used to recruit the respondents. Social media platforms were used (WhatsApp, Twitter and Facebook Messenger) to disseminate the electronic survey instrument. Written informed consent was taken from the participants before the filling questionnaires. Data collection was guided through a self-administered questionnaire developed by the researchers according to the World Health Organization guidelines. The sample size was calculated using EPI software. The inclusion criteria were being 18 years or older and having access to the Internet to fill out the online questionnaire. IBM SPSS Statistics version 25.0 was used for analysis. Descriptive statistics (frequencies, percentages) and bi-variable (chi-square) analyses were done. A p value of <0.05 was considered significant at a 95% confidence interval.
Results:
From 1094 respondents, 78% were male. The majority of respondents were aged ⩽30 years and had an undergraduate education. Nearly 1 in 3 participants were healthcare workers, and 70% lived in households with five or more family members. Overall, 70% of the respondents reported good preventive practices. The majority of the participants reported covering their mouth and nose while coughing and sneezing and cleaning their hands regularly and using alcohol. Meanwhile, 80% of the participants wore a mask when going outside. Moreover, people with post-graduate education had a higher level of preventive practices than those with an undergraduate education.
The results of logistic regression revealed participants residence in Kabul, healthcare workers, family size less than 5, avoid meeting people outside, gender, and avoiding 3Cs, were the significant determinants of adhering to good preventive practices.
Conclusion:
Generally, the public in Afghanistan followed infection prevention rules. However, certain areas require further improvement, such as observing social distance and avoiding shaking hands when meeting others. Negligence of these prevention practices can lead to an increase in infection transmission among people. Public awareness should be continued to keep the people supportive of the government policies.
Introduction
The coronavirus disease 2019 (COVID-19) is a highly contagious respiratory disease caused by severe acute respiratory syndrome coronavirus type-2 (SARS-COV-2). The disease has spread to more than 190 countries since it emerged from Wuhan, China, in 2019. 1 The virus spreads rapidly from an infected person to another person through direct or indirect contact via a sneeze or cough. 2
As of 23 December 2021, there have been 157,878 confirmed cases of COVID-19 in Afghanistan, with 7346 deaths. However, studies estimate that the actual number of infections might be higher than what is reported. 3 Serious efforts, including lockdown, gathering, and travel restrictions, raising awareness through public health education, and hygiene promotion programs, have been implemented to control the outbreak effectively. 4 Nevertheless, inadequate facilities and insufficient healthcare workforce, lack of personal protective equipment, insecurity, and ongoing conflicts make it difficult to reach the aforementioned target. 5
Governments and health departments enforced nationwide lockdowns, social distancing, travel restrictions, precautionary measures, and preventive guidelines to curb the disease. 6 Despite all these measures, the fight to flatten the curve of COVID-19 is still taking a huge toll on governments and health systems, particularly in low- and middle-income countries. 7
The World Health Organization (WHO) issued several infection prevention and control precautions to reduce the risk of exposure to COVID-19, 8 such as wearing a face mask, hand sanitizing, social distancing, avoiding close contact with people, especially in crowded areas, covering mouth and nose during coughing and sneezing, and use of personal protective equipment. 9 These protocols and recommendations are continuously updated by the WHO in the light of available evidence.
In the context of Afghanistan, it was predicted that the healthcare system would be overwhelmed by the pandemic. Therefore, authorities from the early days diverted all resources to the containment of the pandemic. Healthcare workers were less trained, and fewer hospital beds were available for the COVID-19 patients. Nonetheless, the second wave of the pandemic came with more dire implications. Lack of beds, oxygen, and the infection of healthcare workers plighted the healthcare system. Rise in the food stocks, and insecurity were also some of the key components of the second wave of the pandemic. 10
The third pandemic wave started when the country was amid political instability. This was correlated with the fast spread of the virus, lack of oxygen, delta variant, and food insecurity. Moreover, the impact of insecurity was rising, and the healthcare workers were suffering from psychological distress. Therefore, vaccination, which is the most advanced tool for preventing the spread of the pandemic, has started in the country. However, in Afghanistan, there are significant challenges that cast troubles to the safe vaccination of the people, such as geographical barriers, conflicts, and illiteracy. 11 In a previous study conducted among the Afghan public, a significant proportion of people (37%) showed hesitancy toward COVID-19 vaccination. 12 This calls for actions on educational and social media campaigns.
