
Abstract
Good knowledge, awareness and preparedness regarding coronavirus disease 2019, among community pharmacy practitioners (CPPs), will enable them to provide correct information and support to patients, convey instructions from the public health authorities and protect their own health.
Objective:
The aim of this study was to determine knowledge, awareness and preparedness regarding coronavirus disease 2019 among CPPs working in Kathmandu, Nepal.
Methods:
A cross-sectional study was conducted using a convenience sampling method from 10 February to 25 March 2020. Data were analysed descriptively, and one-sample independent t-test and one-way analysis of variance were used to compare scores among different subgroups of respondents (p < 0.05). Post hoc analyses (following analysis of variance) were done using the Bonferroni test.
Results:
A total of 81 CPPs participated. Mean ± standard deviation age was 26.70 ± 5.29 years. Majority of the respondents were male (64.2%). Many CPPs (40.7%) had work experience between 1 and 5 years. Almost half (45.7%) had an educational qualification of Diploma in Pharmacy. Significant differences in knowledge (p = 0.022) and preparedness (p < 0.001) were found among individuals with differing levels of work experience. Similarly, a significant difference was found between knowledge-preparedness and work experience (p = 0.022 and p < 0.001), location of pharmacy (p < 0.001) and educational qualification (p = 0.031). Awareness (p < 0.001) and preparedness scores (p = 0.049) were different among community pharmacies with the different number of medicines available.
Conclusion:
Knowledge was found to be higher in CPPs with a work experience of more than 5 years. CPPs working at larger community pharmacies were more aware and prepared. CPPs’ knowledge, awareness and preparedness should be evaluated more widely and strengthened.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19), caused by a virus initially known as 2019-nCoV and now called Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2), has been declared as a global health emergency by the World Health Organization (WHO) on 30 January 2020.1,2 In December 2019, SARS-CoV-2 was identified and reported from Wuhan, China. Thus far, the number of confirmed cases and deaths as of 9 October 2020 was nearly 37 million and 1 million, respectively. 3 On 25 January 2020, the first case of COVID-19 was diagnosed and reported in Nepal.4,5 Till 10 October 2020, 105,684 cases have been confirmed in Nepal and the death toll stands at 614. 6
Many people in Nepal still depend on community pharmacies, local practitioners (mainly from other systems of medicines), paramedical personnel and community pharmacy practitioners (CPPs) for the treatment of healthcare ailments.7,8 The number of community pharmacies exceeds the total number of health centres. 7 The number of pharmacy professionals is, however, still inadequate for delivering quality services related to pharmaceutical care.7,9 CPPs work as dispensers in community pharmacies and are mainly assistant pharmacists and pharmacists, and they also counsel patients.
Community pharmacy practice in Nepal requires improvement. Department of Drug Administration (DDA) 10 is the national drug regulatory authority founded to implement the Drugs Act 2035 (1978) and its regulations. According to the Drugs Act 2035 (1978), 10 three levels of pharmacy personnel can run a pharmacy in Nepal. They are pharmacist, assistant pharmacist and a professional person. Pharmacist and assistant pharmacists are individuals who have graduated in pharmacy and diploma in pharmacy, respectively. A ‘professional person’ is an individual who possesses the recommended requirement or qualifications by DDA. 10 The recommended requirement or a qualifications of ‘professional persons’ are those who have completed the required training, 11 and this was a measure adopted when the pharmacist and assistant pharmacists were not common in Nepal. However, this orientation training programme has now been discontinued due to the increasing number of diploma and graduate pharmacists. The curriculum of pharmacy is mainly focused on industry, medicinal chemistry and hospital pharmacy. Community pharmacy is less focused on the curriculum. Training opportunities, continuing pharmacy education and continuing professional developments for CPPs are still lacking in Nepal. According to the pharmacist Ranjit, 11 community pharmacy is less explored by the pharmacists comparing to other fields of pharmacy such as hospital and industry.
Except the three pharmacy personnel mentioned in the Drugs Act, other paramedical personnel such as health assistants (HAs), community medicine assistant (CMA), nurses and auxiliary nurse midwife (ANM) also work in community pharmacies. Nurses, CMA and HA are not appropriate personnel to run a community pharmacy in Nepal. Only assistant pharmacist and pharmacists can register at Nepal Pharmacy Council and legally run a community pharmacy by taking permission from DDA. There are no publications, legal documents, or guidelines from any pharmacy professional and regulatory authorities in Nepal for handling civil crises though there have been guidelines provided by international agencies.12,13
There have been many studies highlighting the role of pharmacists in disasters such as earthquakes, infectious disease outbreaks and others.13–18 During a crisis, pharmacists can work as dynamic protagonists in several areas such as distributing drugs, providing information about drugs and diseases, and being involved in direct patient care. 15 Pharmacists have an essential role in the COVID-19 pandemic regarding counselling patients about prevention, providing information about diseases and medicines, and counselling during isolation and quarantine.19,20 Community pharmacies and community pharmacists can work towards decreasing the period of ‘community transmission’ of COVID-19, through proper case finding, recommendation and management (symptomatic) of likely cases. They can also provide patient education regarding self-care to reduce the spread of the disease, including hand hygiene, personal hygiene, correct use of face masks and evaluation of symptoms. 21 International Pharmaceutical Federation (FIP) also notes the vital role of CPP in this kind of catastrophe. 19 Also, a recent article concluded that they could play an essential role in reducing the spread of coronavirus. The first duty is notifying, counselling and educating the community. The second one is maintaining a steady supply of medications and personal hygiene products. The third one is the screening of suspected cases and appropriately referring a suspected case to the hospital. 17 In this unusual circumstance, CPP can be a strong pillar of the healthcare system, maintaining and providing a regular supply of patient’s medications and even personal protective equipment (PPE). Similarly, they can be proactive, ready to deliver skilled and competent pharmaceutical services to confirm medication safety and assume leadership in accepting pharmacy-associated responsibilities and COVID-19 pandemic control.15,22
Although some pharmacists are emerging as leaders, preparation for this kind of pandemic is often inadequate and sometimes absent. Good knowledge, awareness and preparedness regarding COVID-19 are fundamental to fight this pandemic. These will also enhance the implementation of government directives and help CPP be better prepared for the pandemic. Awareness is closely related to knowledge and refers to knowledge about a situation – in this case, the COVID-19 pandemic. Preparedness deals with how ready the CPP is to handle cases of COVID-19 and support the authorities in managing the pandemic. The main objective of this study was to obtain baseline data regarding the knowledge, awareness and preparedness of the CPP towards COVID-19 in Kathmandu district, Nepal, and to identify the factors influencing their knowledge, awareness and preparedness scores.
Methods and methodology
Study design, study period and site
This cross-sectional descriptive study was conducted at community pharmacies situated in Kathmandu district, one of the 77 districts of Nepal, situated in Bagmati Province and within which Kathmandu city (the capital of Nepal) is located. Kathmandu is a district with a large population and more facilities than other districts in Nepal. The data collection was performed from 10 February to 25 March 2020. This was a period when there were few cases of COVID-19 in Nepal and was the beginning of the epidemic in the country.
Study population, inclusion and exclusion criteria
The study population comprised community pharmacies located in Kathmandu district listed in the directory of DDA. According to DDA, there are around 13,000 registered allopathic community pharmacies in Nepal. In Kathmandu district, there were 2430 retail pharmacies. 23 During data collection, any CPPs involved in dispensing medicines, irrespective of their educational qualifications, and employed or working at community pharmacies were eligible to be included in the study.
Inclusion criteria
CPPs eager to take part and complete the consent form were enrolled in this study.
Community pharmacies which are registered with DDA. 23
Exclusion criteria
Community pharmacies dealing with other medicines such as herbal medicines and veterinary medicines, besides allopathic medicines, were excluded, as the maximum number of people visit pharmacies for allopathic medicines.
CPPs, who did not complete the questionnaire, were also excluded from this study.
The sample size was calculated, using the list of recorded community pharmacies, which was taken from the directory of DDA. With eight pharmacies as the sampling interval, using a convenience sampling method, 304 community pharmacies were calculated for the study. Due to the restrictions imposed by the pandemic, the survey had to be stopped after 81 pharmacies were completed.
Variables
Independent variables
The independent variables comprised of socio-demographic characteristics (age, gender) and work profile (working experience (in years), information resource used for drug information, educational qualification) of CPPs. The independent variable also included the different features of community pharmacies such as the number of medicines available in a pharmacy, the usual number of patients seen each day and location of community pharmacy.