Over the years political instability has rooted in Afghanistan. Conflict and war has been every day experience for the people of Afghanistan. The result of such conflicts have led to undereaching of health services in different terrorities of the country. Concurrently, the country is suffering significant challenges in the healthcare system. This instantly started after the United States and international allies’ withdrawal, which has put forth dilemmas for the whole population. The largest health services provider, “Sehatmandi,” has stopped functioning properly due to the lack of funding. As of 23 December 2021, a total of 4,572,319 vaccine doses have been administered. However, during his visit to Kabul, the WHO director said that some COVID-19 hospitals have stopped functioning, and there are unused doses of vaccines in the country. Therefore, swift actions are needed to ensure vaccines are being used and hospitals are operating.
Given the unique context of the Afghanistan, and the low scale of COVID-19 vaccination in the country, reliance on prevention strategies is the most effective way forward. Hence, observing infection prevention protocols during the political instability and new era seems to be the most effective strategy to decrease the infection rates in such a resource-limited setting. Moreover, due to the lack of access to original data from the ground from different parts of the country, we relied on online survey as the most feasible option. Therefore, the main objective of this study was to investigate people’s compliance with infection prevention practices during the third wave of the pandemic to provide an updated insight into the situation and help policymakers design effective measures. This is important to highlight the areas where public awareness is needed to enhance preventive practices among the public and to provide compelling data and evidence on the COVID-19 trend for health policymakers to make strategic decisions.
Methods
Study design, sampling, and target population
This was an online-based cross-sectional survey of the general population from April till May 2021, in Afghanistan regarding their adherence to preventive practices during the third wave of the pandemic. Informed consent was stated in the first page of survey. Participants were not able to proceed without their consent. Participants were recuited through a non-probability convenience sampling. The sample size was calculated using Epi info7 software, based on the number of social media users in Afghanistan, accounting for 4.4 million of the general population. Assuming that 50% is the expected magnitude, using alpha error of 0.05, design effect equals 2 and margin of error 5%, the minimum required sample size was 768. The sample size was calculated using Epi info7 software. The eligibility criteria were being 18 years or older and having access to the Internet to fill out the online questionnaire. Respondents who did not consent to participate in the study and those who did not answer the entire questionnaire were excluded.
Survey instrument, tool administration, and data collection
An online, structured, and self-administered questionnaire was developed by the researchers according to WHO guidelines and preventive practices released in April 2021. 13 The survey tool comprised of three sections. The first section highlighted the general purpose of the study and asked the participants to provide informed consent before answering. The second section included demographic characteristics of respondents, that is, age, sex, education, residence, marital status, occupation, and family size. The third section included 10 questions about preventive practices toward COVID-19 to evaluate compliance with preventive guidelines. To increase the validity and credibility of the findings, the content of the questionnaire was validated by three experts in the field, and their comments were integrated into the questionnaire. Moreover, the questionnaire was pilot tested on 30 non-probability selected individuals compared to the planned sample size to ensure it was legible, reliable, and understandable. The data from the pilot study were not included in the final analysis. The final questionnaire was distributed to respondents across social media platforms (Facebook, Twitter, and WhatsApp) during April to May 2021.
Ethical considerations
Ethical approval for this study was obtained from the Research and Ethics Committee of the Department of Microbiology, Kabul University of Medical Sciences (Approval code: KUMS/RECMD – 096). All aspects of this study comply with the ethical standards of the relevant national and institutional committees on studies involving human contacts and with the Declaration of Helsinki released in 1975 and subsequent revisions.
Statistical analysis
Microsoft Excel 2019 and IBM SPSS Statistics version 25.0 was used for data analysis. Microsoft Excel was used for editing, sorting, and coding and then excel file was then imported into SPSS software. Descriptive statistics (frequencies, percentages), bi-variable (chi-square) analyses and binary logistic regression analyses were done. The frequency of each items described. Overall good and poor preventive practices were scored and calculated. For preventive practices, scores of <60% were classified as poor practices, and ⩾60% were classified as good practices, similar to other studies.14,15 A p value of <0.05 was considered significant at a 95% confidence interval.
Results
A total of 1094 people responded to the questionnaires, displaying a satisfactory response rate of 91.40.