Dependent variables
The dependent variables encompassed knowledge, awareness and preparedness regarding COVID-19 pandemic among CPPs employed in the community pharmacy.
According to the FIP, CPPs in both the unaffected and outbreak-influenced areas are frequently the primary point of contact with the health system for patients with health-related queries/concerns or needing information and dependable advice. 19
Based on prior studies done in other countries, hence, we chose knowledge, awareness and preparedness as the dependent variables. This study will produce the reference point of information on knowledge, awareness and preparedness of CPPs on COVID-19, which will add support in developing forthcoming interventional studies that will eventually help CPPs to prepare for COVID-19 and other infectious diseases.
Data collection tool
The questionnaire included questions on knowledge, awareness and preparedness about COVID-19 (Supplemental Appendix 1). At the time of conducting the study, there were few literatures available, so the study team developed a questionnaire based on available literature and information on COVID-19. The study team also discussed with a microbiologist while developing the questionnaire. The topics of interest while developing the instrument for data collection were community pharmacy service in the time of public health emergencies and community pharmacy preparedness to prevent and control the pandemic of COVID-19 and the sources of information used by CPPs during the pandemic. Standard resources such as the WHO website and FIP website were visited while gathering information on various aspects of COVID-19. The basic standard in developing a Likert-type scale 24 and knowledge, awareness and practice tool was followed. 25 There were questions and statements in four sections (demographics, knowledge, awareness and preparedness).
The questionnaire was pretested at two different study sites (Lalitpur and Bhaktapur districts, adjacent to Kathmandu district) that have demographic and related information comparable to the respondents of the main study. During the pretesting, we included assistant pharmacist, pharmacist, nurses, CMA and others (HAs) in the study. Content validation was completed by referring the questionnaire to subject experts (community pharmacist-1, clinical pharmacist-1, pharmacologist-1 and microbiologist-1). The questionnaire was tested for face validity among 10 community pharmacies. The data obtained during pretesting were not included in the study. Internal consistency was measured by calculating Cronbach’s alpha, 26 which was 0.70, demonstrating ‘acceptable’ reliability. The comprehensibility and ease of understanding of the questionnaire were also studied. After the pilot study, the questionnaire was revised after discussion with the research team and experts from pharmacy and microbiology. Some items were removed from the questionnaire.
Out of four sections, section 1 included eight items related to socio-demographic and related information of CPPs: age, gender, working experience, information resources used for drug information, qualifications, the usual number of patients visiting the pharmacy daily, number of brands of medicines in pharmacy and location of the community pharmacy. The number of brands here means the availability of different brands of the same generic medicine in the community pharmacy.
Section 2 included 11 items designed to evaluate CPP knowledge regarding coronavirus. A score of ‘2’ was given for each correct response, and a score of ‘1’ for an incorrect response. Section 3 comprised 9 items and aimed to study CPP awareness about coronavirus. Section 4 included eight items and aimed to assess CPP preparedness towards handling COVID-19. For sections 3 and 4, the Likert-type scale was used for obtaining the degree of agreement or disagreement with the statements. A score of ‘2’ was given for response ‘agree’, and a score of ‘1’ was given for responses ‘disagree’ and ‘neutral’. Some statements in the questionnaire were negatively phrased, and their scores reversed while calculating the total score.
Ethical approval
Before starting the study, ethical approval was obtained from the Institutional Research Committee (IRC) of KIST Medical College and Teaching Hospital, Gwarko, Lalitpur, Nepal (Ref. 2076/77/37). Written informed consent was obtained from individual respondents.
Data collection procedure
To collect the data from CPPs, the data collector (a student currently pursuing a Master’s in pharmacy) visited the community pharmacies personally and collected the responses. Before the study, a brief training was provided to the data collector by the principal investigator. The correct answers to the questionnaire were not provided to the data collector for avoiding bias. Before collecting data, the data collector provided an overview of the study, objectives, risks and benefits to the respondents. Written informed consent was obtained from those who agreed to participate. The respondents completed the questionnaires in the presence of the assigned data collector.
Scoring system
Demographic data and knowledge, awareness and preparedness of CPPs towards COVID-19 were analysed. For the knowledge section, each correct response was given a score ‘2’ and wrong response ‘1’. For awareness and preparedness, the degree of agreement with the statement was noted. For disagreement, we gave a score of 1, and for the agreement, we gave a score of 2. From section 3, that is, awareness section, statement number 6 ‘Coronavirus infection can be prevented by using a simple surgical mask’ was reverse scored. Similarly, from section 4, preparedness, statement number 1 ‘No action needs to be done in the absence of any symptoms of corona infection’, and statement number 6 ‘Antibiotics can be used to treat corona infection symptoms’ were reverse scored.
Statistical analysis
Statistical Package for the Social Sciences (SPSS), version 26 (SPSS, Inc., Chicago, IL, USA), was used for performing data entry and analysis. Normality of distribution of continuous variables was tested using the Shapiro–Wilk test at 5% level of significance. All categorical variables were presented as frequencies and percentages, and continuous variables were shown as mean ± standard deviation (SD). To compare knowledge, awareness and preparedness scores among different subgroups of respondents, one-sample independent t-test and one-way analysis of variance (ANOVA) were used. The p value <0.05 was considered statistically significant. Post hoc analyses were performed using the Bonferroni test.
Results
Demographic and related features of the CPPs
Table 1 shows demographic and related features of the CPPs. In total, 81 CPPs working at different community pharmacies completed the questionnaire. Mean ± SD age was 26.70 ± 5.29 years. Majority of the respondents were male (n = 52, 64.2%). Most (40.7%) had work experience between 1 and 5 years. Almost half (45.7%) of the respondents had an educational qualification of Diploma in Pharmacy.
Demographic and related features of the community pharmacy practitioners (N = 81).

SD: standard deviation; CIMS: Current Index of Medical Specialties; CMA: Community Medical Assistant; HA: health assistant; ANM: auxiliary nurse midwife.
Professional community pharmacy practitioners.
Others include HA and ANM.
Knowledge of COVID-19 among CPPs
Table 2 shows knowledge of COVID-19 among CPPs. Respondents obtained a mean score of 1.60 (maximum possible score = 2) for the statement ‘Corona is a virus species’. The lowest mean score was obtained for the response ‘The respiratory droplets can enter the mouths, noses or eyes of people who are nearby or possibly be inhaled into the lung’.
Community pharmacy practitioners’ knowledge related to COVID-19.