Sociodemographic analysis
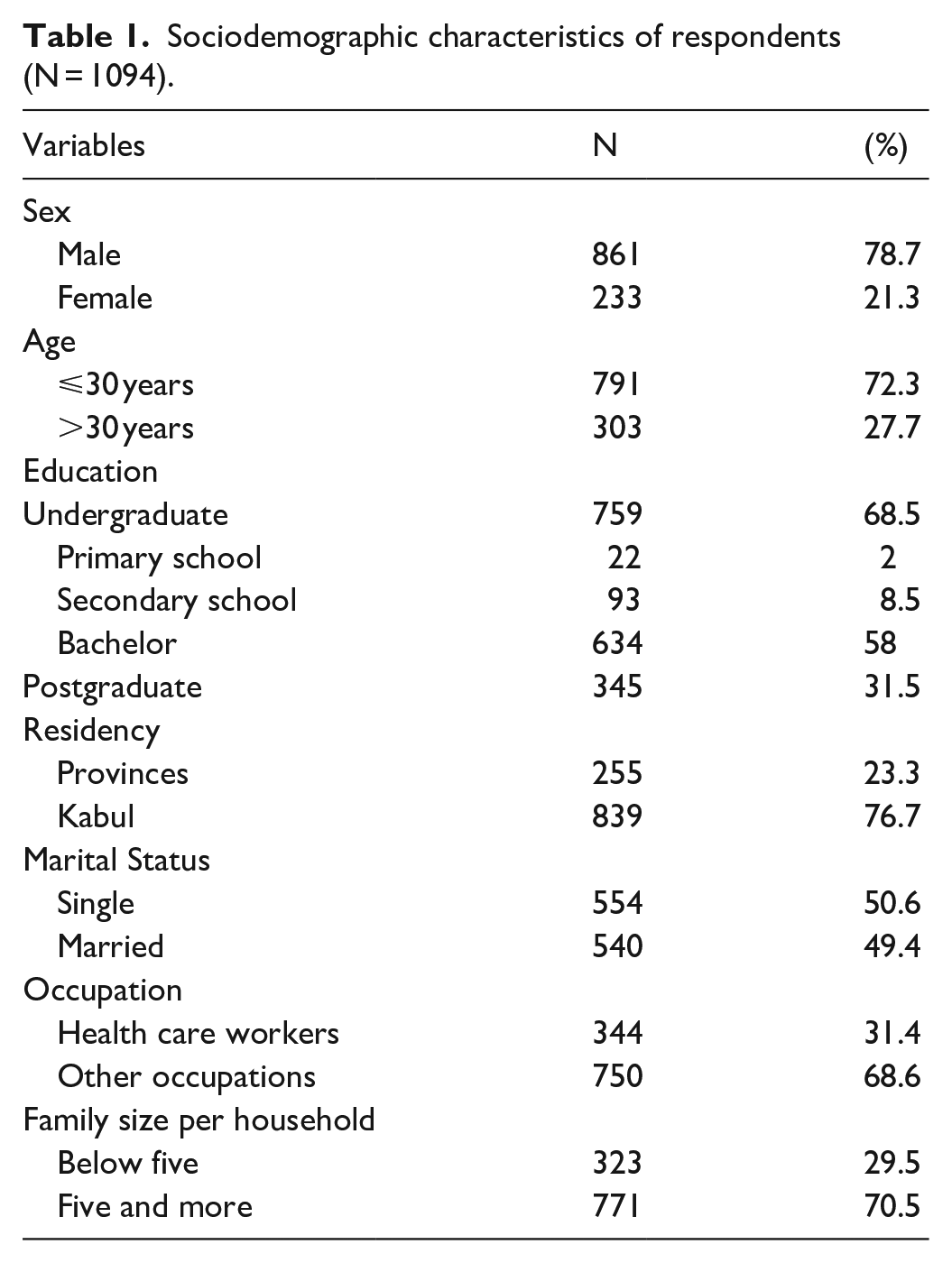
Of all the respondents, 78.7% were male. The majority of respondents were aged ⩽30 years and had an undergraduate education (68.5%). Almost half of them were single and 3 out of 4 participants lived in Kabul, the capital of Afghanistan. Nearly 1 in 3 participants were healthcare workers and 70% were living in households with five or more family members (Table 1).
Sociodemographic characteristics of respondents (N = 1094).