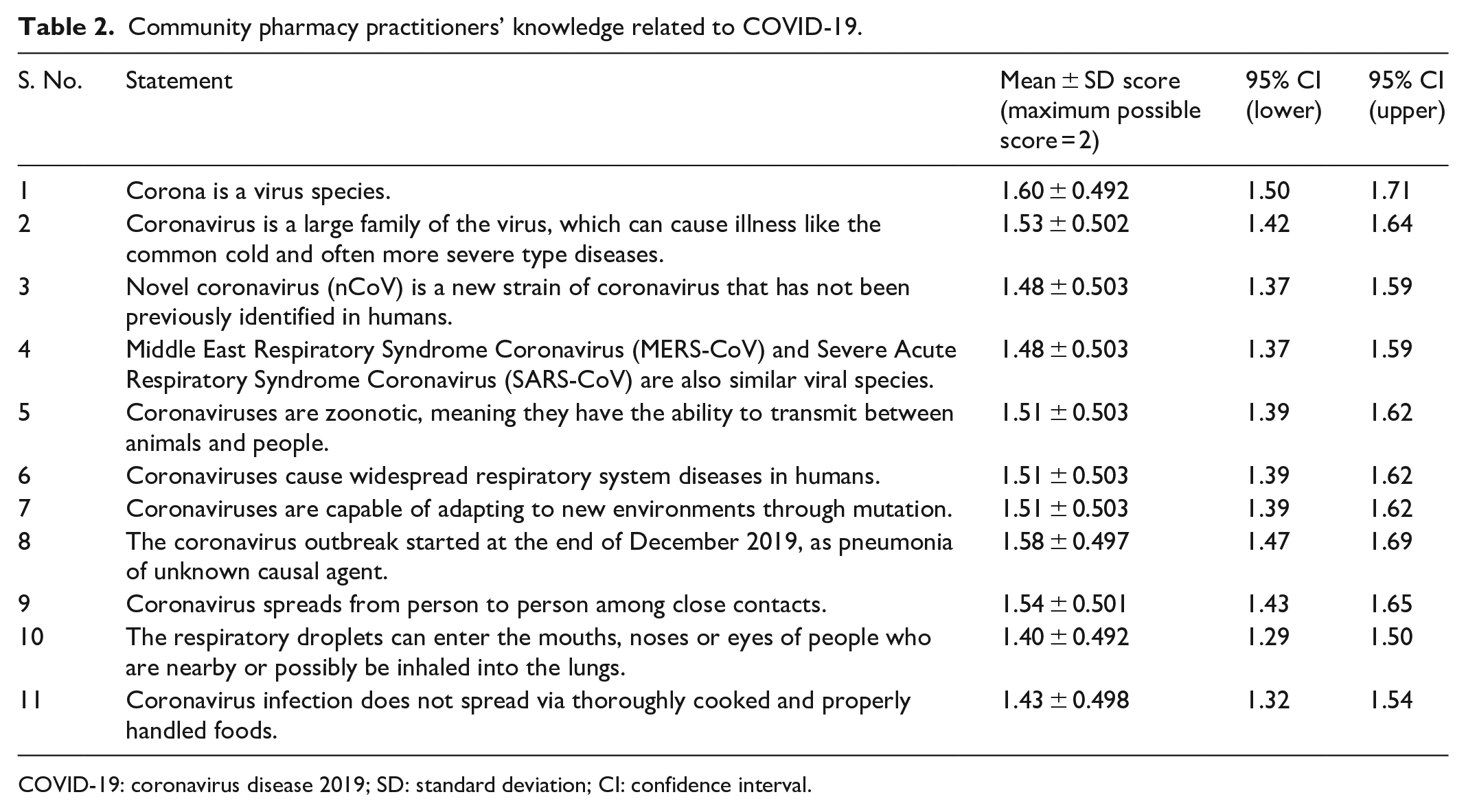
COVID-19: coronavirus disease 2019; SD: standard deviation; CI: confidence interval.
Awareness of COVID-19 among CPPs
Table 3 shows the awareness of COVID-19 among CPPs. Respondents scored highest for the response ‘The symptoms of coronavirus infection are nasal discharge, nasal block, fever and breathing difficulties’ and the lowest score was obtained for the response ‘Infection with coronavirus can be fatal’, suggesting that the respondents were unaware that the COVID-19 can kill the affected individual.
Community pharmacy practitioner’s awareness of aspects related to COVID 19..

COVID-19: coronavirus disease 2019; SD: standard deviation; CI: confidence interval.
The statement was negatively scored.
Preparedness with regard to COVID-19 among CPPs
Table 4 shows the preparedness with regard to COVID-19 among CPPs. A relatively high score was obtained for the response ‘If the patient has travel history from the infected areas with the symptoms, they should be advised immediate hospitalization’. The lowest score was obtained for the response ‘Pharmacies must have an adequate number of medicines to dispense for viral infections including corona’.
Community pharmacists’ preparedness towards handling of COVID 19 pandemic.

COVID-19: coronavirus disease 2019; SD: standard deviation; CI: confidence interval.
The statement was negatively scored.
Total knowledge, awareness and preparedness scores among different subgroups of respondents
Table 5 shows the mean scores among different subgroups of respondents. Significant differences in knowledge and preparedness scores were found among individuals with different levels of work experience, between knowledge-preparedness and work experience, location of community pharmacy and qualification of the dispenser. The awareness and preparedness scores were different among pharmacies with a different number of medicines available. Preparedness scores varied according to the number of medicines available and average number of patients visiting the pharmacy daily. No significant difference in terms of age group, gender, information resource used for drug information in the knowledge, awareness and preparedness score were noted.
Total knowledge, awareness and preparedness scores among different subgroups of respondents.

SD: standard deviation; CIMS: current index of medical specialties; CMA: community medical assistant; HA: health assistant; ANM: auxiliary nurse midwife; ANOVA: analysis of variance.
Bold values ighlight the statistical significance.
Independent-samples t-test at alpha = 0.05.
One-way ANOVA at alpha = 0.05.
Post hoc analysis showed no statistical significance.
Post hoc analyses of statistically significant variables
As tabulated in Table 6, a significant difference was noted between the scores obtained by respondents with a work experience of <1 year and >5 years (p = 0.020). Significance difference was also noted between the scores obtained by respondents working in a pharmacy near the hospital and far away from the hospital area (p = 0.002). Similarly, the difference was noted between the scores obtained by respondents working in the core city and near the hospital (p = 0.091). A significant difference was noted between the scores obtained by respondents working in pharmacies of different sizes, that is, with more than 500 medicines and 50–100 medicines (p = 0.001), 500–1000 medicine and more than 1000 medicines (p = 0.006) and with a work experience of <1 year and >5 years (p = 0.020).
Post hoc analyses of factors influencing community pharmacy practitioners’ knowledge, awareness and preparedness scores.

CMA: community medical assistant; HA: health assistant; ANM: auxiliary nurse midwife.
Bold values highlight the statistical significance.
Post hoc analysis using Bonferroni test at alpha = 0.05. Only the p values with statistical significance are shown in the table.
Others include HA and ANM.
Significant difference was noted between the scores obtained by respondents with a work experience of less than 1 year and 1–5 years (p < 0.001), and 1–5 years and more than 5 years (p = 0.026). Significant differences were noted in the educational qualifications of respondents between diploma in pharmacy and CMA (p = 0.001), Bachelor in pharmacy and CMA (p = 0.002) and CMA and others (p = 0.046). Similarly, about the size of the pharmacy, a significant difference was found between pharmacies with more than 1000 brands of medicines and with less than 500 brands of medicines (p = 0.045).
Discussion
During the time of COVID-19, many studies are being conducted to assess knowledge, attitude and practice among the different study populations.27–29 However, the current study provides the first portrayal of the knowledge, awareness and preparedness among CPPs working in Kathmandu district of Nepal, regarding COVID-19 pandemic.
Education for all CPPs is vital in a country like Nepal, where people prefer to visit community pharmacies for minor symptoms like cough, flu and fever rather than going to doctors which is quite expensive. Dealing with the complexity of COVID-19 requires that each CPPs acquires baseline knowledge and the minimum set of skills such as wearing PPEs to enable them to be aware, plan, take self-prevention measures and respond to COVID-19 patients.
In this study, the educational qualifications of the majority (45.7%) of dispensers working at community pharmacies were ‘Diploma in Pharmacy’ followed by ‘Bachelor in pharmacy’ (23.5%). The findings of the study are in contrast to other studies conducted at several community pharmacies in Nepal, where there was a lower number of diploma in pharmacy and Bachelor in pharmacy.8,30,31 The possible reason may be a growing number of graduating assistant pharmacists and pharmacists in Nepal.7,9 Diploma in pharmacy is a 3-year full-time course at the diploma level, and Bachelor in pharmacy is an undergraduate programme and a 4-year course. In community pharmacy practice, there is not much difference in the scope of work of these two categories. A person who has completed Diploma pharmacy works as an ‘Assistant Pharmacist’ and one with a Bachelor in pharmacy works as ‘Pharmacist’. In this study, around 30% of dispensers working at community pharmacies were found to be paramedics such as a nurse, CMA, HA, ANM and those with orientation programme not having a pharmacy degree, as most of the owner of community pharmacies hire CMA, HA and ANM as they work at lower salaries and are also skilled in doing minor surgeries, dressing and immunizations. The regulations in the country allow these professionals to dispense medicines as per the Drugs Act. 10 Before diploma in pharmacy became established, there was a 3-month orientation course which was offered to individuals already involved in running pharmacies and those who were interested in running one. According to Nepal Pharmacy Council (NPC), there are at present 2590 pharmacists, and 4847 pharmacy assistants registered. 9
We found nearly two-thirds of CPPs use the Internet as a medium to obtain information related to drugs and diseases. In several prior studies conducted in Nepal, it has been stated that participants of the study use the Internet significantly to search for information.32–34 The findings of this study were similar to published studies conducted in Saudi Arabia, where social media was the primary source of information.35–37 A decade ago, the Current Index of Medical Specialties (CIMS) used to be the primary source of drug information available at community pharmacies. 30 The possible reason is due to the increasing number of mobile phones and easy access to internet among the CPPs, which may lead to the maximum use of the internet for obtaining information on drugs and diseases. During the time of the pandemic, there is a high chance of misinformation and false news. So, it is necessary to provide quality information to patients or healthcare professionals. Pharmacists play an important role in providing quality information about diseases and medications. We found that there is a shift to social media and applications due to easy access to mobile phones and the Internet. The augmented usage of smartphones and various medical apps by healthcare professionals, especially community pharmacists, might help in disseminating information during the pandemic. 38