Preventive practices of respondents against COVID-19
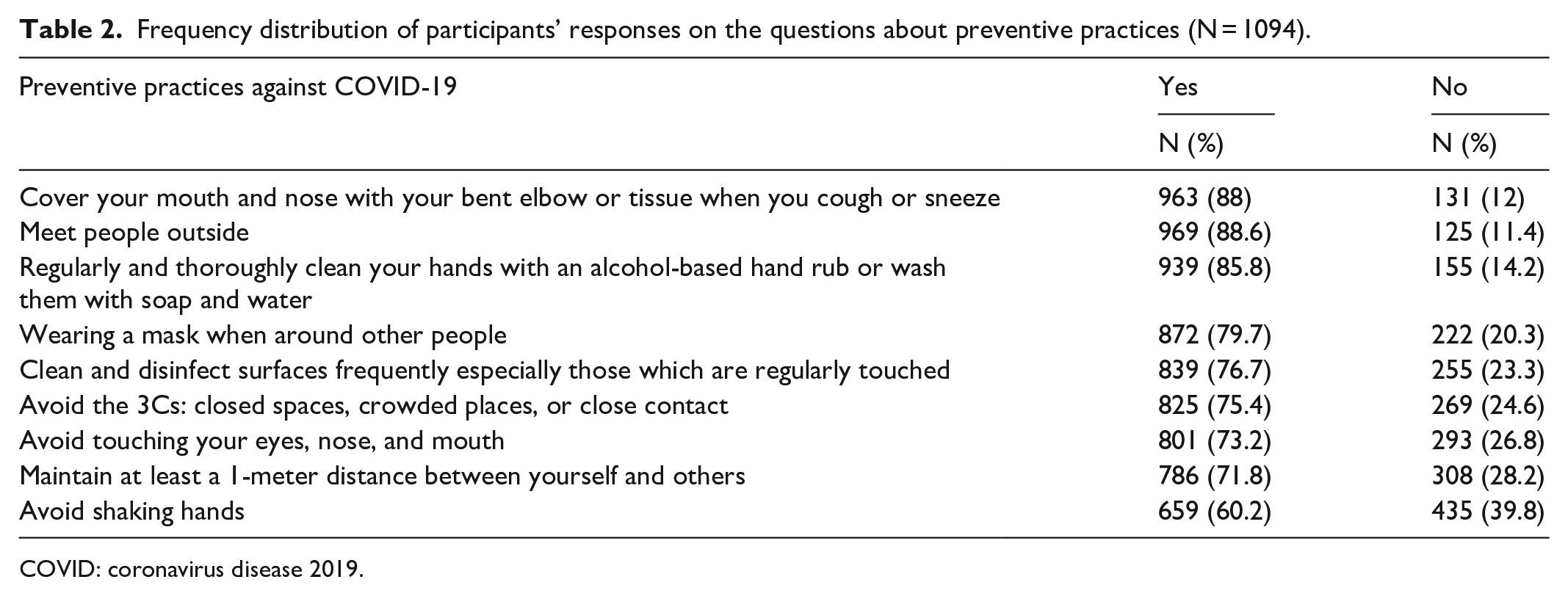
Table 2 shows the frequency of preventive practices reported by the study population. The majority of the participants reported covering their mouth and nose while coughing and sneezing and cleaning their hands regularly and thoroughly with an alcohol-based disinfectant or soap and water (88% and 85.8%, respectively).
Frequency distribution of participants’ responses on the questions about preventive practices (N = 1094).
COVID: coronavirus disease 2019.
Almost 80% of the participants wore a mask when going outside. Furthermore, three out of four respondents reported cleaning and disinfecting surfaces frequently, especially those which are regularly touched, avoiding the 3Cs (closed spaces, crowded places, or close contact); and avoiding touching their eyes, nose, and mouth. Slightly more than two-thirds of the study participants reported maintaining a distance of at least 1 m with others, and only 60% of them avoided hand-shaking while meeting people (Table 2).
Overall, 768 (70.2) respondents reported good preventive practices. Table 3 shows the results of bi-variable (chi-square) analyses to find out significant associations of good preventive practices. There was no significant association between male and female participants concerning preventive practices against the COVID-19. The frequency of good preventive practices was significantly higher in participants more than 30 years old as compared to those aged 30 years or less (74.5% and 68.4%, respectively; p = 0.035). People with post-graduate education had a higher level of preventive practices than those with an undergraduate education only (74.8% and 68.1%, respectively; p = 0.025). Participants who lived in the capital of Afghanistan, that is, Kabul, had a significantly higher level of preventive practices as compared to those who lived in provinces (72.2% and 63.5%, respectively; p = 0.008).
Results of bi-variable (chi-square) analyses of the sociodemographic variables with preventive practice (N = 1094).