COVID-19 is a global threat, and all pharmacists working in different sectors such as clinical, hospital and community settings have a crucial role to play. Community pharmacists can improve the well-being of their patients/consumers by upgrading their knowledge and skills about the disease management process. To improve their role in this global threat, community pharmacists can provide information to the patients or patients’ caregivers or community on COVID-19, including management approaches, psychological counselling and advice, home care and safety approaches, drug–drug interactions and adverse drug reactions, and medical management of chronic comorbid illnesses, such as diabetes, hypertension, asthma and so on. Furthermore, CPPs can liaise with drug information centres, national health authorities and organizations to improve the use of information services provided by them.20,39
Ministry of Health and Population Nepal (MOHP) 40 is also posting COVID-19 occurrence updates and resource materials. Similarly, WHO is providing situation reports regarding COVID-19 for the public, doctors and healthcare professionals.3,6,41 FIP, which is an organization of pharmacists, has also published resource materials for community pharmacists. 19 Simultaneously, it sets extraordinary responsibilities on healthcare authorities and regulatory authorities to expand the accessibility of such resource materials by offering various methods for information delivery, expecting to improve knowledge, awareness and preparedness levels. These educational courses can be vital for providing information and statistics to individuals, community, public and healthcare professionals. In the same way, virtual (online) seminars, online training and courses can also be useful in educating and raising alertness about COVID-19 and other emerging infectious diseases.
There was a significant difference between the knowledge scores of people with experience of less than 1 year and more than 5 years. It is understood that the year of experience influences the knowledge of individuals. In this case, probably they are likely to seek more information from others and also update themselves from available resources such as the Internet, newspapers and so on. 42 CPPs with greater work experience may have better experiential knowledge. Experiential learning emphasizes hands-on experience and real-world situations. 43 Their better experiential knowledge may have accounted for their higher scores. Las Vergnas has expanded on the work of Carl Rogers and mentions that patients live with their illnesses every day and are experts concerning their own experience of illness. Healthcare practitioners, like CPPs, should welcome and value the patients’ experiential knowledge. 44
Similarly, a significant difference was noticed between the CPP in the pharmacies close to the hospitals and far away from the hospitals. The reason could be related to the series of communications happening among the hospital staff on COVID-19 and its seriousness. There was a significant difference in the preparedness score between the CPPs working for less than 1 year and CPP working 1 to 5 years. The probable reason for this influence of years of experience is the fact that longer work experiences prepare individuals to handle any adverse situations such as the COVID 19 pandemic. Similarly, CMA was found to be more prepared than diploma pharmacy and Bachelor in pharmacy. CPPs working at pharmacies with more than 1000 medicines were found to be more prepared than that of those who work in pharmacies with less than 500 medicines. The reason could be the same as we discussed during the awareness section. Preparation and cooperation among healthcare professionals and sectors should be a significant experience to be learned from COVID-19. 42
Community pharmacies are located near to the public and are easily accessible especially during the pandemic as people are afraid to travel to hospitals for minor signs and symptoms. CPPs have different roles such as providing information regarding COVID-19, early case identification, encouraging screening, education on face mask wearing, social distancing and so on. According to FIP, community pharmacies play a crucial role in preventing the spread of COVID-19. 19
The study by Basheti et al. 45 found that there was a significant role for pharmacies in the management of epidemics/pandemics. Similarly, the study conducted at Macau showed the importance of community pharmacists who was given the responsibility of early identification of COVID-19 and patient referral to the hospital. They were also provided with the accountability of supply of medicines, the transmission of information to the community concerning the local condition of disease, whole infection development and methods for personal fortification and inhibition of the transmission of COVID-19. 22 Similarly, other studies have also highlighted that community pharmacies and CPPs have a crucial role in the health system’s response to the management of the pandemic.46–48 Community pharmacists have essential roles such as informing, advising and educating the patients visiting the community pharmacies and the community. Community pharmacists also have an essential role in maintaining a constant supply of medications and individual cleanliness goods. 21
In our perspective, the findings of this study may contribute to identifying educational interventions, which may help policymakers and regulatory authorities such as the MOHP, DDA, NPC and other health and infectious diseases authorities in understanding the usefulness and importance of CPPs at the time of the pandemic or any other infectious diseases. In addition, the outcomes of this study may also contribute to planning, developing and strengthening intervention programmes to maintain the health of susceptible individuals.
Limitations
The study has certain limitations, which must be acknowledged. First, the study was conducted only among CPPs working in community pharmacies of Kathmandu district and did not represent the pharmacy practitioners working at different settings such as a hospital or clinic or industries. Second, the small sample size might not be suitable for generalization. There might have been biases in the study since the study depended on a self-completed survey, self-informed records and self-perception. The investigators interviewed 81 CPPs from different pharmacies when there were 2430 retail pharmacies as per official publication by the DDA. With eight pharmacies as the sampling interval, using a convenience sampling method, authors should interview at least 304 community pharmacies in this study.
Nevertheless, due to sudden lockdown by the government of Nepal and to maintain social distancing, it was not possible to interview 304 community pharmacies, and we had to stop after completing 81 pharmacies. The third limitation is the methodology which can be biased, as many recent studies have demonstrated that the use of mixed methods (qualitative and quantitative) study is more relevant. The study was carried out only at community pharmacies dispensing allopathic medicines. The fourth limitation of this study was that we only studied community pharmacies, which were registered in DDA.
In addition, this study was done at a time when there was only one case reported in the country. Probably, now the existing scenario may be different from the time when the study was conducted. As of now, there are more cases in the country and globally, and hence the scenario may be different.
Recommendations
Based on the findings of this study, several recommendations could be made to increase awareness among CPPs. Studies evaluating pre- and post-study knowledge with educational interventions are recommended to further enhance the community pharmacists’ knowledge on COVID-19, a significant public health emergency faced by many countries. Since this study was a pilot study, it could not include pharmacists employed in diverse pharmacy settings such as hospital pharmacy settings and clinical pharmacy settings. In future, their knowledge, awareness and preparedness can be assessed.
Conclusion
The preliminary findings of this study showed that the knowledge was found to be higher in CPPs with an experience of more than 5 years. Similarly, the CPPs working at bigger community pharmacies are found to be more aware and prepared. Educational interventions can improve knowledge, awareness and preparedness scores.
Supplemental Material
sj-pdf-1-smo-10.1177_1234567891011122 – Supplemental material for Knowledge, awareness and preparedness regarding coronavirus disease 2019 pandemic among community pharmacy practitioners working in Kathmandu, Nepal: A pilot study
Supplemental material, sj-pdf-1-smo-10.1177_1234567891011122 for Knowledge, awareness and preparedness regarding coronavirus disease 2019 pandemic among community pharmacy practitioners working in Kathmandu, Nepal: A pilot study by Sunil Shrestha, Nisha Jha, Subish Palaian and Pathyil Ravi Shankar in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Mr. Ranish Shrestha (Infection Control Unit, Nepal Cancer Hospital and Research Center) for his guidance during the development of the questionnaire. The authors would like to acknowledge Ms. Yunima Sapkota, Mr. Ram Prasad Shrestha and Mr. Ramesh Bhasima for their assistance in the data collection. The authors would also like to thank Institutional Research Committee (IRC) of KIST Medical College, Gwarko, Lalitpur, Nepal, for expedited review of the proposal for ethical approval, and they wish to thank all the respondents of this study who actively participated and gave up their precious time.
Author contributions
S.S., N.J., S.P. and P.R.S. conceived, designed the study, and finalized the methodology and tools used for the data collection. S.S. did pilot testing of the developed tools and N.J. assisted data collector while collecting data. S.S., S.P. and P.R.S. analysed the data and drafted the manuscript. All the authors made significant contributions to writing the manuscript and reviewing the literature. The final manuscript has been read and approved by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Before starting the study, ethical approval for this study was obtained from the Institutional Research Committee (IRC) of KIST Medical College and Teaching Hospital, Lalitpur, Nepal (Ref. 2076/77/37).
Informed consent
Written informed consent was obtained from all subjects before the study from individual respondents.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.