For preventive practices, scores of <60% were classified as poor practices, and ⩾60% were classified as good practices. Scores are calculated based on preventive practice items. A p value of <0.05 was considered significant at a 95% confidence interval.
Furthermore, the frequency of preventive practices among healthcare workers was significantly higher as compared to non-healthcare workers (76.5% and 67.3%, respectively; p = 0.002). Participants who did not meet people outside had a higher level of good preventive practices than those who met people outside (78.4% versus 69.1%; p = 0.033). Finally, households with less than five family members reported a significantly higher percentage of preventive practices as compared to those with five or more family members (76.8% and 67.4%, respectively; p = 0.002; Table 3).
In binary logistic regression analyses, residents in Kabul, healthcare workers, family size less than 5, and avoid meeting people outside retained their role as independent contributors to good preventive practices, whereas age and educational level did not maintain their independent roles, and hence dropped from the model. Furthermore, logistic regression analyses added male sex (p = 0.02; odds ratio (OR) = 1.72, 95% confidence interval (CI) = 1.21–2.45) and avoiding 3Cs (p = 0.04; OR = 1.44, 95% CI = 1.0–2.05) as independent contributors to good preventive practices against the COVID-19 (Table 4).
Results of binary logistic regression analysis for determinants of adherence with good preventive practices among the study population.

AOR: adjusted odds ratio; CI: confidence interval.
1 = reference category.
Discussion
This survey provides a unique assessment of the public adherence to preventive practices amid the COVID-19 pandemic. To the best of our knowledge, this is the first survey that explores the preventive practices among the public in Afghanistan during the third wave of the pandemic.
Over time, due to extreme unstable context of Afghanistan, the overview of health issues on ground has become increasingly difficult to report. It has been reported that in areas under the control of Taliban and other groups, there have been delays or hurdles in providing health facilities. This has affected the true burden of health disease in the country. Given that Afghanistan underwant a sudden political transition, the healthcare stopped functioning properly which led to dire consequences in the country. 16 Major examples were the closure of COVID-19 vaccinaion. This was terrible moment as the country was already striving to vaccinate its population. Moreover, the entire population was struggling with severe economic crisis and displacement inside and outside of the country. 17 This survey was undertaken in such a fragile environment to assess the preventive measure. This is because of the fact that preventive measures seem the most effective way of controlling the pandemic.
In this study, 70% of the respondents have reported good preventive practices against COVID-19. Our findings are in line with a study conducted in Cameroon, where over 60.8% of the public were taking good practices against the COVID-19 pandemic. 18 Similarly, in a study conducted in Saudi Arabia, over 90% of the participants were taking good practices. 19 Moreover, a study in Sudan showed that 87.2% of the general population were willing to adhere to COVID-19 preventive measures. 20 The difference in reported adherence to COVID-19 precautionary measures between counrties could be due to the extent and outreach of awareness raising campaigns and health education programs implemented in different contexts.
In this study, the majority of the participants reported covering their mouth and nose while coughing and sneezing and cleaning their hands regularly and thoroughly with an alcohol-based disinfectant or soap and water. These results points to the effectiveness of health education message in spreading the awareness about the deasese and its precautionary measures. The findings are similar to a study conducted in Ethiopia in which all participants indicated high compliance to precautionary measures, that is, 97.1% washed their hands, 87% avoided social events, 91% used hand sanitizers, and 56.5% wore face masks when going out of the home. 21
Slightly more than two-thirds of the study participants reported maintaining a distance of at least 1 m with others, while almost one-third of them did not report practicing this. As the COVID-19 can spread to the environment up to 2 m, 22 hence, not following social distance could increase the risk of transmission, in addition to this. Furthermore, about 40% of the respondents did not report avoiding hand-shaking when meeting others, this could also increase the risk of transmission among the public. overall, this area needs more attention from the stakeholers to implement social distancing measures in general places and to increase the public awareness adherence to these measures.
We also investigated factors associated with good preventive practices among participants. Gender difference did not show any significant association with adherence to preventive practices. This might indicate that male and female participants were equally concerned and committed to preventive practices against the COVID-19. However, in the regression model, after adjusting for covariates and confounders, male participants were nearly two times more likely to adhere to good preventive practices than do females, this could be due to the greater number of males included in this study. In contrary to this finding, many other studies reported that female participants were more compliant with health-related guidelines and preventive practices especially during the COVID-19 pandemic.23–26
In our study, we found that age was found to have a significant association with follwing preventive practices. Participants older than 30 years reported significantly higher levels of preventive practices. This may be attributed to the higher level of mental maturity and education of people older than 30 years. Consequently, health education campaigns should focus on younger age groups. In support to this finding, different studies also have reported that age was a significant predictor of compliance with preventive practices against COVID-19.21,27 On the contrary, an international survey found no association between age and observing rules. 24
The study findings also indicated that participants with a post-graduate degree and those living in the capital of Afghanistan reported significantly higher levels of preventive practices. This could be explained by the higher levels of trust in science, which is associated with higher compliance with infection prevention and control practices against COVID-19. 28 Post-graduates hold a high proportion of knowledge, awareness, and practice toward COVID-19. They could also play a role in awareness among the people. Moreover, people living in provinces might be affected by false information and less outreach to health facilities than those who are living in the capital province.
Furthermore, the frequency of preventive practices was significantly higher among healthcare workers compared to other employment categories. Similar studies conducted in Nigeria, Iran, and Bangladesh have revealed similar findings among healthcare workers. This could be explained by the high proportion of knowledge, attitudes, and practice among healthcare workers compared to the public.29–31 In contrast, a study conducted in Ethiopia revealed that healthcare workers’ adherence to COVID-19 preventive practices during intrapartum care provision was lower. 32 This raises the point that awareness regarding preventive practices should be put forth for everyone.
The household number was also significantly associated with preventive practices among the study group. Households with less than five family members reported a significantly higher percentage of preventive practices as compared to larger households. Households with lesser members might have better opportunities to educate their members and provide necessary items required for disease prevention, such as masks, disinfectants, and so on. It is generally understood that a more educated family will comply better with relevant preventive and treatment measures. 33
Strengths and limitation
This study has several strengths and limitations. The paucity of data on healthcare workers’ and general populations’ adherence to COVID-19 during the third wave is considered a big challenge for health policymakers in decision-making. Our study comprises both the general population and healthcare workers, thus, it would be considered a valuable addition to the literature. In addition to this, this study highlights the importance of public awareness regarding preventive practices, which is considered crucial in times when there is a shortage of vaccines. On the contrary, our study was carried out during the third wave of COVID-19, which was associated with pervasive political instability and psychological challenges. Therefore, it might not depict the true picture of the pandemic. Further studies are needed to highlight the depth of the COVID-19 pandemic among healthcare workers and the general population. The use of non-probability convenience sampling limits the generalization of study findings to the region of interest. Moreover, there might have been participants not participated in the survey due to the insecurity or fear of being exposed to problems. In addition, this was a web-based study. Hence, those who did not have access to the Internet are excluded, which means the study was affected by selection bias. Meanwhile, the self-reported adherence may not reflect the actual practice of participants, which means the findings might be affected by social desirability bias.
Conclusion
The study findings show that the people of Afghanistan are generally following infection prevention rules. The practices of wearing a mask and washing hands with an alcohol-based disinfectant or soap and water were good. However, certain areas require further improvement, such as observing social distance and avoiding shaking hands while meeting others. Negligence of these preventive practices can lead to an increase in the infection rate among the public. Public awareness should be continued to keep people supportive of the government policies. Social media, TV advertisements, and similar platforms may be used for this purpose.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221122399 – Supplemental material for Self-reported adherence to preventive practices during the third wave of COVID-19 in Afghanistan
Supplemental material, sj-docx-1-smo-10.1177_20503121221122399 for Self-reported adherence to preventive practices during the third wave of COVID-19 in Afghanistan by Arash Nemat, Mohammad Faiq Sediqi, Yasir Ahmed Mohammed Elhadi, Nahid Raufi, Mohammad Yasir Essar and Abdullah Asady in SAGE Open Medicine
Footnotes
Acknowledgements
This study is available on the preprint service.
Author Contributions
A.N. wrote the manuscript draft and developed the original idea; Y.A.M.E. developed the original draft; A.A. contributed in the analysis, discussion, and proofreading; M.F.S., Y.A.M.E., N.R., and M.Y.E. assisted with the design and distribution of the questionnaire and revision of the manuscript. All authors have read and approved the final manuscript. A.N. is the corresponding author. All authors meet the standards described in the ICMJE authorship guidelines.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
Ethical approval was obtained from Department of Microbiology, Kabul University of Medical Sciences. Respondents’ participation was completely consensual, anonymous, and voluntary.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.